Poor awareness of one’s own mental illness is an established feature in schizophrenia. In the International Pilot Study of Schizophrenia
(1), lack of insight was the most prevalent and second most discriminating symptom and was useful in subtyping divisions within schizophrenia. The problem of unawareness of abnormal movements in patients with schizophrenia who have tardive dyskinesia has not received much attention. Nonschizophrenic patients with abnormal movements (e.g., those with Parkinson’s disease) are usually aware of their movements. In addition, patients with mental disorders such as bipolar psychosis seem to be more aware of neuroleptic-induced movements than patients with schizophrenia
(2). Approximately 25% of patients with schizophrenia treated with neuroleptics develop the potentially serious side effect of tardive dyskinesia. Of those, 44% to 88% are not aware of their dyskinetic movements
(3,
4). Unawareness of abnormal movements and the subsequent lack of complaints may delay a diagnosis of tardive dyskinesia.
Previous studies of this phenomenon did not use validated scales and were subject to rater bias
(3,
5). Our a priori hypotheses were 1) that lack of insight into mental illness and lack of awareness of abnormal movements are aspects of the same dysfunction and 2) that unawareness of tardive dyskinesia is stable over time.
METHOD
Forty-three outpatients with a DSM-III-R diagnosis of schizophrenia (N=36) or schizoaffective disorder (N=7) were selected from a motor disorder clinic. A global dyskinesia score of 2 or more on the Maryland Psychiatric Research Center Involuntary Movement Scale
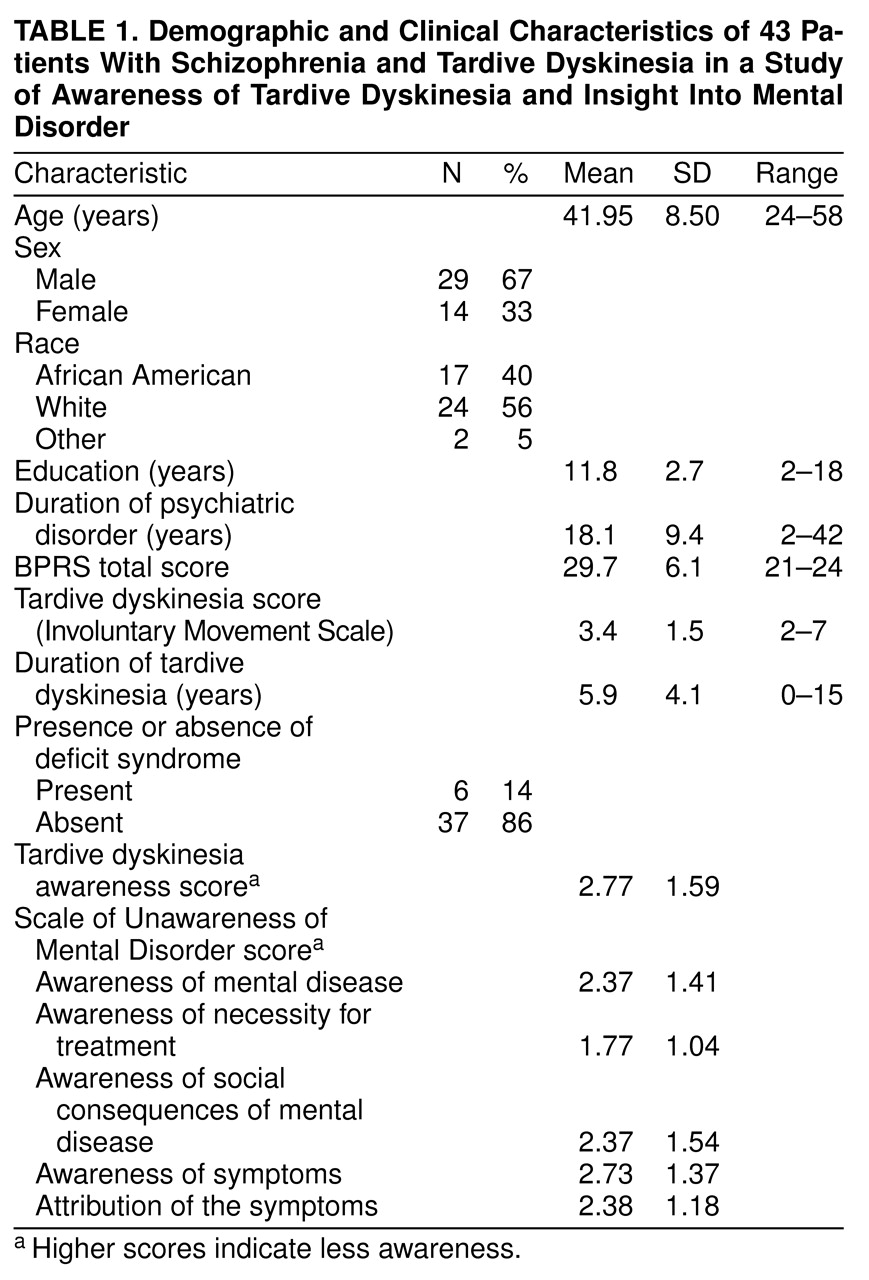
(6) was required. All 43 patients who met inclusion criteria agreed to participate and gave written informed consent before participating in the study. Their sociodemographic characteristics are shown in
Table 1.
The Brief Psychiatric Rating Scale (BPRS)
(7) was used to measure symptoms. Patients were grouped as having the deficit syndrome or not by using the Schedule for the Deficit Syndrome
(8). Twenty-one of the 43 patients were reevaluated 2 years after the first assessment. Of these patients, 16 still scored more than 2 on the Involuntary Movement Scale. Clinical and tardive dyskinesia ratings were obtained by the patient’s primary clinician.
Patients’ insight into their mental illness was measured by using the Scale of Unawareness of Mental Disorder
(9), which assesses varying degrees of insight in five different domains (
Table 1). Scores on this scale range from 1 (complete awareness) to 5 (complete unawareness). All patients were examined by a psychiatrist (C.A.) who was trained by the authors of the scale and had good reliability for the different constructs of the scale (intraclass correlation coefficient [ICC] range=0.79–0.95). The patients’ awareness of their tardive dyskinesia was assessed by a clinician who was blind to the patients’ insight into their mental disorder. The approach used to rate awareness of tardive dyskinesia was the same as that of the Scale of Unawareness of Mental Disorder. Because some patients may report that they have tardive dyskinesia or abnormal movements because they have been told so by others rather than because they were aware of the problem, special care was taken to rate the patient’s own awareness of the abnormal movements. A high interrater reliability was achieved for the awareness of tardive dyskinesia item as rated by two different raters for the first 20 patients (ICC=0.94).
Tests of the primary research hypotheses were conducted in a confirmatory framework. Specifically, Pearson’s correlation coefficients were used to assess relationships between awareness of tardive dyskinesia and continuous clinical insight dimensions. Differences in insight measures between patients with and without the deficit syndrome were assessed by using Student’s t test. Stability of awareness of tardive dyskinesia was evaluated by using intraclass correlation coefficients.
Exploratory analyses were conducted to examine possible relationships between awareness of tardive dyskinesia and sociodemographic, clinical, and tardive dyskinesia-related variables. A correlational approach (Kendall and Pearson’s) was used for these hypothesis-generating analyses.
RESULTS
Patients showed moderate insight into the different constructs of insight assessed. Their mean awareness ratings are shown in
Table 1. Awareness of tardive dyskinesia was not significantly related to any of the sociodemographic or clinical variables. Nor was awareness of tardive dyskinesia related to severity of dystonia, parkinsonism, or akathisia; body areas mainly affected; or number of years with tardive dyskinesia.
The six patients with the deficit syndrome showed significantly less awareness of tardive dyskinesia (mean score=4.2, SD=0.7) than the 37 patients without the deficit syndrome (mean score=2.6, SD=1.6) (t=–3.92, df=40, p<0.005). Groups did not differ in severity of tardive dyskinesia. Tardive dyskinesia awareness was not significantly related to scores on any of the BPRS subscales.
Awareness of abnormal movements and insight into mental disorder were significantly but only moderately correlated (Pearson r=0.35, df=42, p<0.05). Correlation of awareness of tardive dyskinesia with insight into social consequences of the mental disorder was significant (Pearson r=0.41, df=42, p<0.01). Correlations with the other three insight dimensions were not significant. Awareness of tardive dyskinesia was stable over time: ICC=0.76 for the index and 2-year follow-up assessments (N=16).
DISCUSSION
Almost half (46%) of these patients with schizophrenia had at least a moderate lack of awareness of their tardive dyskinesia, a smaller proportion than previously reported. Despite attending a motor disorder clinic with education programs, deficits in awareness of their dyskinesia did not improve over the 2-year period. To our knowledge, no previous study has evaluated long-term stability of awareness of abnormal movements.
The relatively low rate of lack of awareness in the current study may be due to recruitment of patients from a specialized motor disorders clinic. Furthermore, differences in insight evaluation methods may explain discrepancies between studies. Consistent with the findings of a previous study
(10), there was only a weak correlation between awareness of tardive dyskinesia and insight into mental illness. Anosognosia patients may be aware of the deficit in specific body areas and not in other areas or show awareness of memory deficits but lack of awareness of paralysis
(11). Similarly, patients with schizophrenia can be aware of some symptoms but not others.
Patients with the deficit syndrome were significantly less aware of tardive dyskinesia than were patients without the deficit syndrome. Relative lack of emotional responsiveness in general may explain this finding. Alternatively, the finding may be a manifestation of parietal lobe impairment, which has been implicated in the deficit syndrome as well as in awareness dysfunctions
(11,
12). One should apply caution when interpreting these findings because of the small number of patients in the study. There is insufficient power to declare a negative finding definitive. The power to detect a medium effect size for Pearson r=0.30 with 43 subjects and alpha=0.05 is only 0.51. Further studies with larger groups of patients are needed. Because all of the patients in our study were attending a motor disorder clinic, these findings may not be generalizable to other settings.
There are practical implications of these data. Clinicians cannot rely solely on patients to report dyskinetic movements. Regular, direct clinical observation is needed, and other caretakers, including patients’ relatives, may need to be educated to detect abnormal movements. Early detection of tardive dyskinesia may decrease exposure to the cause of the abnormal movements by leading to a lower dose or change in medication to a more benign drug.