As Weygandt noted in 1899
(1), cognitive dysfunctions seem to be present in patients with bipolar disorder, both in clinical remission
(2) and in prodromic and residual phases
(3). Cognitive dysfunctions appear to increase in proportion to the length of illness
(4) and to be correlated to midsagittal magnetic resonance imaging brain size in patients with bipolar disorder who have psychotic symptoms
(2).
A poor level of insight has been described as a characteristic in patients with acute bipolar disorder
(5,
6). Awareness seems to grow only partially with clinical improvement
(6 and appears to diminish progressively with the repetition of episodes
(7).
A distinction between bipolar I and bipolar II disorder has been reported in terms of long-term diagnosis stability
(8), greater prevalence in family members of patients with bipolar II disorder, and the familial phenotypic homogeneity of bipolar II disorder
(9,
10). Studies of self-awareness phenomena and their neurofunctional correlates, however, have not considered the distinction. Therefore, the present study aims to evaluate awareness of illness in patients with either bipolar I or bipolar II disorder. We also investigated the presence of subjective cognitive disturbances in a phase of clinical stabilization.
METHOD
Fifty-seven outpatients were recruited consecutively at the Neurosciences Institute; 25 patients had bipolar I disorder, and 32 had bipolar II disorder (full or partial remission phases, according to DSM-IV criteria). All patients provided written informed consent. They were evaluated for clinical symptoms, insight, and basic cognitive symptoms. To avoid diagnostic uncertainties relating to diagnoses from the spectrum of schizophrenia, patients with bipolar I disorder who had mood-incongruent psychotic symptoms were excluded from the study.
At the evaluation, all of the patients were taking mood stabilizers (lithium, N=29; carbamazepine, N=10; valproate, N=7; lithium and carbamazepine, N=5; lithium and valproate, N=4; gabapentin, N=2). Twenty of the patients were women, and 37 were men; they ranged in age from 24 to 47 years (mean=33.9, SD=6.7); their mean length of illness at recruitment was 6.3 years (SD=3.5); their mean hospitalization duration was 2.6 weeks (SD=3.2); and their mean educational level was 10.8 years (SD=3.1). None of the patients had concomitant medical illnesses or were substance abusers.
Patients were interviewed with the Structured Clinical Interview for DSM-IV Axis I Disorders. The Brief Psychiatric Rating Scale (BPRS), the Hamilton Rating Scale for Depression, the Young Mania Rating Scale
(11), and the Social Adjustment Scale were administered for clinical assessment. The Structured Clinical Interview for DSM-IV Personality Disorders was used to evaluate comorbid axis II disorders. Four (16%) of the patients with bipolar I disorder (two borderline, one obsessive-compulsive, one dependent) and nine (28%) of the patients with bipolar II disorder (four borderline, two antisocial, two obsessive-compulsive, one histrionic) were given concurrent personality disorder diagnoses. The first three general items on the Scale of Unawareness of Mental Disorder
(12) were used; these items refer to the subject’s current awareness of mental disorder, utility of the therapy, and social consequences of the disorder. The scores on the Scale of Unawareness of Mental Disorder subscales are distributed on a 5-point scale on which 5=complete lack of awareness.
The Frankfurt Complaints Questionnaire
(13) was used for the self-evaluation of patients’ subjective experiences of cognitive disorder. Results on this measure were organized into four factorial dimensions: disorder of normal automatic processes, disorders of perceptual capacities, depression/anhedonia, and overstimulation.
Student’s t test (alpha=p<0.05, two-tailed) and chi-square tests were used to compare the two groups. Interrater reliability was verified by a series of independent interviews conducted by two of us (S.P. and L.Q.); reliability on the Scale of Unawareness of Mental Disorder achieved an interclass correlation value ranging from 0.76 to 0.89.
RESULTS
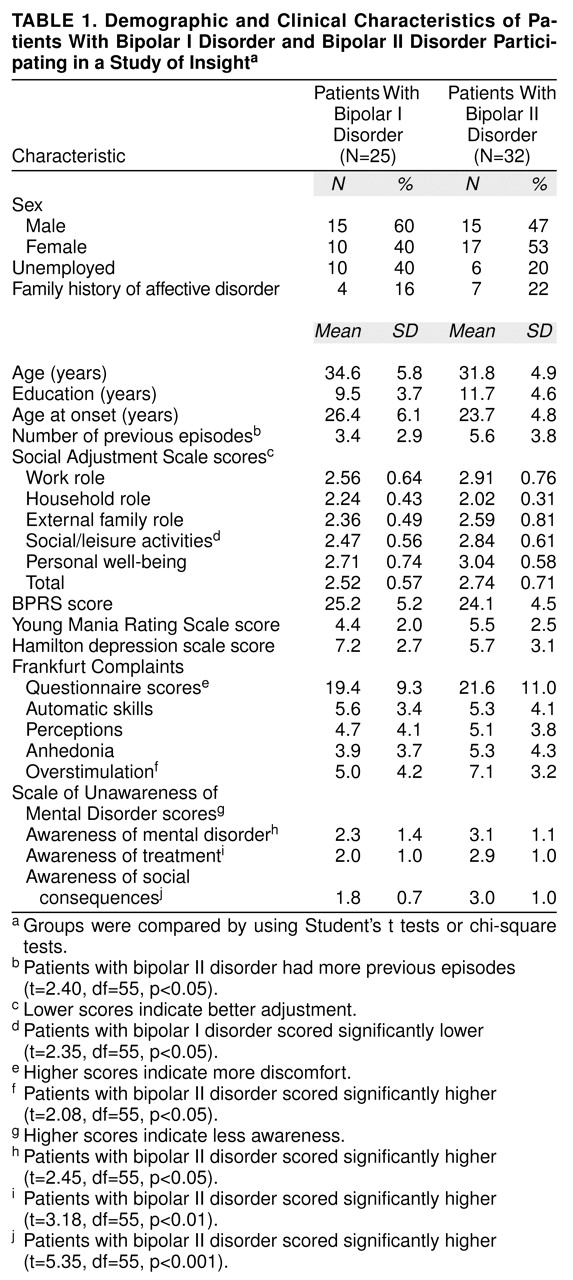
The mean BPRS score of all 57 patients was 24.7 (SD=4.9), their mean Young Mania Rating Scale score was 5.03 (SD=2.36), and their mean Hamilton depression scale score was 6.35 (SD=2.95). No significant differences were found between patients with bipolar I and bipolar II disorder regarding these three scales (BPRS: t=0.84, df=55, n.s.; Young Mania Rating Scale: t=1.79, df=55, n.s.; Hamilton depression scale: t=1.99, df=55, n.s.) (
Table 1). Neither did we find differences between groups in mean Frankfurt Complaints Questionnaire total scores, although the mean score on the overstimulation scale of the patients with bipolar II disorder was significantly higher than that of the patients with bipolar I disorder (
Table 1). Patients with bipolar II disorder also showed a poorer level of insight than the patients with bipolar I disorder according to scores on the three subscales of the Scale of Unawareness of Mental Disorder (
Table 1).
The patients with bipolar II disorder had a greater number of previous mood episodes than patients with bipolar I disorder, but there were no differences between the groups in unemployment rate, age, sex, or age at onset (
Table 1). Patients with bipolar I disorder showed a significantly higher level of adjustment to social/leisure activities measured with the Social Adjustment Scale, but no other significant differences were found in social adjustment (
Table 1). The patients with bipolar II disorder had a nonsignificantly greater rate of family history of affective disorder than the patients with bipolar I disorder (χ
2=0.3, n.s.) (
Table 1).
DISCUSSION
Patients with bipolar II disorder showed poorer awareness of their illness than patients with bipolar I disorder, although general impairment of awareness of illness was found in the whole study group. The latter finding is in agreement with other studies
(5,
6), which have found that although there appears to be a correlation between a reduction of insight and severity of clinical symptoms, the correlation is not as linear as one might expect. Our results complement those of Amador et al.
(12), revealing an impairment of insight in patients with primary mood disturbances.
Greater lack of insight might constitute a psychopathological characteristic that complicates the course of bipolar II disorder. Like subjects with bipolar II disorder in other studies
(14), our patients with bipolar II disorder also had a greater number of relapses and a higher rate of affective disorders in their families.
The lower level of awareness of social consequences of their illness among the patients with bipolar II disorder, even though this may be affected somewhat by the data showing greater employment, was associated with social adaptation that was in fact worse. However, the complex relationship among an elevated number of previous episodes, mood alteration, and reduced insight is not completely explainable on the basis of our data.
In reporting cognitive complaints, patients with bipolar II disorder reported a greater level of overstimulation than the patients with bipolar I disorder. The experience of overstimulation can be considered a multidimensional construct, interpretable both as a neuropsychological dysfunction and as a peculiar use of self-deception
(15) involving reduced awareness of having a disorder and a tendency to interpret their suffering as “friction” at the interface of internal rhythms and the environment
(16).
It remains to be documented whether the level of insight varies in relation to different phases of the illness or to other factors such as gender or comorbid disorders. It would be worth devoting greater attention to the possibility of considering self-awareness deficit as a course specifier.
Further investigations are needed to clarify the possible relationship of subjective cognitive complaints to objective neuropsychological cognitive evaluation in patients with bipolar II disorder compared with patients who have bipolar I disorder and other comparison groups.