Before 1987, a notation of a severe substance-related syndrome (e.g., dependence) in most diagnostic systems required evidence of tolerance or withdrawal. However, this approach created a number of dilemmas in which clinicians were unable to apply an appropriate label to some patients despite important levels of life impairment related to substances. These problems led the framers of DSM-III-R to consider a broadly defined syndrome in which dependence is seen as a complex process that reflects the central importance of substances in an individual’s life, along with a feeling of compulsion to continue taking the substance and subsequent problems controlling use
(1–
3). Here, tolerance and withdrawal were seen as potentially important, but not central, aspects of a substance dependence diagnosis. However, despite what might be viewed as an important paradigm shift in diagnosing substance use disorders, there are few data available to test the meaning of these changes.
At least two types of studies are required to draw conclusions regarding the clinical implications of the diminished emphasis on physiological aspects of dependence. As reviewed in a recent article, the more impressive data require large-scale prospective studies to determine whether a physiological component of dependence predicts a more severe clinical course
(4). Unfortunately, only two relevant studies have been published, with the first reporting data in a subgroup of 94 cocaine-dependent individuals
(5). Results indicated that on the basis of Sommer’s D statistic, a past history of tolerance was moderately related with Addiction Severity Index ratings of employment problems (0.20), social impairment (0.27), and psychiatric severity (0.25), whereas a past history of withdrawal or withdrawal avoidance was most strongly associated with psychiatric severity (0.42). However, for many Addiction Severity Index outcome ratings, other DSM items related at least as well to outcome as tolerance or withdrawal
(5). The other follow-up study reported the relationship between each of the seven DSM-IV dependence items and the outcome for 375 successfully evaluated of 521 subjects who reported at least one DSM-IV problem (not full dependence) for alcohol, cocaine, opiates, amphetamines, sedative-hypnotics, or cannabinols
(6). While few details were offered, the authors concluded that neither tolerance nor withdrawal stood out among the DSM-IV criteria items regarding their ability to predict a more severe outcome as measured by the Addiction Severity Index.
The second type of study compares cross-sectional evaluations of dependent subjects with and without a physiological component. Regarding cocaine-dependent subjects, a study by Rounsaville and Bryant
(5) provided evidence that physiological components were not superior to other DSM-III-R symptoms in assessing severity. In addition, the cross-sectional component of the second study did not support the conclusion that either tolerance or withdrawal was a unique indicator of severity relative to other criteria
(6).
Our group has previously described a cross-sectional and retrospective analysis of data from 3,395 personally interviewed alcohol-dependent individuals
(4). That study demonstrated that 86.9% of those alcoholics reported experiencing withdrawal, tolerance, or both regarding alcohol; almost half (48.7%) of these noted tolerance alone. Those with tolerance or withdrawal reported a larger maximum number of drinks per day (30 versus 18), were more likely to have experienced two or more continuous days of drinking while giving up responsibilities (58% versus 21%), and noted a twofold or higher increase in the number of alcohol-related physical and psychiatric problems. Those subjects with histories of withdrawal reported the most severe difficulties. These results are supported by a latent class analysis which showed that while both tolerance and withdrawal contributed significantly to the alcoholic classification, subjects with withdrawal had a more severe course
(7).
The findings reported earlier in this article raise a number of questions that are addressed in the present study. First, is the prior history of substance-related problems more severe for individuals with physiological aspects of the dependence syndrome for drugs other than alcohol? Second, does the evidence support the conclusion that a physiological component is best defined rather broadly by including tolerance or withdrawal or both, or should a more narrow definition requiring evidence of withdrawal be used?
METHOD
The data were generated from subjects who took part in the six center-wide Collaborative Study on the Genetics of Alcoholism. This is a family pedigree study that begins with an alcohol-dependent proband in treatment and gathers data from that subject and all available appropriate relatives
(4,
7–
10). Subjects in the Collaborative Study on the Genetics of Alcoholism sample were included regardless of additional diagnoses, with the only exclusions occurring for individuals who were unable to speak English, those with evidence of severe debilitating diseases such as AIDS, those with recent heavy intravenous drug use, and subjects who had fewer than two relatives available for interview. Comparison subjects were selected from a variety of sources including general medical and dental clinics, drivers’ license records, and random population surveys. After a full explanation of the procedures, appropriate subjects gave written informed consent to participate. Probands, comparison subjects, and their relatives who at some time in their lives met DSM-III-R criteria for dependence on at least one drug including marijuana, cocaine, amphetamines, and opiates were included in the present analysis. Many of these subjects also had alcohol dependence and were included in the companion paper
(4).
A structured face-to-face interview, the Semi-Structured Assessment for the Genetics of Alcoholism
(9), was given to all subjects. This instrument screens for 17 axis I DSM-III-R diagnoses, including abuse and dependence on substances. A separate section of the Semi-Structured Assessment for the Genetics of Alcoholism reviews items relating to the patterns of marijuana use and problems, including tolerance and withdrawal. Another section assesses the patterns of use of cocaine, amphetamines, and opiates, as well as 14 problems related to the heavy use of these drugs, including tolerance and withdrawal.
In order to test the correlates of a physiological dependence syndrome as suggested by DSM-IV, for each drug separately those individuals with dependence were placed into three groups on the basis of their endorsement of several items at some time during the course of their drug dependence. Group 1 membership, indicating a more narrowly defined physiological dependence, required at least one episode of withdrawal for that drug as defined in DSM-III-R, including at least two of seven relevant withdrawal symptoms for marijuana, six for cocaine or amphetamines, and 13 for opiates, or use of a substance to avoid or relieve withdrawal symptoms. Subjects in group 2 reported they had never experienced withdrawal or used substances to avoid withdrawal but endorsed tolerance, i.e., had needed 50% or more than the usual dose of the drug to get the same effect. Group 3 consisted of individuals who, while dependent on that drug, experienced neither tolerance nor withdrawal.
The present report contains three sets of analyses, looking at each of four drugs separately. For each, chi-square tests (with Yates’s corrections) were applied to categorical data across groups, while F or two-tailed t values determined the significance of differences in group means for continuous variables. If the overall group differences were significant, these were followed by Tukey’s honestly significant difference post hoc test of pairwise comparisons. In addition, the potential clinical implications of a broader definition of a physiological component of dependence were evaluated by comparing the combined groups 1 and 2 to group 3; the meaning of a narrower definition was tested by comparing group 1 with groups 2 and 3 combined. A logistic regression analysis was used to determine the potential influence of those variables significant at the univariate level in predicting physiological dependence, with control for the influence of all of the other predictors. Finally, because of the large numbers of subjects involved in some of the analyses, the magnitudes of the effect sizes (small, medium, or large) are indicated in the tables according to the method of Cohen
(11), indicated by d for Student’s t test and w for chi-square.
RESULTS
Among the 8,995 subjects in the Collaborative Study on the Genetics of Alcoholism sample, 2,143 (23.8%) met criteria for dependence on at least one relevant drug at some time in their lives. In this group, 49.8% were dependent on only one of the four drugs, 31.5% on two, 13.3% on three, and 5.4% on all four drugs. The sample included 784 probands (36.6%), 1,299 relatives of probands (60.6%), and 60 dependent comparison subjects (2.8%), with a total of 797 women (37.2%), and was composed of Caucasian (69.1%), African American (20.3%), and Hispanic (7.1%) subjects, as well as subjects from other ethnic backgrounds (3.5%). The mean age was 33.3 years (SD=7.7), and participants reported an average of 12.4 years of education (SD=2.0). At the time of the interview, 55.4% were married or living as married, 27.3% were separated or divorced, 1.0% were widowed, and 16.3% had never been married and were living alone.
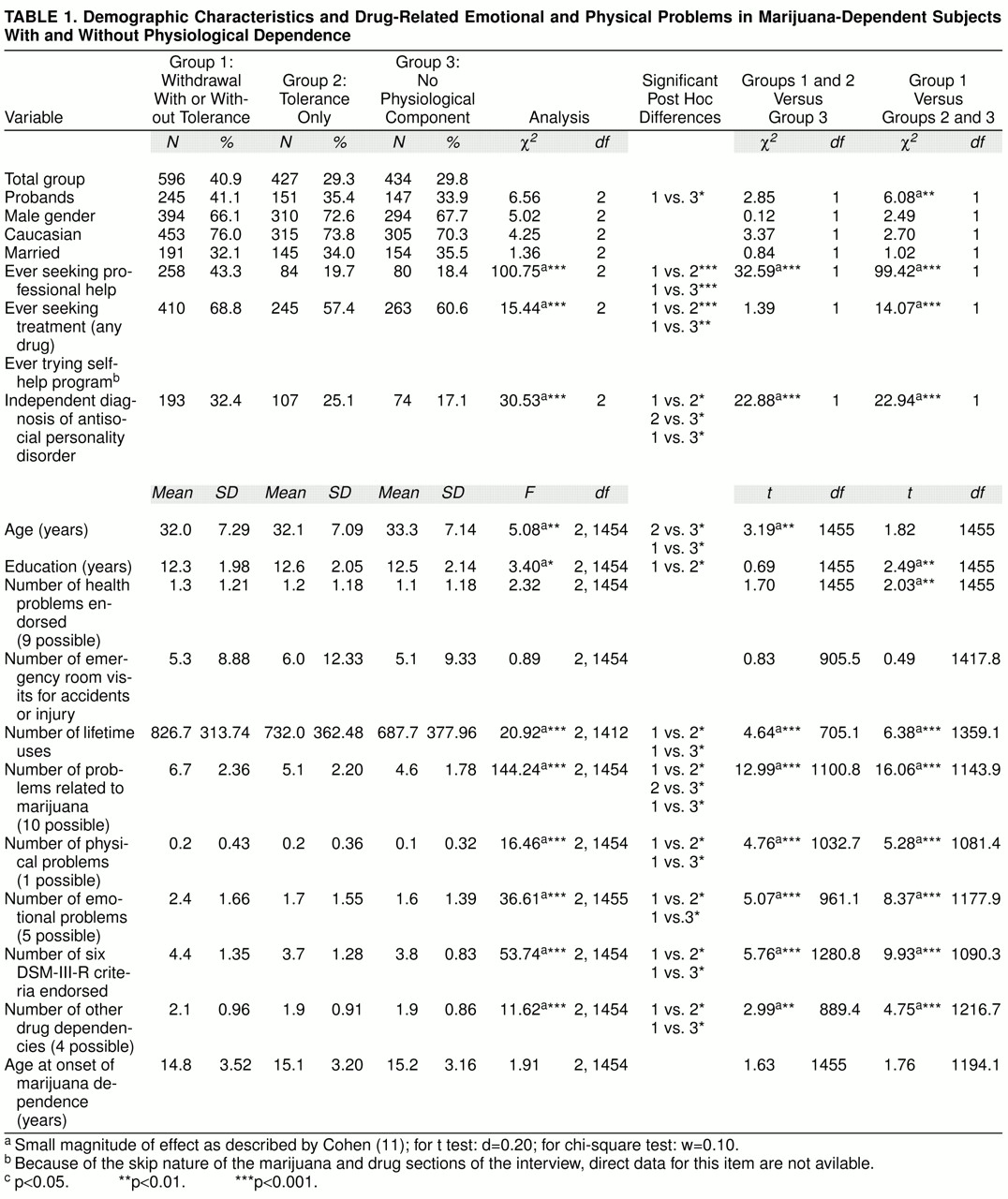
Table 1 compares the three groups among those individuals who fulfilled criteria for marijuana dependence. More than one in four (29.8%) reported no evidence of tolerance or withdrawal, while about 40% related histories of symptoms consistent with withdrawal from that substance (group 1). Inspection of the table reveals few significant differences in demography across the groups, although there were some small differences in age and education.
Despite these demographic similarities, both the narrower (group 1) and broader (group 1 and group 2) definitions of a physiological component of dependence were associated with more severe problems and heavier intake of marijuana, compared to those without a physiological component (group 3). For most items, group 1 subjects demonstrated higher levels of substance involvement and problems than did group 2. The substance-related problems here and in the following tables excluded those observed only in the context of withdrawal.
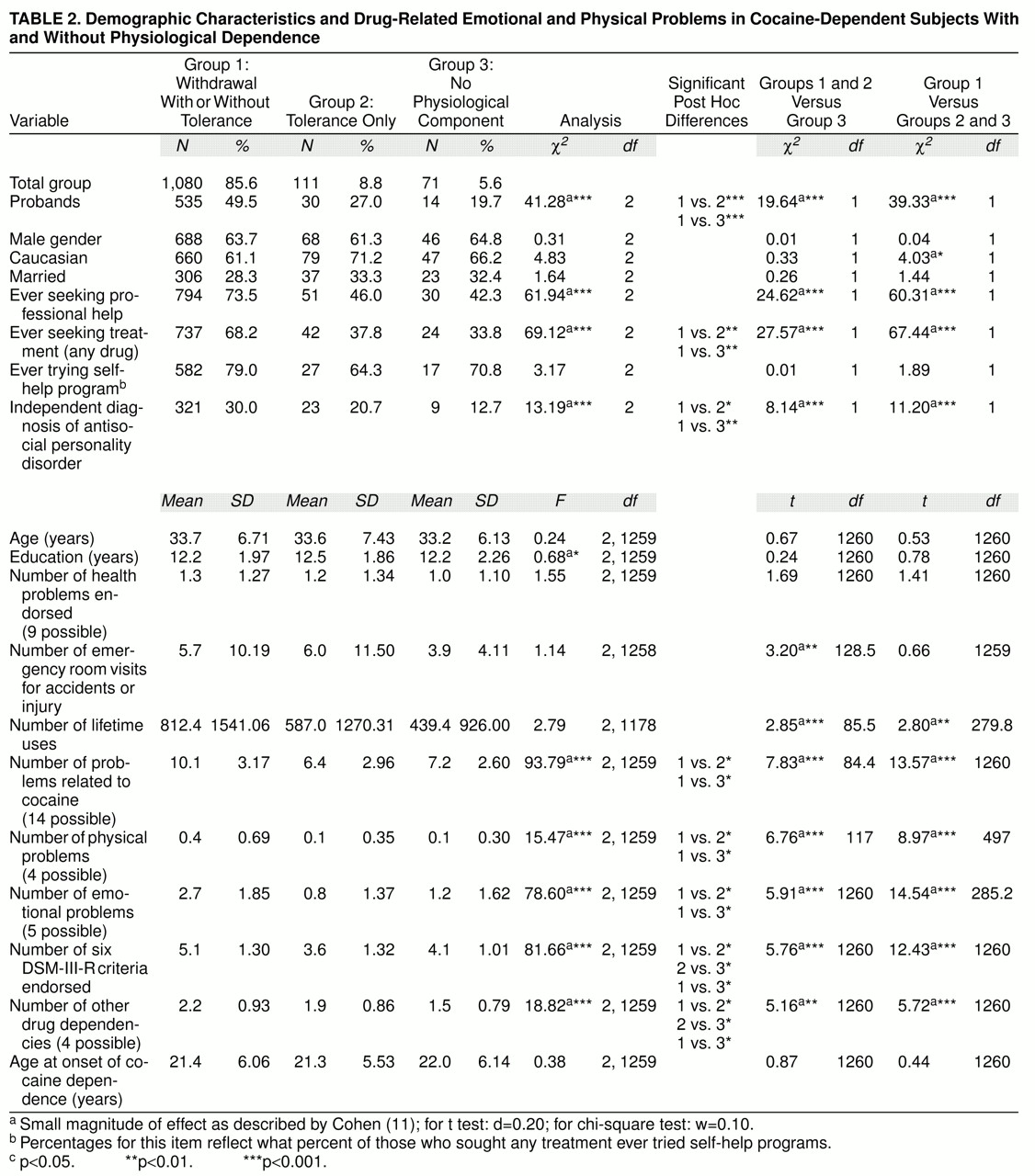
Table 2, structured similarly to
table 1, focuses on the subjects who had ever fulfilled criteria for cocaine dependence. Here, few denied ever having experienced tolerance or withdrawal, with the large majority fulfilling criteria for group 1 (withdrawal). With the exception of the proportion of subjects who were original probands and a small difference in education, the three groups were similar in demography and medical histories. However, the most severe clinical course was reported by group 1 individuals. The only characteristic for which group 2 demonstrated significantly more problems than group 3 was the number of additional drug dependencies.
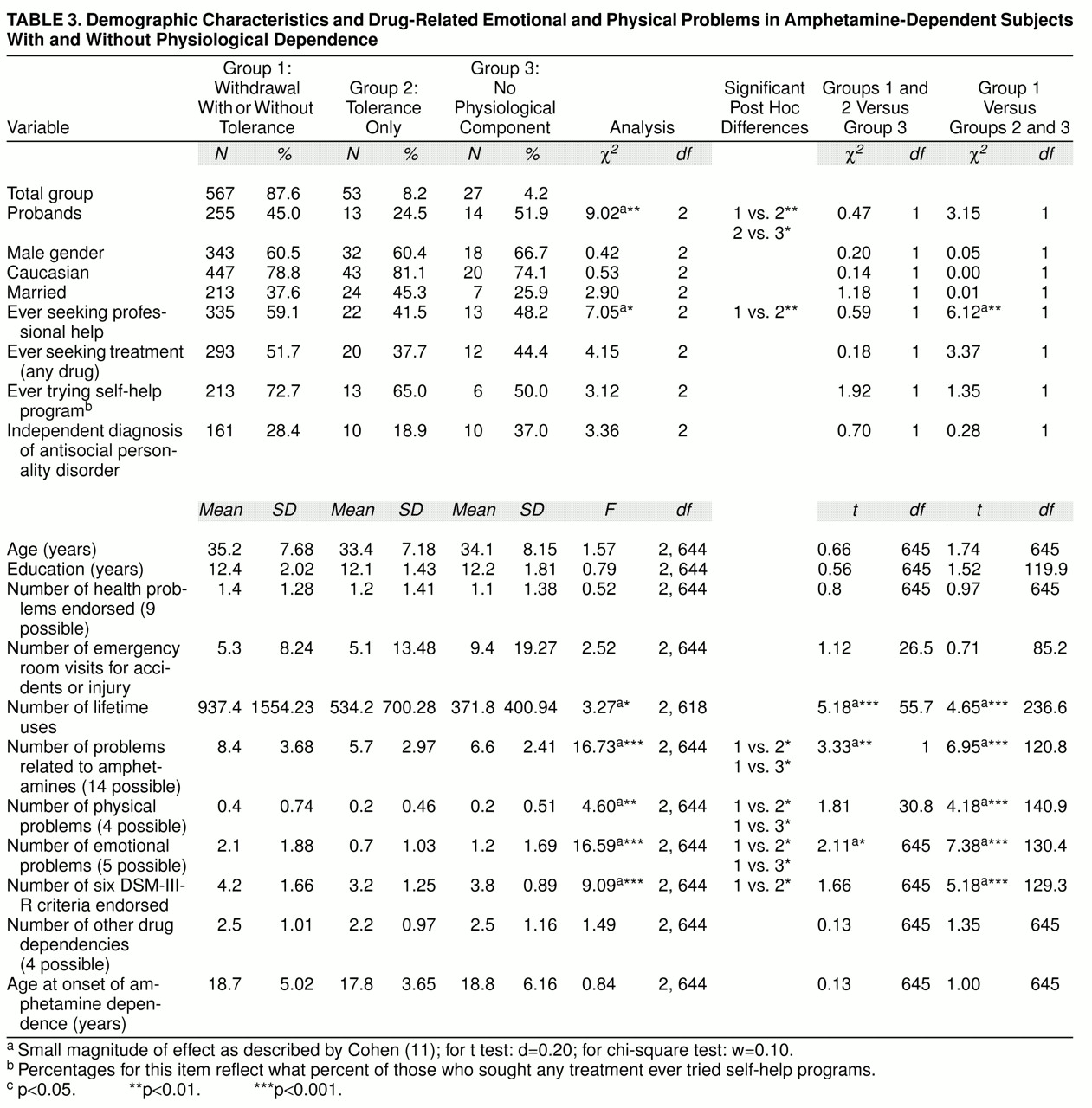
The data in
table 3, focusing on amphetamine-dependent subjects, reveal a relatively small proportion who denied a physiological component (4.2%), and over 87% noted a history of withdrawal. Except for the proportion of probands, the three groups were similar in demography and general physical health histories, but the most severe problems were observed for group 1 subjects. Those reporting tolerance alone were more similar to group 3 than to group 1.
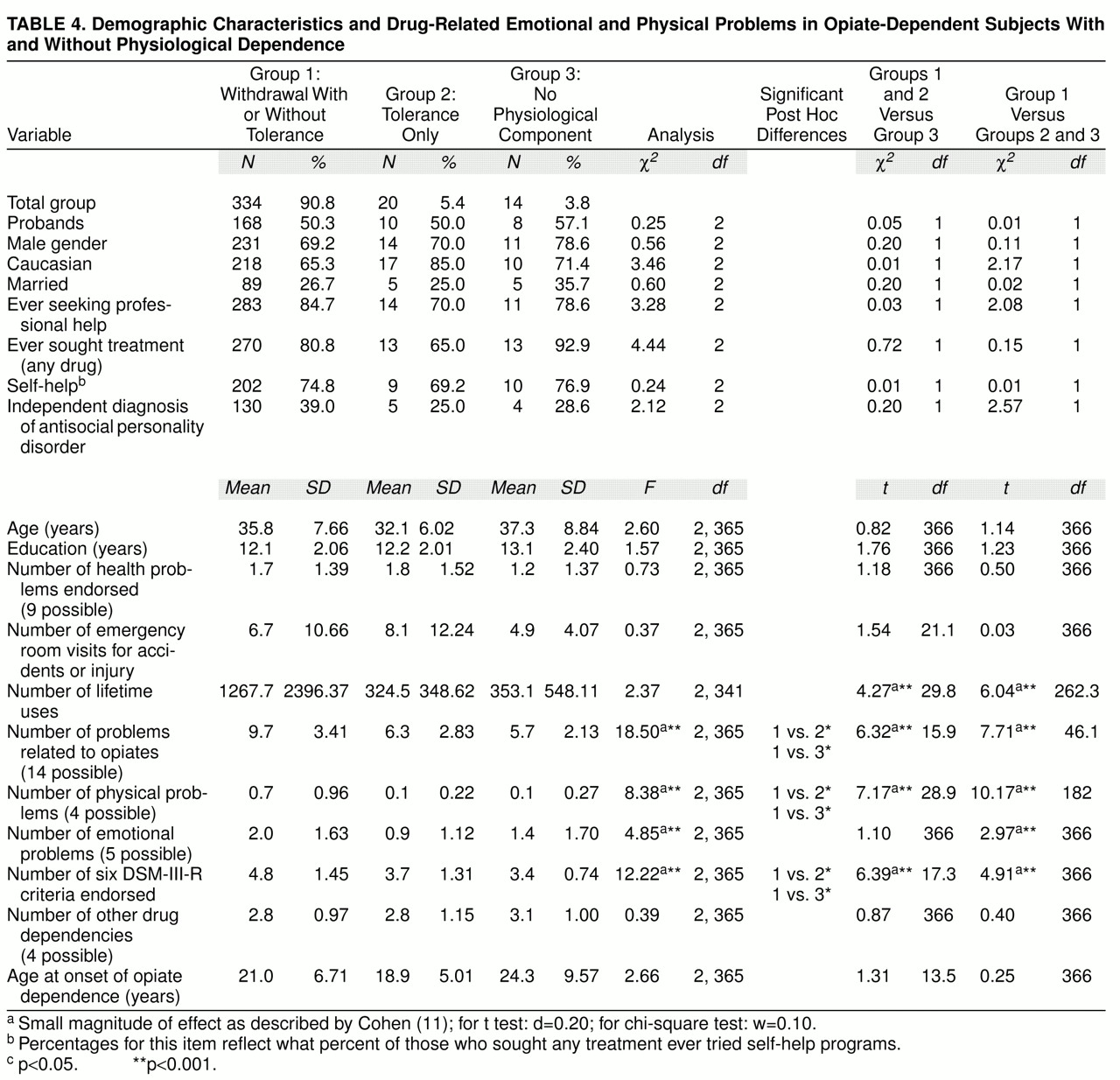
Finally,
table 4 offers similar information for the subjects with histories of opiate dependence. Only a small proportion denied tolerance or withdrawal, and the large majority reported withdrawal. Even though the size of group 3 makes it difficult to draw conclusions, the data in
table 4 generally support results from the prior three tables. Once again, the three groups were similar in demography and overall medical problems, but subjects in group 1 stand out as having the most severe clinical course.
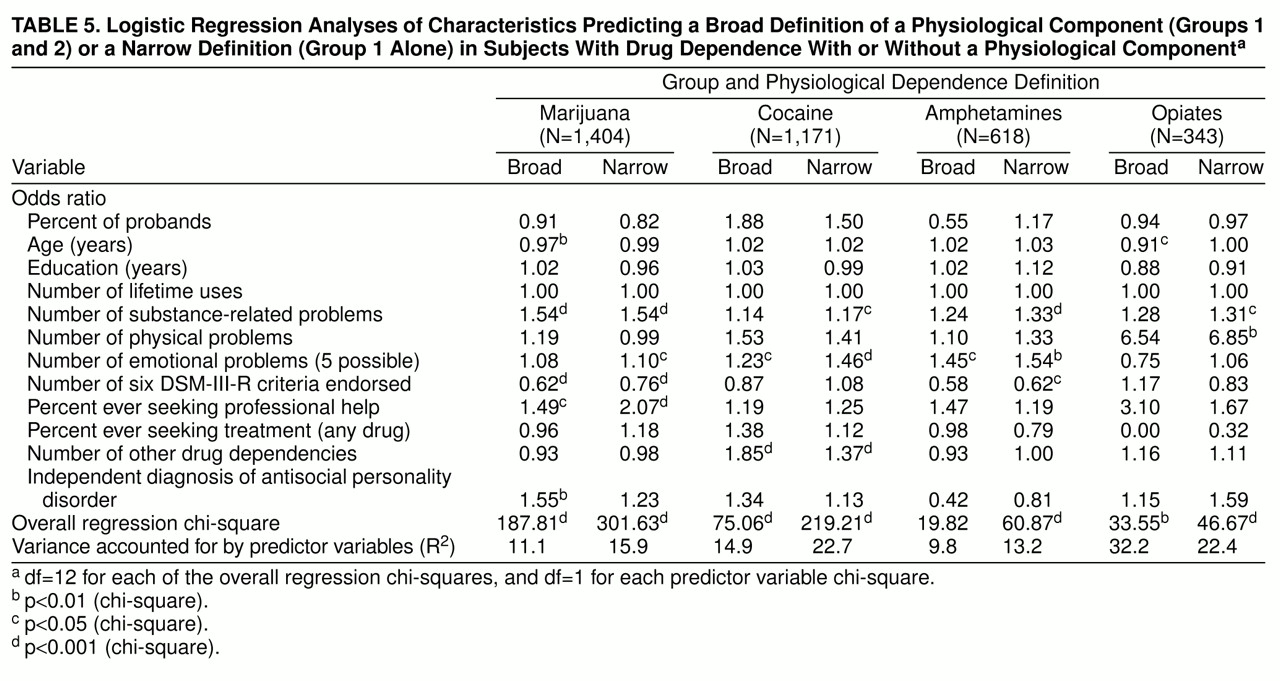
The data in tables 1–4 do not clarify which of the clinical correlates of physiological dependence remain robust when considered in the context of the others, nor do the univariate analyses of group differences take into account the impact of antisocial personality disorder, a diagnosis most common in group 1. Therefore, in
table 5 all variables that significantly differentiated across the three groups in tables 1–4, and those that added significantly to the logistic regressions in the alcohol study
(4), were entered as predictors of the broad definition of a physiological component of dependence (i.e., group 1 and 2 membership) in logistic regression equations carried out separately for each of the four drugs, and as predictors of the more narrowly defined withdrawal (group 1). The number of subjects for each substance is slightly lower than that presented in tables 1-4 because the logistic regression requires that complete data be available on all variables for all subjects.
Beginning with marijuana, five items significantly contributed to the prediction of the broadly defined physiological dependence, generating an equation with an overall chi-square of 187.81 (df=12, p<0.001), explaining 11.1% of the variance. The items that entered the equation reflected the pattern of problems, a diagnosis of antisocial personality disorder, and age, as well as the proportion of individuals seeking professional help. The odds ratios associated with each of these items were in the predicted direction, except for the number of DSM-III-R items endorsed, in which case a suppressor variable operated to reverse the direction of the relationship.
Focusing on the 1,171 subjects with cocaine dependence who were appropriate for that analysis, for the broad definition of a physiological component the overall chi-square was 75.06 (df=12, p<0.001), which explained 14.9% of the variance. Significant predictors included the number of additional drug dependencies (the only drug for which this was true) and the number of the five possible emotional problems endorsed. Regarding the predictors of the broad definition of dependence on amphetamines, the overall chi-square was 19.82 (df=12, n.s.), with only one item (the number of emotional problems endorsed) entering the equation at a significant level. Despite the small number of individuals with opiate dependence (only 12 with complete data had experienced neither tolerance nor withdrawal), the logistic regression for those drugs was significant, explaining 32.2% of the variance, although only one item, age, functioned as a significant predictor.
The same analyses were also carried out for the more narrow definition of a physiological component that requires evidence of withdrawal. Beginning with marijuana, three of the five items from the broad definition were significant, with the remaining two still operating in the same direction. A new item entered the equation (the number of emotional problems), and there was a larger overall chi-square (301.63, df=12, p<0.001) and more explained variance (15.9% versus 11.1%) compared to when the broad definition was used. For cocaine, the same items as for a broadly defined physiological dependence operated as predictors, with the number of substance problems also reaching significance. The overall chi-square was 219.21 (df=12, p<0.001), and 22.7% of the variance was explained, compared to 14.9% for the broad physiological syndrome. For amphetamines, two additional variables (the number of substance-related problems and the number of DSM-III-R criteria items endorsed) entered the equation, with a larger chi-square (60.87, df=12, p<0.001) and a larger proportion of the variance explained, compared to the broad physiological concept. The overall chi-square for the logistic regression related to opiate dependence was 46.67 (df=12, p<0.001), with the number of substance-related problems and number of physical problems functioning as significant predictors.
An additional analysis was carried out to determine the applicability of the logistic regression findings to a potentially important subgroup. To evaluate whether these results were merely a reflection of the fact that some subjects were genetically related, the logistic regressions reported in
table 5 were repeated, but for probands only (a group of unrelated subjects). Results indicated that similar predictors were operating.
DISCUSSION
These cross-sectional and retrospective data demonstrate that for all four drugs, both broad and narrow definitions of a physiological component to dependence identified groups with more severe substance problems. Although the specific items differed a bit across drugs, they consistently indicated a pattern of higher levels of substance intake and evidence that a broad array of substance-related problems was associated with a physiological component that required a history of withdrawal syndrome.
This greater intensity of problems for group 1 and/or group 2 is not explained simply by a history of antisocial personality disorder or by demographic characteristics. Although the proband status did significantly differ across groups in some of the analyses, the other indicators of severe substance-related problems still operated in the logistic regression analyses in the context of the proband condition. Finally, data from
table 5 demonstrate that the results were not likely to reflect only dependence on other drugs.
The present results are similar to those in our companion paper focusing on alcohol dependence
(4) and resemble the conclusions from the latent class analysis
(7). The present data, however, differ from those in several other reports
(5,
6). Both of the earlier studies carried out most analyses on people who met only one or more dependence criteria for a drug (not necessarily the full syndrome), and both assessed severity with the Addiction Severity Index. This index provides a global measure of impairment in six domains generally affected by drugs, alcohol, or both, whereas this study used the Semi-Structured Assessment for the Genetics of Alcoholism, a more detailed and intensive evaluation of the clinical course. It is possible that more concordant results would have been obtained if similar diagnostic criteria and measures had been used in all the studies.
Tables 1–5 indicate that for each of the drugs the self-report of an experience of a withdrawal syndrome was associated with more severe problems than tolerance alone. Thus, these data highlight the potential benefits of redefining physiological dependence to demand evidence of withdrawal. The absence of impressive differences between groups 2 and 3 is consistent with the findings from the study on alcohol
(4).
It is possible to speculate about why tolerance did not work as well as withdrawal in distinguishing the clinical course for the substances tested. It may be that tolerance and withdrawal, despite some similarities, have a number of different underlying mechanisms
(12,
13). In addition, withdrawal is based on more dramatic and perhaps more reliably reported symptoms than is tolerance, a characteristic that could be important when establishing a history of the phenomena retrospectively. Finally, the problem with tolerance in this context might relate to the definition used, where, for example, a 50% increase in the amount of the substance needed for an effect might be a relatively low threshold.
As with any study, there are methodological limitations. First, additional analyses will be needed to see if other combinations of items from DSM-III-R or DSM-IV would better identify a subgroup with a more severe course. Second, these cross-sectional analyses offer no information regarding the future clinical course among drug-dependent individuals. Third, even though the number of drug dependencies did not contribute significantly to most logistic regression analyses, it is possible that for subjects dependent on more than one drug, retrospective reports of withdrawal symptoms could be altered by a possible confusion across the different substances. Fourth, the data are limited to the substance dependencies most frequently reported in the Collaborative Study on the Genetics of Alcoholism sample, although these do represent the type of drugs most closely related to tolerance, withdrawal, or both. Some unique aspects of the Collaborative Study on the Genetics of Alcoholism sample, including the genetic relationship between members of the same family, also limit the generalizability of the present results, although the results appeared to hold even when unrelated probands were evaluated.
ACKNOWLEDGMENTS
The Collaborative Study on the Genetics of Alcoholism (H. Begleiter, State University of New York, Health Sciences Center at Brooklyn, Principal Investigator; T. Reich, Washington University, St. Louis, Co-Principal Investigator) includes six different centers where data collection takes place. The six sites and principal investigators and co-investigators are Indiana University (J. Nurnberger, Jr., T.-K. Li, P.M. Conneally, H. Edenberg); University of Iowa (R. Crowe, S. Kuperman); University of California at San Diego and Scripps Institute (M. Schuckit, F. Bloom); University of Connecticut (V. Hesselbrock); State University of New York, Health Sciences Center at Brooklyn (H. Begleiter, B. Porjesz); Washington University (T. Reich, C.R. Cloninger, J. Rice).