Follow-up studies
(1,
2) examining outcome decades after an index episode have been the primary source of data about full recovery (i.e., sustained improvement in both symptoms and social/vocational functioning) among patients with schizophrenia. These studies provided the important information that about half of patients eventually recover or have only mild impairment. However, these investigations were limited by their reliance on retrospective information. In addition, because the initial evaluations were done decades ago, data were not available for many biological and clinical measures of current interest. There have been no follow-up studies of recovery during the crucial early phase of the illness.
Our study addressed the following questions. How frequently do patients recover during the early course of schizophrenia? What are the predictors of early recovery? Do predictors of full recovery differ from predictors of symptom remission and predictors of adequate social/vocational functioning? In order to study recovery prospectively, subjects must be assessed frequently in multiple domains over a long period of time. We were able to address our questions about recovery using data from a prospective study conducted from January 1986 until February 1999 that assessed patients for a period of up to 9 years from their first episode of schizophrenia or schizoaffective disorder.
Method
The parent study has been described in detail elsewhere
(3–
5). Study conduct conformed to the guidelines of the Long Island Jewish Medical Center Institutional Review Board. After a complete explanation of the study, subjects and available family members provided written informed consent. Subjects (N=118) who met Research Diagnostic Criteria
(6) for schizophrenia or schizoaffective disorder and who had no more than 12 weeks of lifelong antipsychotic treatment were assessed at baseline, treated according to a standardized medication algorithm, and evaluated prospectively. Subjects progressed from one medication in the algorithm to the next until they responded. The sequence of medications was as follows: fluphenazine, haloperidol, haloperidol plus lithium, either molindone or loxapine, and clozapine. Adjuvant medications (sertraline or lithium) for mood stabilization were used as clinically indicated. Benztropine, lorazepam, and propranolol were prescribed as needed for side effects. The treatment settings were an inpatient unit, day and partial hospital programs, and an outpatient department. In each setting, treatment was administered by the study treatment team (psychiatrist, research social worker, and nurse). In addition to clinical management, there was a psychoeducation program for subjects and family members. Group and individual psychotherapy were provided as needed. Subjects also had access to an extensive range of ancillary services (e.g., rehabilitation services) provided by Zucker Hillside Hospital, a large psychiatric center. Initially, there was no limitation on study duration; later the length of treatment in the study was set at 5 years.
Assessments and Measures
The parent study included many measures; those used in the current analyses were as follows.
Diagnosis
At baseline, patients were interviewed with the Schedule for Affective Disorders and Schizophrenia (SADS)
(7). Final study RDC diagnosis for each subject was assigned when the initial episode remitted (or after 1 year of study participation for patients who did not remit). Information sources used were the baseline SADS interview, interviews with family members, longitudinal psychopathology ratings, and clinical data from the treatment team.
Psychopathology
The Schedule for Affective Disorders and Schizophrenia—Change Version (SADS-C) with psychosis and disorganization items
(8) was completed at baseline, every 2 weeks during treatment of acute episodes, and every 4 weeks at other times. The Scale for the Assessment of Negative Symptoms (SANS)
(9) was employed at baseline and every 4 weeks.
Premorbid social adjustment
The Premorbid Adjustment Scale
(10) was completed at baseline from information provided by both patients and family members. “Premorbid” was defined as the period ending 6 months before the first psychiatric contact or hospitalization or 6 months before any evidence of florid psychotic symptoms.
Neuropsychological assessments
After stabilization of the initial psychotic episode, subjects were tested with a comprehensive cognitive battery that included 41 tests
(11). Tests were grouped to characterize six domains: language, memory, attention, executive function, motor function, and visuospatial function. The mean of these six scales was employed as the global scale. A premorbid cognitive functioning scale was also constructed that was based upon the hypothesis that certain tests of general knowledge, vocabulary, and reading skill are less liable to deteriorate
(12,
13). The contribution of test variables to scales was based on an a priori assessment of content validity, similar to methods previously described
(12,
14,
15). Scores for each scale were computed by averaging z scores on contributing variables. These z scores were based on the performance of a healthy comparison group (N=36). Higher values on the cognitive scales indicate better performance.
Social adjustment
The Social Adjustment Scale II
(16) was used every 6 months to assess this variable.
Magnetic resonance imaging (MRI)
Brain scans were obtained during the index episode using a 1.0-T whole-body MRI system (Magnetom, Siemens, Erlangen, Germany). Images acquired by a three-dimensional gradient echo sequence (coronal acquisition, 3.1-mm thick contiguous slices, with 256×256 matrix in a 24-cm field of view; number of excitations=1; TR=40 msec, TE=15 msec, flip angle=50°) were used for morphometric analysis. A semiautomated mensuration system was used for assessing whole brain, cortical, ventricular, caudate, superior temporal gyrus, and hippocampal volumes (methods described in references
15,
17–19). To examine the effects of regional cerebral volume asymmetry, volumes for prefrontal, premotor, sensorimotor, occipitoparietal, and temporal lobes in each hemisphere were calculated (as described elsewhere
[20]). Asymmetry indexes were computed for each region using the formula: ([right volume minus left volume] divided by [right volume plus left volume]) multiplied by 100. Torque, a composite index of cortical asymmetry, was calculated as prefrontal index plus premotor index plus temporal index minus occipitoparietal index minus sensorimotor index. In the calculation formula, the sensorimotor and occipitoparietal indexes were subtracted so that higher positive values of torque indicate a more healthy pattern of asymmetry.
Recovery Criteria
Our recovery measures were derived from the University of California at Los Angeles recovery criteria
(21). Full recovery required that subject ratings covering the same period fulfill criteria for both symptom remission and adequate social/vocational functioning. We operationalized the definitions for these components as follows. Symptom remission criteria required both 1) a rating of no worse than “mild” (score=3) for all of the following SADS-C psychosis items: severity of delusions, severity of hallucinations, impaired understandability, derailment, illogical thinking, and bizarre behavior and 2) a rating of no worse than “moderate” (score=3) for the SANS global ratings of affective flattening, alogia, avolition-apathy, and anhedonia-asociality. Adequate social/vocational functioning criteria had three components derived from ratings on the Social Adjustment Scale interview; all components had to be fulfilled to meet criteria. The first component was appropriate role function, defined as paid employment, attending school at least half-time or, if a homemaker, performing that role adequately or better. The second component was the ability to perform day-to-day living tasks without supervision. This entailed personal appearance and grooming that was “reasonable, neat, clean and appropriate” or better and at least adequate functioning as a homemaker or, if not the primary homemaker for the family, a rating of “usually carries out most chores with little difficulty” or better on the performance adequacy (chores) item. The third component was social interactions with a peer outside of the family, defined as social interactions once a week or more with friends or romantic contacts.
Data Analysis
Each subject rating was classified as meeting criteria for full recovery and, separately, for the recovery components of symptom remission and adequate social/vocational functioning.
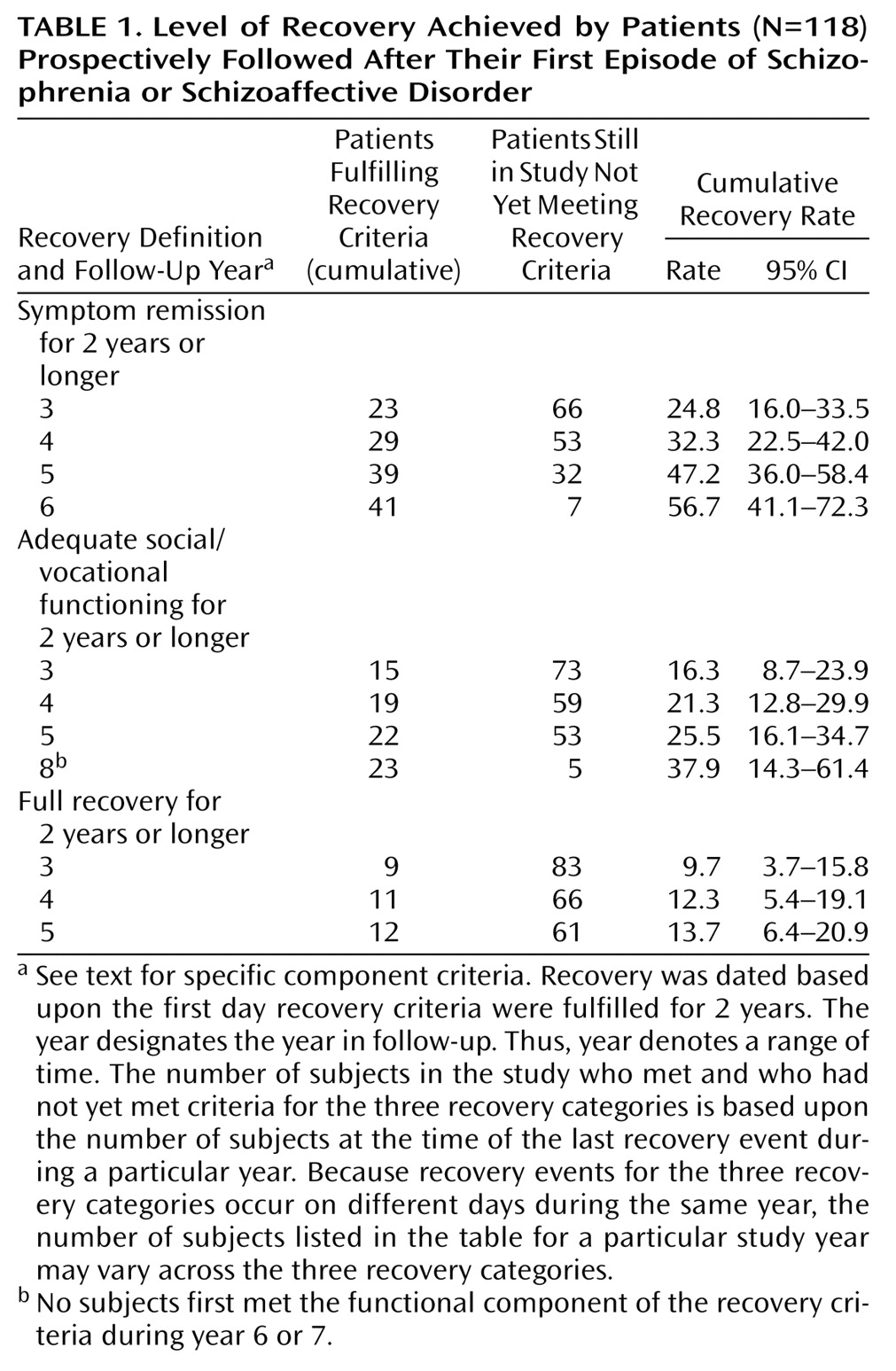
Recovery rates
Subjects were classified as meeting criteria for symptom remission, adequate social/vocational functioning, or full recovery if their ratings met the appropriate criteria for 2 consecutive years. Cumulative recovery rates were determined by survival analyses that adjusted for differences in duration of follow-up among subjects; 95% confidence intervals (CI) are provided to indicate the precision of these estimated rates.
Predictors of recovery
The recovery rate definitions provide an easy-to-understand summary of clinically meaningful outcomes. However, to explore predictors of recovery, continuous measures of recovery (rather than the dichotomous variables used for the recovery rate analysis) were used in order to minimize information loss. We constructed these continuous measures for the predictor analyses using the entire array of each individual’s ratings and did not require that criteria be maintained for 2 years. For each subject we calculated the proportion of all of their ratings that met the cross-sectional criteria for full recovery. We also calculated the same proportions separately for the symptom remission component and for the adequate social/vocational functioning component of the recovery criteria.
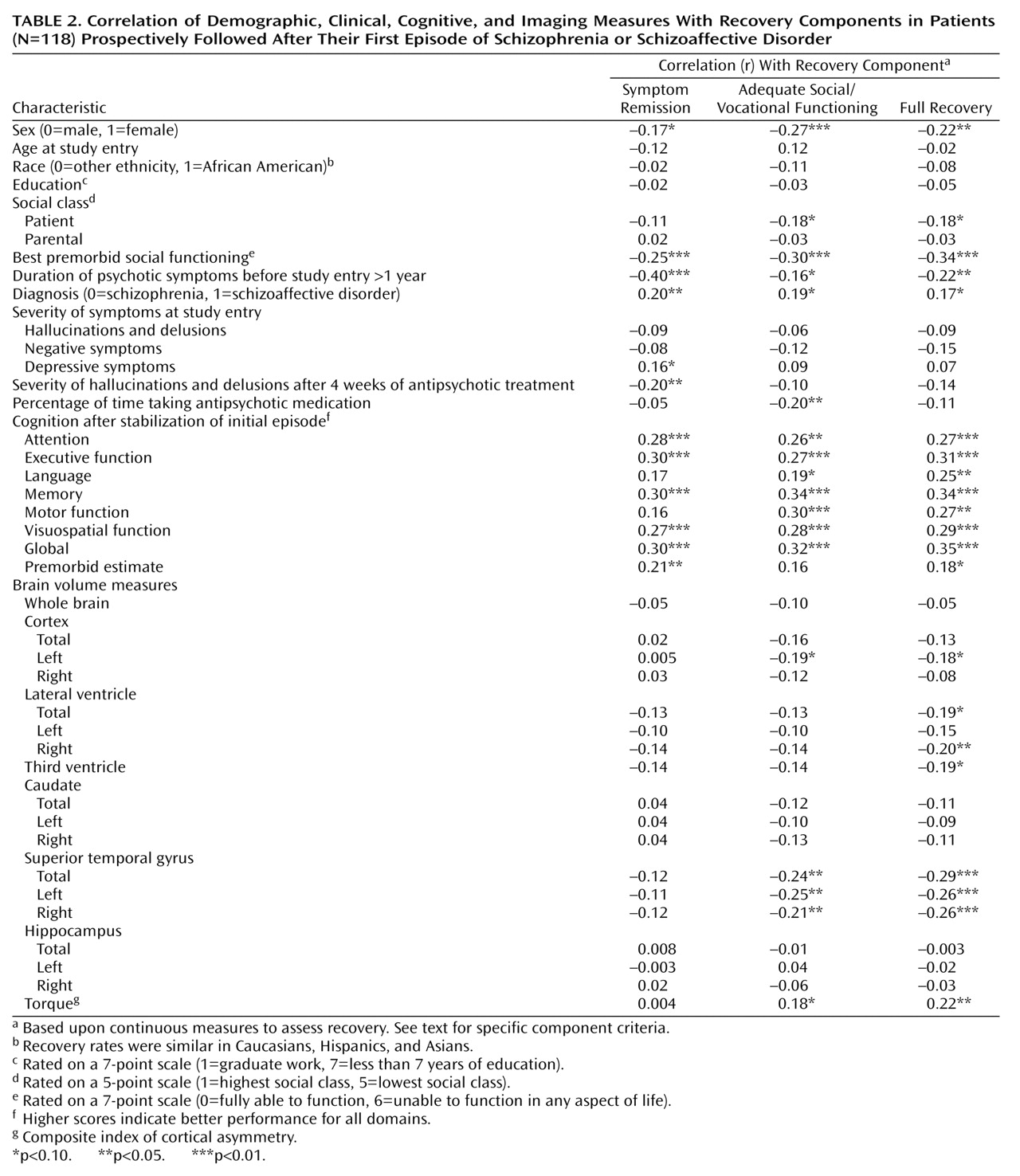
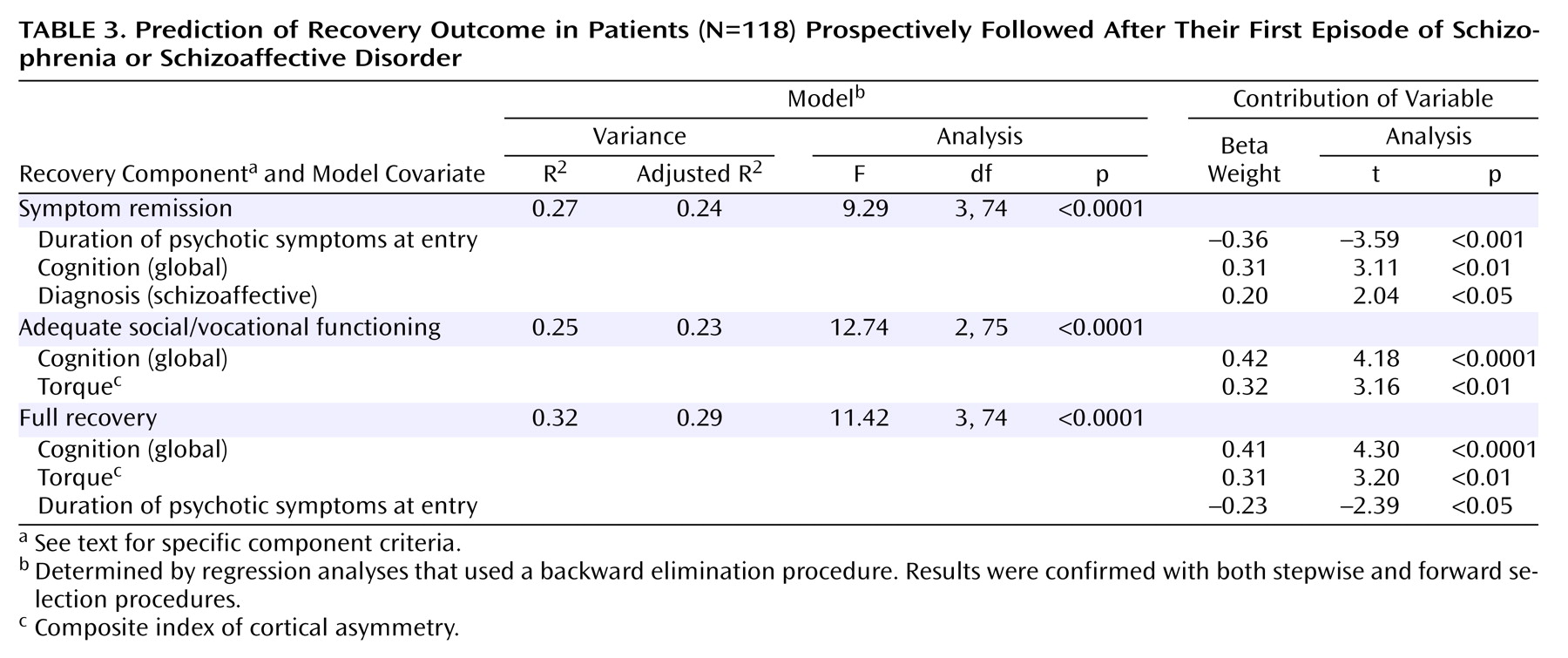
Regression analysis (backward elimination) was used to study the relative contributions of various predictors to the percent of the total number of ratings for each subject that met criteria for symptom remission, adequate social/vocational functioning, and full recovery. The set of potential explanatory variables consisted of demographic, clinical, cognitive, and MRI measures. Selection of variables for the regression models was based on correlational analyses. Variables were included in the models if they were significantly correlated at the p<0.05 level with symptom remission, adequate social/vocational functioning, or full recovery.
Discussion
Our subjects did well in terms of control of positive and negative symptoms, the usual measure of response in treatment studies. Approximately half had symptom remission for 2 years or longer. However, only a quarter of the subjects achieved sustained social/vocational recovery, and only 13.7% met criteria for full recovery. Direct comparison of our rates with those from the long-term follow-up studies is precluded by the very substantial differences in study design and outcome criteria. However, our data are consistent with the findings from the long-term studies in that some patients with schizophrenia can achieve both symptom remission and appropriate social/vocational functioning.
In evaluating our recovery rates, it is important to consider that the level of vocational and social functioning required by our criteria would not be met by some members of the general public who do not have a psychiatric disorder. Further, although early course may predict long-term course
(2), long-term follow-up studies
(1,
2) have consistently found a subgroup of subjects who recover after many years of severe illness. Our recovery rates may therefore underestimate the percentage of our subjects who eventually recover. Nonetheless, the very low rate of full recovery during our study observational period, despite what we believe was excellent treatment in a research team setting, highlights the importance of continuing efforts to develop treatments designed to improve the initial course of patients with schizophrenia.
We found specific predictors of recovery. Better cognitive performance was associated with full recovery and both the adequate social/vocational functioning and symptom remission components of recovery. The other two variables associated with full recovery, torque and duration of psychotic symptoms at study entry, were associated with only one of the recovery components. More cerebral asymmetry was associated with adequate social/vocational functioning, and duration of psychotic symptoms at study entry was associated with symptom remission. Elucidating the mechanisms underlying these associations may provide a basis for later development of interventions to promote recovery.
Our findings about the association between cognition and recovery are consistent with data from other studies relating cognitive performance and social/vocational outcome (reviewed in references
24,
25). However, relationships between cognitive performance and symptom outcomes have been much less recognized. In previous analyses of data from our parent study, relationships between cognitive performance and symptom outcomes were not consistent. Measures of attention were related to acute treatment response
(4), but cognitive performance was not related to relapse following initial symptom remission
(5). What may have contributed to our ability to detect the relationships between cognitive variables and symptom remission in the current analyses? One possibility is that our symptom remission criteria differed from most symptom outcome measures in 1) requiring a fixed level of improvement in both positive and negative symptoms and 2) assessing outcome over an extended period.
Regarding our other predictors, our finding of a relationship between duration of untreated psychosis and symptom remission is consistent with findings from many, but not all, studies of duration of untreated psychosis and treatment response (reviewed in reference
26). Our findings also indicate an association with full recovery. The association between symptom remission and the diagnosis of schizoaffective disorder is consistent with earlier studies
(2,
27,
28) that found that patients with schizoaffective disorder have less severe residual symptoms than patients with schizophrenia. Abnormalities in brain asymmetries have been found in many studies of schizophrenia (reviewed in reference
29) and have been postulated to be a core feature of the disorder by some investigators
(30). Neurodevelopmental abnormalities have been implicated as the cause of the decrease in cerebral volume asymmetry found in schizophrenia. In a previous analysis
(20) of a subset of the current sample, measures of torque were not associated with acute treatment response, but lower torque values were associated with more negative symptoms at baseline in men. Our results suggest an association with full recovery and longer-term social/vocational functioning.
Two variables not associated with our recovery measures deserve mention. Medication discontinuation was strongly associated with relapse in earlier analyses with our sample
(5). Although many subjects stopped medication at some point in our study, long-term medication adherence was very high, since subjects usually resumed medication following staff interventions or the return of symptoms. This limited our ability to detect medication effects on outcome and probably accounts for the lack of association between medication use and symptom remission in the current analyses. Ho and colleagues
(31) found that baseline negative symptoms predicted social/vocational outcomes at 2-year follow-up in a sample of 50 subjects with first-episode schizophrenia. In our analyses, more severe baseline negative symptoms were associated with poorer outcomes, but the correlations were not significant. The divergent findings from the two studies may result from differences in the outcome measures and the period covered by the assessments. The assessment period may be critical in studies of negative symptoms in first-episode schizophrenia, since the pattern of negative symptoms may still be evolving at this stage of the illness. This was highlighted by an earlier analysis
(32) of the first 70 subjects in our sample. Severity of baseline negative symptoms did not predict which subjects later developed persistent negative symptoms.
In summary, patients with first-episode schizophrenia or schizoaffective disorder can recover. However, the low rate of recovery during the early years of the illness highlights the need for continued efforts to develop better treatments to promote recovery by patients with schizophrenia.