Participants
Subjects consecutively admitted (including those admitted on a weekend) to a level 1 trauma service in Victoria, Australia, were eligible for the study. Individuals were included in the current study if they 1) experienced a physical injury that required an admission of at least 24 hours to the Trauma Service; 2) experienced either no brain injury or mild traumatic brain injury (as defined by the American Congress of Rehabilitation Medicine
[20]); 3) were between 18 and 70 years of age; and 4) had a reasonable comprehension of English. Participants were excluded if the injury was a result of deliberate self-harm, if they were currently abusing intravenous substances, or if they had a current psychotic disorder.
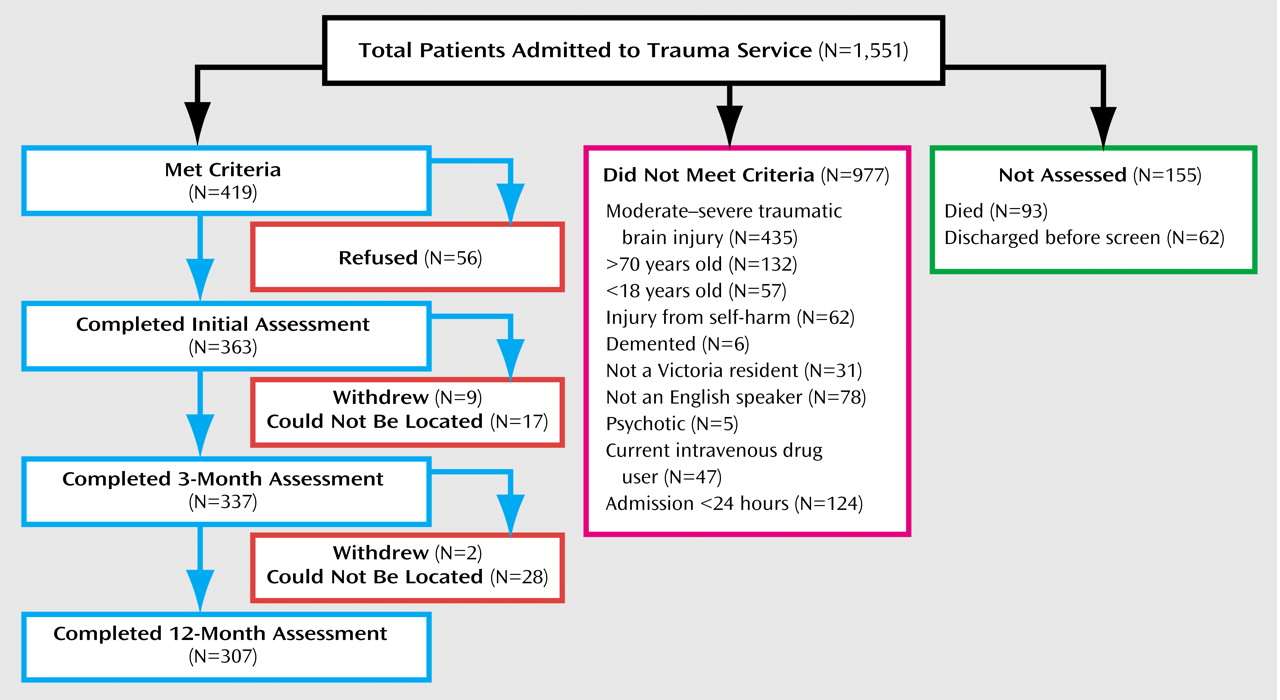
Figure 1 presents a flow chart of those included and excluded from the study.
Participants were recruited over an 18-month period. During this time, 419 individuals met inclusion criteria and were approached to participate in the study. After a complete description of the study, written consent was obtained from 363 participants (87%). Interview and self-report data were collected just before discharge. Follow-up telephone assessments were conducted 3 and 12 months after the trauma. A total of 337 participants (93% of those who commenced the study) completed the 3-month assessment and 307 participants (85% of those who commenced the study) completed the 12-month assessment.
Individuals who refused to participate in the current study did not differ from those who participated in terms of gender (χ2=3.80, df=1, n.s.), age (t=1.00, df=410, n.s.), days in the hospital (t=1.79, df=409, n.s.), injury severity score (t=0.05, df=442, n.s.), the presence of a head injury (χ2=0.00, df=1, n.s.), or discharge destination (home or rehabilitation service) (χ2=1.20, df=1, n.s.).
Subjects who did not complete the 3-month diagnostic interviews did not differ from those who did in terms of gender (χ2=0.54, df=1, n.s.), mild traumatic brain injury (χ2=0.02, df=1, n.s.), discharge destination (χ2=0.01, df=1, n.s.), number of days in the hospital (t=1.34, df=361, n.s.), or injury severity (t=0.32, df=358, n.s.). Noncompleters did differ from completers in terms of age (t=2.14, df=361, p<0.05), with noncompleters more likely to be younger. On psychological variables, noncompleters did not differ significantly in terms of depression (t=0.61, df=24.58, n.s.) or anxiety levels (t=1.79, df=354, n.s.) just before discharge.
Individuals who failed to complete the 12-month assessment did not differ from 12-month completers in terms of gender (χ2=0.14, df=1, n.s.), mild traumatic brain injury (χ2=0.85, df=1, n.s.), discharge destination (χ2=0.48, df=1, n.s.), or injury severity (t=1.89, df=358, n.s.). However, they did differ in terms of age (t=3.92, df=87.08, p<0.001) and number of days in the hospital (t=1.98, df=360, p<0.05), with noncompleters being more likely to be younger and having spent fewer days in the hospital. Noncompleters also reported higher levels of both anxiety (t=3.14, df=354, p<0.05) and depression (t=3.29, df=354, p<0.001) just before discharge, suggesting that the reported 12-month prevalence rates may be a slight underestimate.
The majority of participants were male (N=273 [75%]), and the average age was 36 years (SD=13.43). The average injury severity score
(21) was 12.80 (SD=9.73); 33% (N=121) of participants experienced a severe injury (injury severity score ≥15), 31% (N=113) had a moderate injury (injury severity score=10–14), and 36% (N=129) experienced a mild injury (injury severity score=0–9). Participants spent an average of 10.13 days (SD=9.64) in the Trauma Centre, with 31% (N=113) requiring an intensive care unit admission. Motor vehicle accidents were the principle mechanism of injury (74% [N=270]), while 9% (N=33) of injuries occurred at work, and 13% (N=47) were due to other accidents. Thirteen people (4%) were assaulted. A total of 202 participants (56%) met criteria for a mild traumatic brain injury
(20): loss of consciousness of 30 minutes or less, a Glasgow Coma Scale
(22) score of 13–15 after 30 minutes, or posttraumatic amnesia not greater than 24 hours. Approximately half the participants (53% [N=192]) were discharged home while the remainder were discharged to a rehabilitation facility.
The study sample resembled the characteristics of all trauma service admissions for the same time period with regard to gender (p=0.47, Fisher’s exact test) and mechanism of injury (p=0.43, Fisher’s exact test). The current study’s patient group, relative to the total population, was younger (mean=36 years [SD=13.43] versus 41 years [SD=21.06]; t=4.40, df=1912, p<0.001) and had a lower injury severity score (mean=12.80 [SD=9.73] versus 17.11 [SD=13.18]; t=5.87, df=1912, p<0.001). This is not surprising given that we excluded those over 70 years of age at admission, as well as all admissions with moderate to severe brain injury and, of course, those who were deceased.
Measures
The Clinician-Administered PTSD Scale for DSM-IV
(23) was used to assess PTSD after 3 and 12 months. This structured clinical interview is one of the most widely used tools for diagnosing PTSD and measuring PTSD severity and has demonstrated excellent reliability and validity
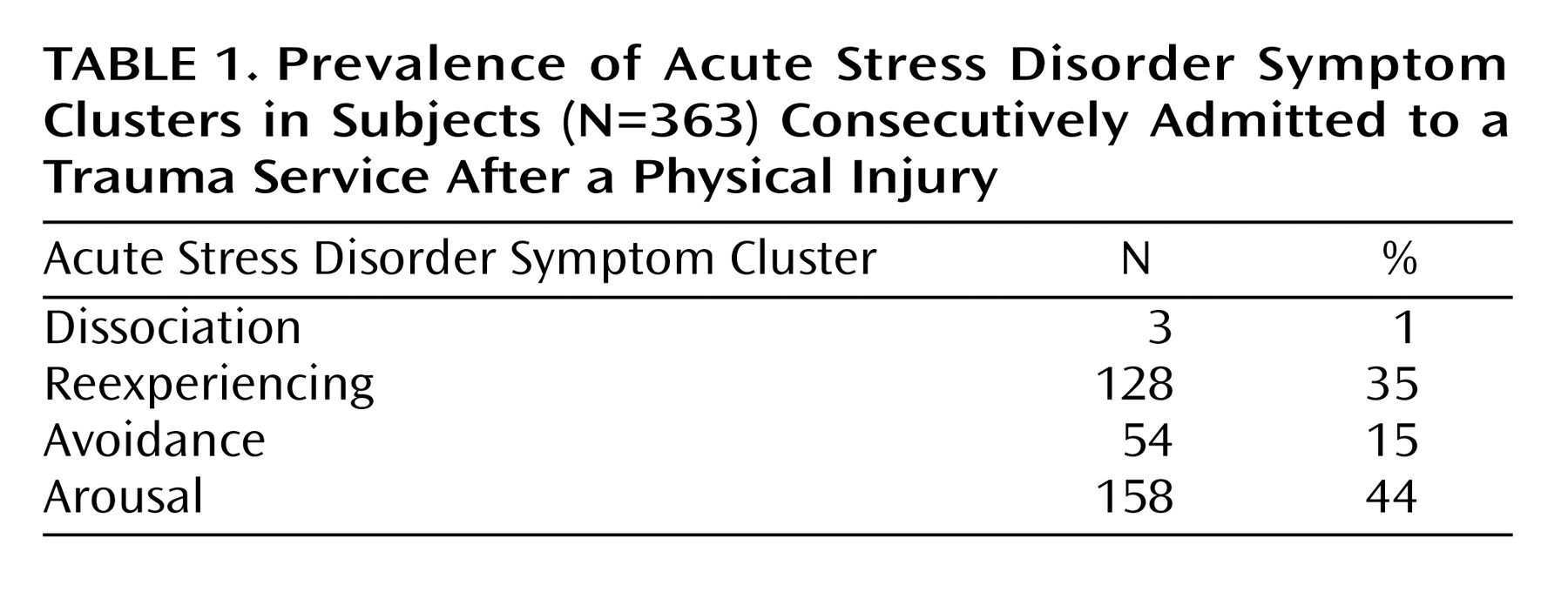
(24). The Clinician-Administered PTSD Scale, with its additional dissociation questions, was used also to assess acute stress disorder. Following common practice, both acute stress disorder and PTSD were scored using the “1-2 rule” (i.e., diagnostic criteria were met for each symptom if frequency ≥1 and intensity ≥2)
(25). Since the diagnosis of PTSD is, by definition, tied to a specific event, it was assessed in this study with specific reference to the injury-producing event.
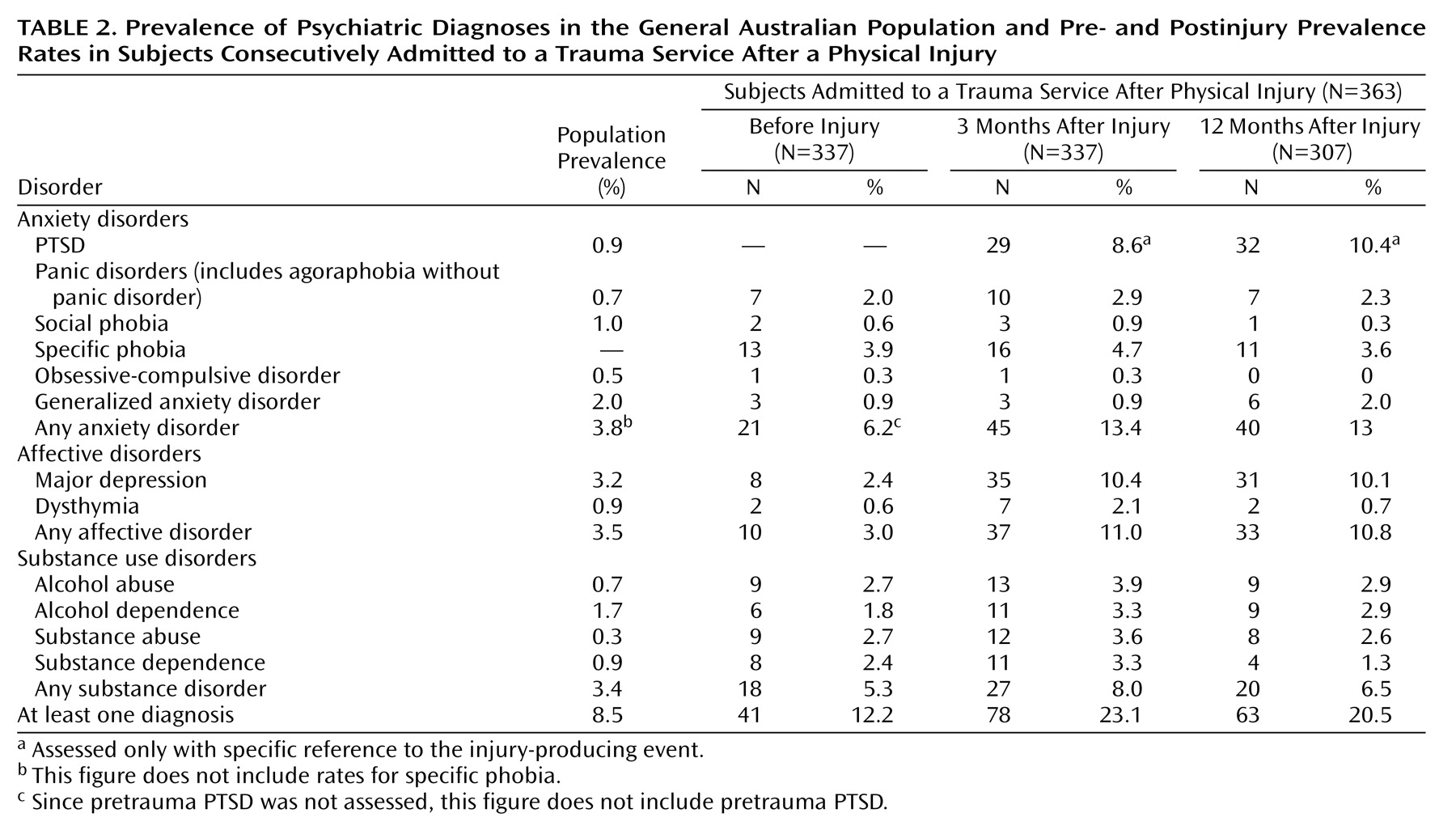
After 3 and 12 months, anxiety disorders, affective disorders, and substance use disorders were assessed by using the relevant modules of the Structured Clinical Interview for DSM-IV (SCID)
(26). The SCID is one of the most widely used and thoroughly researched psychiatric clinical interviews
(27). At the 3-month assessment, participants were asked about the duration of any conditions that met diagnostic criteria; those that had been present for more than 3 months were deemed to have been present before the traumatic event.
Self-report measures of anxiety and depression were also obtained with the Beck Anxiety Inventory
(28) and the Beck Depression Inventory
(29).
Two trained mental health clinicians conducted all structured clinical interviews. One-third of all clinical interviews were audiotaped, and one-third of those (approximately 10% of all assessments) were randomly selected and rated for interrater reliability. A high level of interrater agreement on diagnosis was obtained (kappa=0.95).
Procedure
Since blood loss and pain can produce symptoms that could be misinterpreted as psychogenic in nature, initial assessment was conducted just before discharge from the acute hospital. At this time, patients were hemodynamically stable and were relatively pain free. Since narcotic analgesia has side effects that can mimic dissociative symptoms (e.g., CNS disturbances), assessments were conducted at least 24 hours after intravenous narcotic cessation (mean=2.53 days, SD=2.37). Fifteen participants (4%) were receiving oral narcotic analgesia at the time of the assessment. There were no significant differences in current dissociative symptom levels between those receiving and not receiving oral narcotic analgesia (t=1.07, df=361, n.s.). The mean time of assessment was 7.74 days (SD=6.52) after admission and 2.45 days (SD=4.92) before discharge.
A diagnosis of acute stress disorder per DSM-IV requires three of five peritraumatic dissociative symptoms (“while experiencing or after experiencing” the trauma) to be present. However, the measurement of peritraumatic dissociation is difficult with an injured population. Many injured individuals experience mild traumatic brain injury, are administered narcotic analgesia at the scene of the trauma, or are intoxicated at the time of the incident, all of which may produce dissociative-like symptoms
(30). In the current study, most participants were administered narcotic analgesia at the scene of the trauma and over 50% experienced a mild traumatic brain injury, making retrospective reports of peritraumatic dissociative symptoms unreliable. To avoid this potential confound, at the initial assessment participants were asked about
current dissociative symptoms by modifying the dissociative questions of the Clinician-Administered PTSD Scale. The dissociative questions were modified by asking “How often has that happened in the past ? days,” with the interviewer inserting the number of days since intravenous narcotic analgesia had ceased.
Given the potential overlap between organic and psychogenic symptoms, care was taken to ensure that symptoms were psychogenic in origin. Both clinical assessors were sensitive to the consequences of physical injury and mild traumatic brain injury and trained to ask appropriate probes to detect differential diagnoses (i.e., whether a symptom was best accounted for by a nonpsychiatric explanation). Symptoms that were better accounted for by, for example, pain, hospital environment, or the injuries themselves were not scored as psychiatric symptoms.
In the follow-up assessments, care was taken to differentiate between various conditions such that a disorder was diagnosed only if it was not better explained by another diagnosis. For example, the reexperiencing phenomena that are characteristic of PTSD (intrusive memories of the traumatic event) were differentiated from the general ruminative worry (often about the consequences of the injuries) that is more characteristic of depression or generalized anxiety disorder. Avoidance was accepted as a PTSD symptom if it was specifically associated with attempts to avoid reminders of the trauma (i.e., functionally aimed at reducing the likelihood of activating unpleasant traumatic memories). If avoidance was engaged to prevent the occurrence of a feared outcome, and thereby reduce anxiety, it was identified with another anxiety disorder (specific phobia or panic disorder). If the avoidance was more associated with a lack of motivation and energy, it was seen as depressive phenomenology. If the avoidance was related to the current environment or physical incapacity, it was not deemed to be a psychiatric symptom. Thus, prevalence estimates of psychiatric morbidity in this study are considered to be conservative.