There is a growing epidemiological and clinical literature documenting the frequent co-occurrence of substance use disorders and posttraumatic stress disorder (PTSD). For example, the National Comorbidity Survey
(1) found that men with an alcohol or other drug use disorder were 2.06 and 2.97 times more likely than those without an alcohol or another drug use disorder to have co-occurring PTSD, respectively. Among women, the odds of having co-occurring PTSD in the presence of an alcohol or other drug use disorder were 2.48 and 4.46, respectively
(1) . The likelihood of these two disorders co-occurring in the Australian population were found to be even higher
(2) . Analysis of the National Survey of Mental Health and Well-Being found that men with an alcohol use disorder were 6.6 times more likely to have co-occurring PTSD than men without an alcohol use disorder, and men with a drug use disorder were 7.2 times more likely than men without a drug use disorder to have co-occurring PTSD. These odds for women were 4.5 and 12.4, respectively
(2) .
Despite the frequent co-occurrence, much remains to be understood about this comorbidity. Specifically, although existing analyses have identified the association between alcohol and other drug use disorders and PTSD
(1,
2), there is little epidemiological information regarding the association between PTSD and particular substances. The analysis of the Epidemiological Catchment Area (ECA) data by Cottler et al.
(3) found that individuals who had ever used cocaine or opiates were at particular risk of trauma exposure (odds ratio=5.06) and PTSD (odds ratio=3.62) compared to those who had never used cocaine or opiates
(3) . It is likely that these associations would be even stronger among those who use substances at problematic levels; however, this has not yet been examined.
There is also a notable lack of epidemiological research focusing explicitly on the interrelationships between these two disorders
(4), the demographic correlates of this comorbidity, or its impact on physical and mental health and disability. Existing clinical evidence indicates that substance use disorder plus PTSD may be associated with poorer physical and psychological health and poorer functioning
(5 –
8) compared to those with either disorder alone. However, because these studies have been limited to clinical groups of those in treatment for either disorder, they may be subject to self-selection or referral bias
(9) . Epidemiological examination of the factors associated with substance use disorder plus PTSD would add considerably to understanding this comorbidity. Achieving a better understanding of this comorbidity is particularly important given its association with poorer treatment outcomes
(10) .
With data collected from the Australian general population, the present study aimed to
Results
Prior analysis of the survey has shown that in the preceding 12 months, 1.3% of the population met DSM-IV criteria for PTSD (weighted N=180,802), and 7.9% met criteria for a substance use disorder (weighted N=1,061,081)
(11) . Six percent had an alcohol use disorder (weighted N=813,637), 2.2% had a cannabis use disorder (weighted N=302,246), 0.5% had a sedative use disorder (weighted N=64,976), 0.4% had an amphetamine use disorder (weighted N=46,917), and 0.3% had an opioid use disorder (weighted N=38,922). It is important to note that 85% of the people with a substance use disorder had only one substance use disorder, and at best, the association between any substance use disorders was fair (kappas ranged from 0.03 to 0.31)
(16) .
Substance Use Disorder and Trauma
High rates of trauma exposure were reported across all substance use disorders (more data are available online). After we controlled for age and sex, logistic regression analysis revealed that the greatest likelihood of trauma exposure was associated with sedatives (92.8% versus 56.7%) (odds ratio=7.94, 95% CI=3.16–19.97), amphetamines (91.0% versus 56.8%) (odds ratio=7.47, 95% CI=2.36–25.84), and opioid use disorders (87.8% versus 56.8%) (odds ratio=5.58, 95% CI=1.96–15.95). Poisson regression showed that individuals with these disorders experienced a greater number of traumatic events than those who did not have these disorders. After we adjusted for age and sex in Poisson regression, those who had been exposed to trauma experienced an average of 2.38 more substance use disorders compared to those who were not exposed to trauma (0.12 versus 0.05) (risk ratio=2.38, 95% CI=2.05–2.78). The most common trauma types experienced by individuals with substance use disorders were having witnessed serious injury or death (40.5%), having been involved in a life-threatening accident (33.1%), and having been threatened with a weapon, having been held captive, or having been kidnapped (25.7%).
Prevalence of Substance Use Disorder Plus PTSD
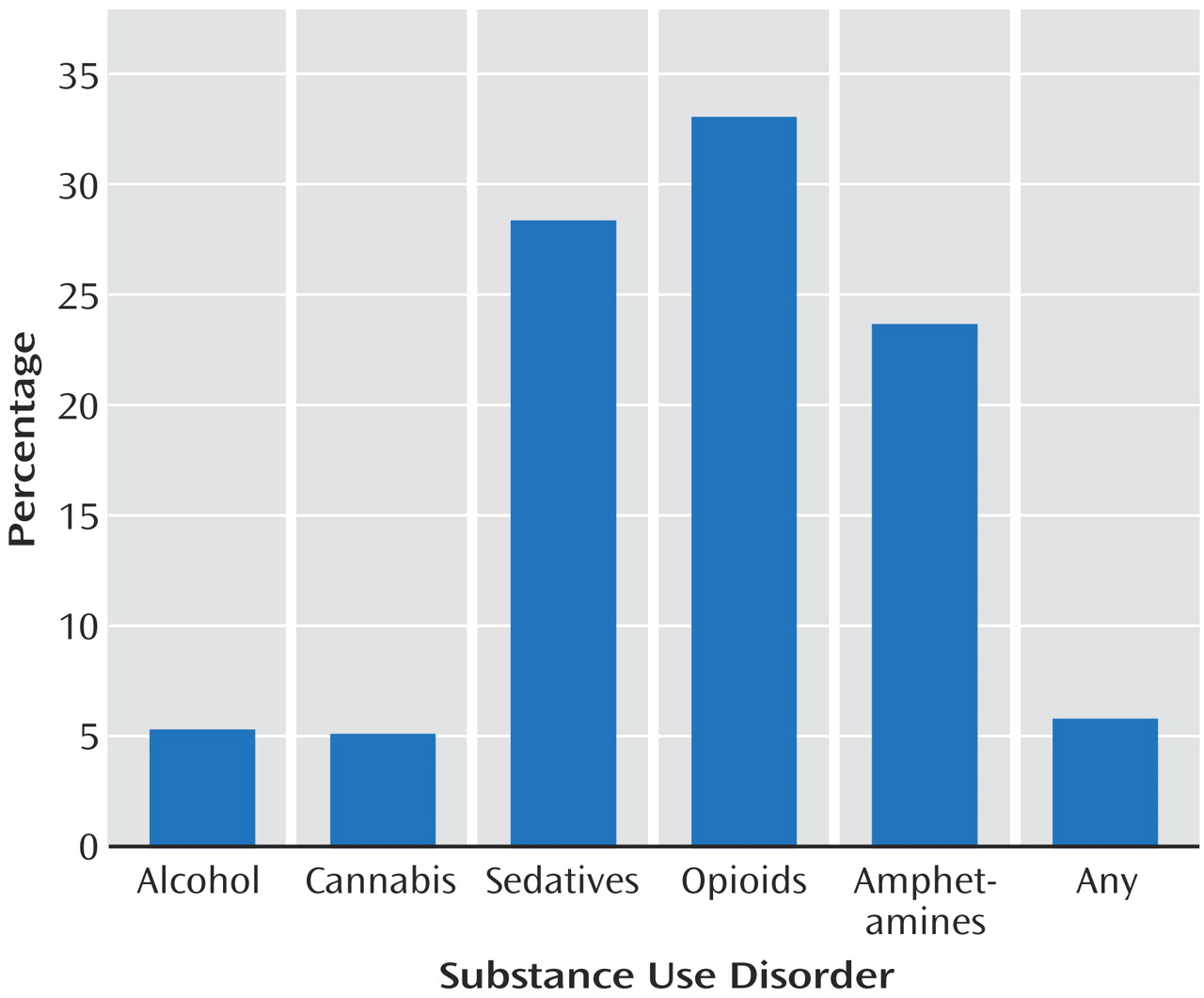
Overall, 34.4% of those with PTSD also had a substance use disorder, most commonly an alcohol use disorder (24.1%). After we adjusted for age and sex in logistic regression, individuals with PTSD were 5.19 times more likely to have an alcohol use disorder (95% CI=3.51–7.67) (
Figure 1 ). After we adjusted for age and sex in Poisson regression, those with PTSD had an average 5.47 more substance use disorders than those without PTSD (1.6 versus 1.2) (risk ratio=5.47, 95% CI=4.39–6.82).
Of those with a substance use disorder, 5.9% had comorbid PTSD, making them 6.53 (95% CI=4.55–9.36) times more likely to receive a diagnosis of PTSD compared to those without a substance use disorder after we adjusted for age and sex in logistic regression. The highest prevalence of PTSD was found among those with an opioid use disorder (33.2%), followed by those with a sedative use disorder (28.5%). After we controlled for age and sex in logistic regression, the likelihood of having PTSD was highest among those with sedative (odds ratio=24.06, 95% CI=12.93–44.76) and opioid use disorders (odds ratio=23.54, 95% CI=10.49–52.81).
For 57.5% of those with both a substance use disorder and PTSD, their most traumatic event occurred before the onset of substance use disorder symptoms. In 8.7% of the cases, the event occurred simultaneous to the onset of substance use disorder symptoms, and for 33.8%, the symptoms of substance use disorder preceded the most traumatic event. Those with both a substance use disorder and PTSD were equally as likely to have chronic PTSD (i.e., PTSD lasting for more than 1 year) compared to those with PTSD alone (78.4% versus 75.1%).
Correlates of Substance Use Disorder Plus PTSD
To examine the relationship between substance use disorder and PTSD, the sample was divided into four groups:
Substance use disorder plus PTSD: participants diagnosed with both a substance use disorder and PTSD.
Substance use disorder alone: participants diagnosed with a substance use disorder who did not have PTSD.
PTSD alone: participants diagnosed with PTSD who did not have a substance use disorder.
Neither: participants who were not diagnosed with either a substance use disorder or PTSD.
Only a small proportion of the group had substance use disorder plus PTSD (0.5%), representing an estimated 62,183 Australian adults (more data are available online). An estimated 7.4% had a substance use disorder alone, 0.9% had PTSD alone, and 91.2% had neither a substance use disorder nor PTSD. The remaining analyses were based on comparisons between these groups.
Demographics
We present prevalence estimates for demographic correlates in each of the four groups (more data are available online). Those with substance use disorder plus PTSD were more likely to be men than those with PTSD alone (odds ratio=2.52, 95% CI=1.29–4.94) and were more likely to be between 18 and 34 years than those with neither disorder (odds ratio=2.93, 95% CI=1.73–4.97). The group with substance use disorder plus PTSD was less likely than all other groups to be in a married/de facto relationship (substance use disorder alone: odds ratio=0.50, 95% CI=0.26–0.94; PTSD alone: odds ratio=0.33, 95% CI=0.16–0.68; neither: odds ratio=0.19, 95% CI=0.10–0.35). There were no differences in level of educational attainment among the four groups. Those in the group with substance use disorder plus PTSD were more likely than those in the group with substance use disorder alone (odds ratio=4.63, 95% CI=2.61–8.23) and the group with neither (odds ratio=4.44, 95% CI=2.55–7.73) to derive their main source of income from a government allowance and less likely than all other groups to derive their main source of income from a wage or salary (substance use disorder alone: odds ratio=0.23, 95% CI=0.12–0.45; PTSD alone: odds ratio=0.41, 95% CI=0.19–0.86; neither: odds ratio=0.33, 95% CI=0.17–0.63).
Physical Health
After we adjusted for demographic characteristics and neuroticism in linear regression, substance use disorder/PTSD status was not associated with level of general physical health as measured by the 12-Item Short-Form Health Survey Questionnaire (substance use disorder plus PTSD: 44.0; substance use disorder alone: 49.3; PTSD alone: 45.1; neither: 48.9; t=1.85, df=3, p>0.05).
Sixty-one percent of those with substance use disorder plus PTSD reported at least one chronic health condition compared with 35% of those with substance use disorder alone, 41% of those with PTSD alone, and 39% of those with neither disorder. After we controlled for demographic characteristics and neuroticism in logistic regression, those with substance use disorder plus PTSD were more likely to report having a physical health condition than all other groups (substance use disorder alone: odds ratio=2.13, 95% CI=1.15–3.94; PTSD alone: odds ratio=2.38, 95% CI=1.15–4.92; neither: odds ratio=2.53, 95% CI=1.39–4.62). With a Poisson regression to control for demographic characteristics and neuroticism, those with substance use disorder plus PTSD were found to have a greater number of physical health conditions than those with substance use disorder alone (risk ratio=0.68, 95% CI=0.53–0.88), PTSD alone (risk ratio=0.71, 95% CI=0.52–0.98), or neither disorder (risk ratio=0.65, 95% CI=0.51–0.83).
Mental Health
General mental health
PTSD status was significantly associated with level of general mental health as measured by the 12-Item Short-Form Health Survey Questionnaire (substance use disorder plus PTSD: 35.1; substance use disorder alone: 46.9; PTSD alone: 37.4; neither: 52.4; t=12.59, df=3, p<0.001). After we adjusted for demographic characteristics and neuroticism, linear regression revealed that those with substance use disorder plus PTSD had significantly poorer general mental health than those with substance use disorder alone (mean difference=–7.86, 95% CI=–9.40 to –6.31), PTSD alone (mean difference=–1.91, 95% CI=–2.51 to –1.30), or neither disorder (mean difference=–7.89, 95% CI=–9.98 to –5.81).
Comorbid affective, anxiety, and personality disorders
Almost two-thirds of those in the group with substance use disorder plus PTSD and the group with PTSD alone had a comorbid affective disorder, and approximately half in both groups had a comorbid anxiety disorder (excluding PTSD) (Table 4). Personality disorders were also highly prevalent among those with substance use disorder plus PTSD (62.3%).
After we controlled for demographic characteristics and neuroticism in logistic regression, those with substance use disorder plus PTSD were significantly more likely to have a comorbid affective, anxiety, or personality disorder than those with substance use disorder alone or neither disorder. Those with substance use disorder plus PTSD were equally likely to have each of those comorbidities as those with PTSD alone.
Suicidal ideation and attempted suicide
More than half of those with substance use disorder plus PTSD had ever thought about suicide, and 17.3% had a lifetime history of attempted suicide (more data are available online). After we controlled for demographic characteristics and neuroticism in logistic regression, those with substance use disorder plus PTSD were no more or less likely to have ever considered or attempted suicide than those with substance use disorder or PTSD alone. Although those with substance use disorder plus PTSD were no more likely to have considered suicide than those with neither disorder, they were more likely to have a lifetime history of attempted suicide.
Disability
After we controlled for demographic characteristics and neuroticism in logistic regression, those with substance use disorder plus PTSD were more likely to have had at least 1 day out of role in the last month than those with substance use disorder alone (53.7% versus 24.4%) (odds ratio=2.79, 95% CI=1.60–4.85) and neither disorder (53.7% versus 17.1%) (odds ratio=4.03, 95% CI=2.36–6.87). There was no difference in the likelihood of having had at least 1 day out of role in the last month between those with substance use disorder plus PTSD and those with PTSD alone (53.7% versus 40.3%) (odds ratio=1.39, 95% CI=0.72–2.69).
Discussion
Consistent with previous epidemiological and clinical investigations conducted in the United States
(1,
5), the present study found that substance use disorder and PTSD were highly comorbid conditions experienced by over 62,000 Australians. This represents a significant minority of the general population. Approximately one-third of those with PTSD also had a substance use disorder, and 5.9% of those with a substance use disorder also had PTSD. The presence of either disorder significantly increased the likelihood of having the other (odds ratio=6.53). These findings provide further evidence that there is a significant association between substance use disorder and PTSD and that their co-occurrence in clinical samples is not merely due to selection bias. Previous research has demonstrated that traumas leading to PTSD are experienced at similar rates in both Australia and the United States
(2) .
Trauma exposure and PTSD were highly prevalent across all substance use disorders. Notably, the highest rates of PTSD were among those with opioid, sedative, or amphetamine use disorders. It should be noted, however, that substances used are likely to be influenced by the drug markets of particular countries. Cocaine use disorders were not measured in the National Survey of Mental Health and Well-Being because of the low prevalence of use among the Australian population. However, Cottler et al.
(3) found a strong association between cocaine use and PTSD in the ECA study. Nonetheless, findings from the present study and studies from the United States have demonstrated a clear association between PTSD and hard-core drug use across cultures.
The elevated prevalence of PTSD among hard-core substance abusers may be due in part to the high-risk lifestyle associated with this kind of drug use. This lifestyle increases the risk of exposure to trauma, indirectly increasing the likelihood of subsequent PTSD
(17) . However, for two-thirds of those diagnosed with both a substance use disorder and PTSD, symptoms of substance use disorder followed or developed at the same time as their most traumatic event, suggesting that the majority of those with this comorbidity may be self-medicating their PTSD symptoms
(18) . The cross-sectional nature of this study does not allow for strong causal inferences to be made; however, it seems important that treatments for this comorbid substance use disorder plus PTSD focus on the interconnectedness of the two disorders.
As found in the clinical literature
(8), individuals with lifetime trauma exposure were also found to abuse or be dependent on multiple substances. It may be that individuals with substance use disorder plus PTSD require the use of multiple substances to alleviate different symptoms of PTSD or to overcome tolerance to one drug. The high rate of polydrug use among those with PTSD is of concern because of the harms associated with polydrug use, including overdose
(19), poor physical and mental health
(20), and HIV risk-taking behavior
(21) . Because substance use disorder categories in the present study were not mutually exclusive and no measure was taken of primary drug of concern, associations between different substances and particular trauma types, the chronicity of PTSD, and PTSD symptom clusters could not be examined. It is recommended that future research examine these associations by participants’ primary drug of concern.
Individuals with substance use disorder plus PTSD were typically young, unmarried, or not in a de facto relationship and derived their main source of income from a government allowance. Together, these findings indicate that individuals with substance use disorder plus PTSD have poorer social and occupational functioning, particularly when compared with those with substance use disorder alone. Similar findings have been noted in both Australian and American studies of individuals with comorbid substance use disorder plus PTSD
(8,
22) . These associations are of clinical concern because it has been suggested that the lack of support from an intimate partner and financial constraints may create practical and emotional barriers to accessing treatment and may be potential risk factors for relapse after treatment
(23) .
In keeping with studies of people seeking treatment for a substance use disorder in both the United States and Australia
(6,
8), those with substance use disorder plus PTSD were found to be in poorer general physical and mental health compared to those with substance use disorder alone, with 12-Item Short-Form Health Survey Questionnaire scores between and 1 standard deviations below the population mean, respectively
(13) . Affective, anxiety, and personality disorders were also more prevalent among those with this comorbidity; however, they were no more likely to have considered or attempted suicide. Nonetheless, it should be noted that approximately one in five people with either substance use disorder plus PTSD or substance use disorder alone had a lifetime history of attempted suicide. Given their poorer physical and mental health, it is not surprising that those with substance use disorder plus PTSD were more likely to have had a day out of role in the preceding month. These findings are of relevance to treatment providers because many of these psychological correlates have been shown to have a negative impact on substance use disorder treatment outcomes
(24) . These findings also reveal that individuals with comorbid substance use disorder plus PTSD demonstrate a significant challenge to treatment providers and are likely to require substantial clinical resources.
Although those with substance use disorder plus PTSD were more likely to have a chronic health condition and had a greater number of health conditions than those with PTSD alone, the two groups shared a remarkably similar clinical profile. This finding indicates that the additional morbidity seen among individuals with substance use disorder plus PTSD may be attributed largely to PTSD. Thus, treating substance use disorder alone in such circumstances is unlikely to remedy the other problems experienced by individuals with this comorbidity
(7) . This is not to say that by treating PTSD the substance use disorder will resolve but rather that both disorders should be treated concurrently.
Findings from the present study must be considered in light of a number of limitations. Despite the sophisticated sampling design used in the National Survey of Mental Health and Well-Being, it is unlikely that the sample is representative of all those with a substance use disorder or PTSD because of the hidden nature of this population and the difficulties inherent in accessing these individuals. For example, a small but significant proportion of those with substance use disorder and PTSD are homeless. Because participants were recruited from private dwellings, these individuals would not be represented in the present study. Furthermore, underreporting of drug use by patients with mental illness has been reported in studies that compared self-report measures with observer reports and laboratory tests
(25) . Two studies, however, have examined self-reported substance use among those with PTSD and found their responses to be highly valid
(26,
27) .
In spite of these limitations, the present study has provided important information regarding the clinical profile of individuals with substance use disorder plus PTSD. The similarity in findings from studies conducted in the United States and Australia also demonstrates that these associations occur in spite of differences in culture, drug use, and the provision of substance abuse treatment. It is important that individuals are assessed for substance use disorder plus PTSD upon entry into treatment for either disorder so that they may receive appropriate referral and treatment. It is also important that future research examine the impact of this comorbidity on treatment outcomes because current studies of this association are limited. Additionally, further research is necessary to determine which treatments are most effective in treating comorbid substance use disorder plus PTSD
(28) .