Major depressive disorder is usually an episodic disease, with recurrent episodes occurring in at least 50% of the patients seeking treatment for major depression at tertiary care centers
(1). Although patients usually suffer multiple episodes of major depression, most studies have examined only a single recurrence.
The National Institute of Mental Health (NIMH) Collaborative Program on the Psychobiology of Depression
(2) is a prospective, naturalistic, longitudinal investigation that has helped describe the episodic course of illness in major depressive disorder. Early research from the NIMH collaborative depression study found that after recovery from an index episode of unipolar major depression, the cumulative probability of recurrence was nearly 30% after 6 months of follow-up and almost 40% after 12 months of follow-up
(3). The time to recurrence was significantly shorter for those with a history of three or more episodes of major depression before intake than for subjects with fewer than three previous episodes.
Since that 1983 report, a large number of subjects from the NIMH collaborative depression study have suffered multiple recurrences. The present study focuses on the time to recurrence of major depressive disorder across multiple episodes that have been prospectively observed in their entirety. Based on studies of a single recurrence
(3–
5), it was predicted that as the duration of recovery increases, the risk of recurrence decreases. A second prediction was that each recurrence increases the probability of yet another recurrence.
RESULTS
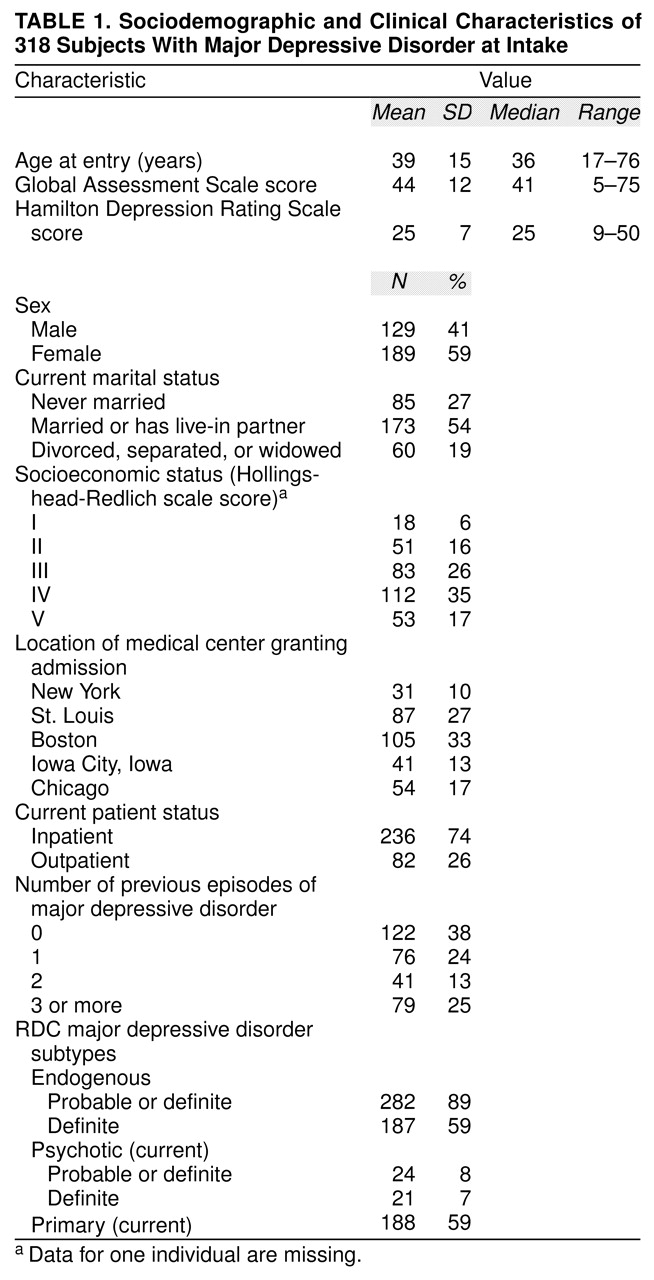
The study group comprised 318 subjects who had recovered from their intake episode of unipolar major depression during the first 10 years of follow-up are included. Data for 34 subjects (11%) who died during follow-up are included. Of the 318 subjects, 263 (83%) were followed for at least 5 years, and 208 (65%) were followed for the entire 10-year period. The mean length of follow-up was 419 weeks (SD=159), and the median length of follow-up was 520 weeks. A total of 481 recurrences were observed during the 10-year follow-up. The mean number of episodes of major depressive disorder per year of follow-up was 0.21 (SD=0.24).
Survival Analyses of Time to Recurrence
The survival analyses for the first five prospectively observed recurrent episodes of major depressive disorder are shown in
table 2. The analyses are presented as the proportion of subjects who had not yet had a recurrence (i.e., remained well) at various points in the follow-up period. The time periods start after the completion of an 8-week recovery period. (Subjects were at risk for recurrence only after they had recovered—i.e., completed the 8-week recovery period.) There were 318 subjects who recovered from their intake episodes. Of these, 202 suffered a recurrence. The remainder were treated as censored cases at the end of their follow-up. The cumulative probability of recurrence at 1 year was 25%; at 2 years, 42%; and at 5 years, 60%. (The proportions in
table 2 represent Kaplan-Meier product limit estimates, which incorporate censored cases.)
Of the 202 subjects who suffered a recurrence, 172 recovered and were at risk for a second recurrence. A total of 115 subjects eventually had a second recurrence. The cumulative probability of recurrence at 1 year was 41%; at 2 years, 59%; and at 5 years, 74%.
With each succeeding recurrence, the cumulative probability of recurrence generally increased at each time point (moving down each column in
table 2). However, the overlapping confidence intervals at each time point suggest that the differences were not statistically significant.
Median Time to Recurrence
For the entire study group, the median time to recurrence for the first prospectively observed recurrence was 150 weeks, and the 95% confidence interval (CI) was 116–204 weeks. For the second recurrence, the time was 83 weeks (95% CI=60–108); for the third recurrence, 77 weeks (95% CI=44–104); for the fourth recurrence, 68 weeks (95% CI=32–112); and for the fifth recurrence, 57 weeks (95% CI=28–88). The 95% CIs indicate that the median time to recurrence for the first prospective recurrence was significantly longer than the time to recurrence for subsequent recurrences. For subsequent episodes, the median times to recurrence did not differ significantly (because of overlapping CIs).
Interval-Specific Probability of Recurrence
Analyses were also conducted to calculate the semiannual interval-specific probability of recurrence—that is, the probability that a patient who was still well at the start of a 6-month interval would experience a recurrence during those 6 months. Across the five recurrences, the mean probability of recurrence during the first 6 months after recovery was 20% (SD=6) (weighted by number of subjects). This indicates that, on average, of the subjects at risk for recurrence, 20% had a recurrence in the first 6 months after the onset of recovery from the preceding depressive episode.
In subsequent 6-month intervals, the rate of recurrence decreased. Across all five recurrences, the weighted mean for the probability of recurrence in the second 6 months (months 7–12) after the onset of recovery from the preceding mood episode was 19% (SD=7); in the third 6 months (months 13–18), the weighted mean was 15% (SD=6); in the fourth 6 months (months 19–24), the weighted mean was 13% (SD=3); in the fifth 6 months (months 25–30), the weighted mean was 11% (SD=3); and in the sixth 6 months (months 31–36) after the onset of recovery from the preceding mood episode, the weighted mean for the probability of recurrence was 9% (SD=6). The mean average interval-specific probabilities of recurrence were not compared statistically because the groups of subjects overlapped.
Probability of Recurrence
Mixed-effects, grouped-time survival analysis was used to examine recurrence during all prospectively observed recovery periods. The number of lifetime episodes of major depressive disorder was significantly associated with recurrence during the 10-year follow-up period (odds ratio=1.16, 95% CI=1.03–1.31; z=2.33, p=0.02). Thus, for each successive episode of major depression, the risk of recurrence increased by 16%. The ICC from the mixed model was 0.20, which indicates that there was very little consistency in the time to recurrence within subjects.
Treatment
The highest level of pharmacotherapy received during any of the 4 weeks immediately preceding the onset of the five prospectively observed recurrences was examined. The low level of maintenance treatment was striking. During the 4 weeks immediately before the onset of the first three prospectively observed recurrences, 47%–50% of all subjects received no pharmacotherapy. During the 4 weeks immediately before the onset of the fourth and fifth prospectively observed recurrences, one-third of the subjects received no pharmacotherapy. During any of the 4-week periods immediately preceding the onset of the five prospectively observed recurrences, only 33% to 45% of the subjects received at least 100 mg/day of imipramine or its equivalent, and only 18% to 30% received at least 200 mg/day of imipramine or its equivalent.
By using the composite antidepressant score previously described, the mean level of treatment for the 4 weeks immediately preceding the recurrence was calculated for each of the five recurrences. For the first recurrence, the mean was 1.1 (SD=1.3); for the second, the mean was 1.1 (SD=1.3); for the third, the mean was 1.2 (SD=1.3); for the fourth, the mean was 1.4 (SD=1.3); and for the fifth recurrence, the mean was 1.6 (SD=1.5). (As noted earlier, a composite antidepressant score of 1 indicated a dose of 1–99 mg/day of imipramine or its equivalent, and a composite antidepressant score of 2 indicated a dose of 100–199 mg/day of imipramine or its equivalent.)
DISCUSSION
The length of prospective observation distinguishes the present study from previous investigations. By means of the current study and its 10 years of follow-up, we were in a better position to retain and assess the individuals whose course of illness was marked by a long interval from one recurrent episode to the next. This reduced the likelihood that the length of the observation period would condition or bias the results.
The probability of recurrence decreased for each successive 6-month interval after recovery, as shown by the mean average interval-specific probability of recurrence. In addition, the results within each row of
table 2 show that for each recurrence, the rate of risk of recurrence fell as time elapsed. Both of these findings indicate that as the duration of recovery increases, the risk of recurrence decreases or decays (first prediction). Previous observational
(3,
4) and treatment
(16–
19) studies have also found that the probability of a single recurrence of major depression declines over time. Similarly, in a study of subjects from the collaborative depression study with bipolar I disorder, the risk of recurrence decreased as the duration of recovery increased
(20).
The findings from the mixed-effects model suggest that the probability of recurrence of major depression is significantly influenced by the number of lifetime episodes experienced before any recovery period or well interval. This confirms the second prediction that the probability of recurrence increases with each succeeding episode. With each successive recurrence, the risk of a subsequent recurrence increases by 16%. Thus, a patient with five lifetime episodes of major depressive disorder is more than twice as likely to suffer a recurrence than is a patient with one lifetime episode.
For the subjects with two or more prospectively observed episodes, the consistency in time to recurrence was low, as quantified by the ICC. This indicates that the time to recurrence is highly variable for any particular individual and accords with Kraepelin’s observation
(21) that these patients experience a “sequence of attacks…between which pauses are interpolated of extraordinarily fluctuating duration” (p. 188).
One limitation of this study is that the cohort at risk for each succeeding prospective recurrence became progressively smaller. This was in part due to the subjects who did not recover and remained ill during follow-up and were therefore not at risk for recurrence. Also, the subjects who recovered and did not have a recurrence were not at risk for additional episodes. Thus, patients with relatively long intervals of illness or wellness were disproportionately excluded from successive analyses. As a result, the analyses underestimate the rates of recurrence over the lifetime of the patients. Even longer follow-up intervals would be required to more fully incorporate these subjects into the analyses and more accurately describe the course of illness for the entire study group.
Another limitation is that the analyses were restricted to episodes of major depression. Episodes of minor depression or intermittent depression were not included, with the net effect of underreporting the extent of psychopathology suffered by the study group.
This was an observational study, and treatment was not randomly assigned. As a result, treatment varied, and this may have influenced the findings. It is possible that some subjects recovered and discontinued treatment in the belief that they no longer required it and, by so doing, may have placed themselves at an increased risk for recurrence. It is also possible that the recurrence of major depressive disorder in patients receiving treatment may have left some of these patients feeling discouraged about treatment in general, with the result that they never pursued treatment again and were thus at increased risk for subsequent recurrence. Many of the subjects in the present study received little or no maintenance pharmacotherapy. This is unfortunate, given the findings from treatment studies
(17–
19) that indicate that maintenance therapy is efficacious in preventing recurrences.
Our findings can be summarized as follows. 1) After recovery from the index episode of unipolar major depression, the subjects suffered an average of two recurrences during 10 years of follow-up. 2) As the duration of recovery increased, the probability of recurrence decreased. 3) The probability of recurrence was significantly influenced by the lifetime number of episodes, such that the risk of recurrence increased by 16% with each successive recurrence. 4) The within-subject time to recurrence varied considerably from one recurrence to the next. 5) Many subjects received little or no maintenance treatment before recurrences.