Gender differences in the epidemiology and course of schizophrenia are well established
(1,
2). For instance, many studies have suggested that narrowly defined schizophrenia is more common in males and that the onset occurs earlier in male patients than in their female counterparts
(3–
5). Gender differences in bipolar affective disorder have also been described. Thus, women may have a higher risk of developing rapid-cycling bipolar disorder and dysphoric or mixed mania
(6). Furthermore, women may be more likely to present with an initial depressive episode before onset of mania
(7) and to suffer from a greater number of depressive episodes and from longer, more refractory episodes throughout the course of their illness
(8,
9). However, whether there are gender differences in incidence or age at onset of bipolar disorder remains unclear.
Older studies found no consistent gender differences in age at onset of bipolar disorder
(10), but some small, more recent cross-sectional studies that have used strict operational criteria for diagnosis suggested that women may have a later age at onset of mania and bipolar disorder
(7,
11,
12). Higher incidence rates of mania in midlife have also been described
(13), but studies of mania and bipolar disorder have generally been too small to provide reliable data regarding differences in incidence or age at onset by gender. Larger incidence studies could therefore examine gender differences in incidence of bipolar disorder throughout the lifespan, evaluate likely causative factors, and possibly identify subsets of bipolar disorder patients. Previous studies showed that age at onset of bipolar disorder is of critical importance, as early-onset bipolar disorder has been associated with more severe clinical symptoms
(14,
15), comorbid substance abuse
(16,
17), a stronger family history of affective disorder
(18), and poor outcome
(16,
17,
19). Furthermore, studies investigating distributions of age at onset identified subsets of bipolar disorder patients that may be differentiated on the basis of familial transmission and clinical symptoms
(18,
20,
21). However, such studies were based on consecutive admissions or outpatient visits rather than on epidemiological samples, and thus they may be subject to referral bias. The current study, a 35-year incidence study of all psychiatric contacts (inpatient, outpatient, and community) with first-episode mania or bipolar disorder in southeast London, allowed us to investigate incidence rates and age at onset by gender in a large epidemiological sample.
Method
We identified all cases of bipolar I disorder, first manic episode, in patients who contacted psychiatric services, including inpatient, outpatient, and community referrals, in a defined catchment area, Camberwell, southeast London, an inner-city area of approximately 120,000 people (London, Office of Population Censuses and Surveys, 1997), between January 1965 and December 1999. The identified cases included those involving patients whose first presentation to services was with mania and those involving patients who presented with a first manic episode after a previously assessed or treated depressive episode in primary or secondary care. This study was approved by the South-London and Maudsley Ethical Committee.
Identification of Cases
Clinical and sociodemographic data were collected for all people from the geographically defined area of Camberwell who presented with psychosis, mania, or hypomania between 1965 and 1999. All possible cases of mania, hypomania, schizophrenic psychosis, including the schizoaffective type, paraphrenia, and “other nonorganic psychosis” were extracted from the prospectively collected Camberwell Cumulative Psychiatric Case Register
(22), which provided a comprehensive list of all persons from Camberwell who had their first contact with psychiatric services, including those not admitted, between 1965 and 1984.
From 1984 to 1999, cases were identified by generating a list from hospital computer records of all people admitted to any hospital serving the Camberwell catchment area who had any possible psychotic illness, mania, hypomania, or bipolar affective disorder, as coded by ICD-9 or ICD-10. In addition, case records of all patients from the area (1984–1999) were examined to identify those who had made contact with services but were not admitted. Patients admitted to hospitals outside the area would normally be transferred to local hospitals or services for continuing care, and these records were also identified.
To ensure that patients who initially presented to psychiatric services with major depression and later returned with mania were not missed by the Camberwell Case Register (1965–1984), which mainly recorded first contacts, we examined admission lists and ward reports for the entire follow-up period from all hospitals serving the Camberwell catchment area to identify patients with a diagnosis of mania or bipolar disorder. The compilation of this Camberwell database was previously described by Boydell et al.
(23).
Diagnostic Procedure
Patients who were not residents in the catchment area, had presented previously with a psychotic or manic episode, had a clear organic cause for their symptoms, or had onset before age 16 years were excluded from this study. Case records of the remaining subjects, including medical, nursing, social work, and occupational therapy notes, together with all correspondence relating to the case, were examined, and the Operational Checklist for Psychotic Disorders, Version 3.4
(24) was completed for each case by one experienced psychiatrist (N.K.) for the year after the patient’s presentation. The Operational Checklist for Psychotic Disorders is a well-validated symptom checklist that is based on the phenomenological descriptions in the Present State Examination
(25). It has a glossary of clear and explicit descriptions for each constituent item of psychopathology and instructions for coding the items and was designed with case-note review in mind. Checklists prepared with this instrument were used to generate DSM-IV diagnoses by using the accompanying computer program. The patients who met the criteria for a DSM-IV diagnosis of bipolar I disorder, first manic episode, which included patients who experienced an episode of depression before onset of mania, were included in the analyses for this study.
Clinical and Sociodemographic Variables
Clinical and sociodemographic variables were extracted from case notes by an experienced psychiatrist (N.K.), who used a pro forma document, as described by Castle et al.
(26). The age at onset of DSM-IV mania was defined according to Operational Checklist for Psychotic Disorders guidelines as the age at which first psychiatric contact was sought for mania. The age at onset of DSM-IV bipolar disorder was defined as the age at which treatment was first sought in primary or secondary care for any affective disorder, including major depression. Ethnicity was classified according to the ethnicity category stated by the patient. For analysis, ethnicity was divided into a white group (self-assigned ethnicity white) and a nonwhite group (all other self-assigned ethnicities). In the absence of a statement of self-assigned ethnicity, the patient’s and his or her parents’ place of birth, if available, and any description of color was used to determine ethnicity. Premorbid functioning in work and social areas and premorbid personality disorder were rated according to Operational Checklist for Psychotic Disorders criteria. Obstetric complications were rated according to the scale devised by Lewis and Murray
(27), and family history of psychotic or affective disorder was rated according to Operational Checklist for Psychotic Disorders guidelines. Childhood antisocial traits or behavior were identified if the patient met the DSM-IV criteria for conduct disorder (persistent aggression to people or animals, destruction of property, deceitfulness or theft, or serious violation of rules). Childhood neurotic traits, antisocial traits, and juvenile delinquency were rated as described by Castle et al.
(26). To assess interrater reliability for the variables described here, including age at onset of mania and bipolar affective disorder in 5-year bands, a random subset of 60 case notes was rated independently by another author (S.K.); results ranged between kappa 0.85 and 1.00 for different variables.
Denominator Data
Incidence rates of DSM-IV bipolar I disorder, first manic episode, by gender were determined by 5-year age bands across the study period (1965–1999) by using data supplied from the Office for Population Censuses and Surveys. Population data concerning the general population of Camberwell were generated from the 1961, 1971, 1981, and 1991 censuses (100% samples) and were stratified by age and gender (London, Office for Population Censuses and Surveys and London Research Centre, 1997). Population estimates for the intermediate years were interpolated, and corrections were made for underenumeration throughout the entire time period. The male-female ratio of the general population of Camberwell remained fairly uniform throughout the period of study, with a slight female preponderance (London, Office for Population Censuses and Surveys, 1997).
Statistical Analysis
Overall incidence rates and rate ratios by gender and age for 10-year age-at-onset bands were calculated by using the StATA statistical program
(28). Mean differences in age at onset for first-episode mania and bipolar disorder by gender, family history, developmental variables, premorbid functioning, personality variables, and ethnicity were assessed with the Mann-Whitney U test because of the positive skew in the distribution of age at onset. Variables with significant or near-significant results were then entered into analysis of covariance (ANCOVA) with age at onset as the dependent variable. In this analysis, age at onset of mania and bipolar disorder were log transformed to remove skewness from the data. Associations between gender and individual premorbid variables were then sought by using chi-square tests.
Results
Age at Onset by Gender
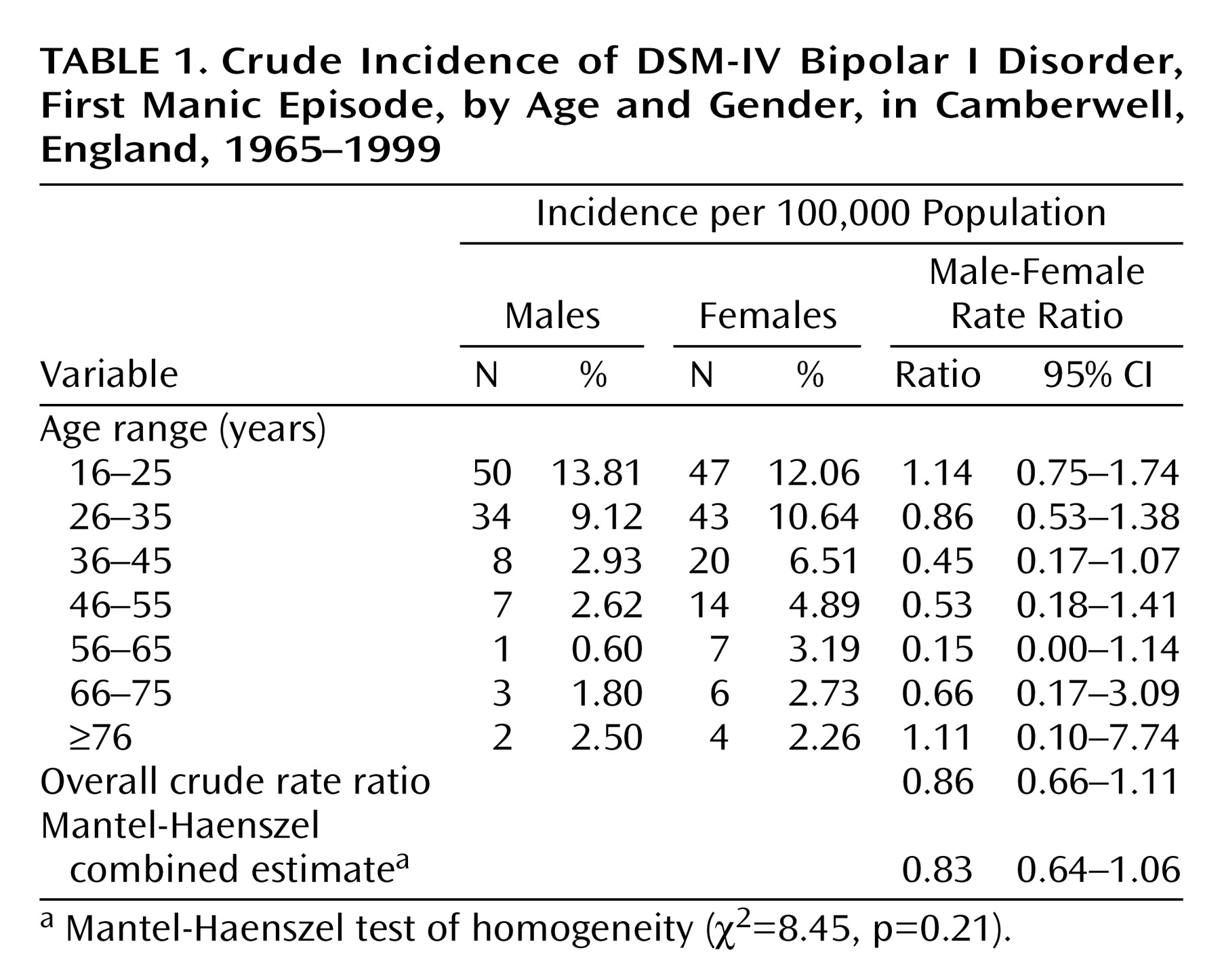
Of the 1,443 cases rated for the entire 35-year period, 246 involved patients who met the criteria for DSM-IV bipolar I disorder, first manic episode, of whom 52 (21.1%) had been treated for a previous episode of DSM-IV depression. One hundred forty-one patients (57%) were female, and 105 (43%) were male (rate ratio=1.21, 95% confidence interval (CI)=0.94–1.56). One hundred forty-nine patients (60.6%) were of white European ethnicity, 52 (21.1%) were African Caribbean, 33 (13.4%) were African, and 12 (4.9%) were from other ethnic groups.
The mean age at onset for mania was 32.9 years (SD=15.3, median=28); age at onset was later for women (mean=35.1 years, SD=16.2, median=31) than for men (mean=30.0 years, SD=13.4, median=26) (Z=–2.72, p=0.007, Mann-Whitney U test). The mean age at first contact with a health professional for bipolar disorder was 31.2 years (SD=14.9, median=26); first contact was later for women (mean=33.1 years, SD=15.6, median=28) than for men (mean=28.7 years, SD=13.6, median=25) (Z=–2.60, p=0.009, Mann-Whitney U test).
Almost one-half (48%, N=50) of the male patients had onset of mania by age 25 years and 80% (N=84), by age 35 years, whereas only a one-third (N=47) of the female patients had onset by age 25 years and 64% (N=90), by age 35 years. Similarly, the peak age at onset of bipolar disorder was earlier in men: 56% (N=59) had onset by age 25 years and 83% (N=87), by age 35 years, compared with 37% (N=52) and 68% (N=96), respectively, in women.
To examine whether differences in age at onset were consistent across the 35-year period of this study, gender differences in age at onset of first-episode mania or bipolar disorder were examined by using 5-year date bands. Age differences were consistently observed, with female patients having a later onset of mania and bipolar disorder during six of the seven date bands (mean difference=1.7–11.0 years) and male patients having a marginally later onset during one band.
Overall Incidence Rates for DSM-IV Bipolar I Disorder, First Manic Episode, by Gender
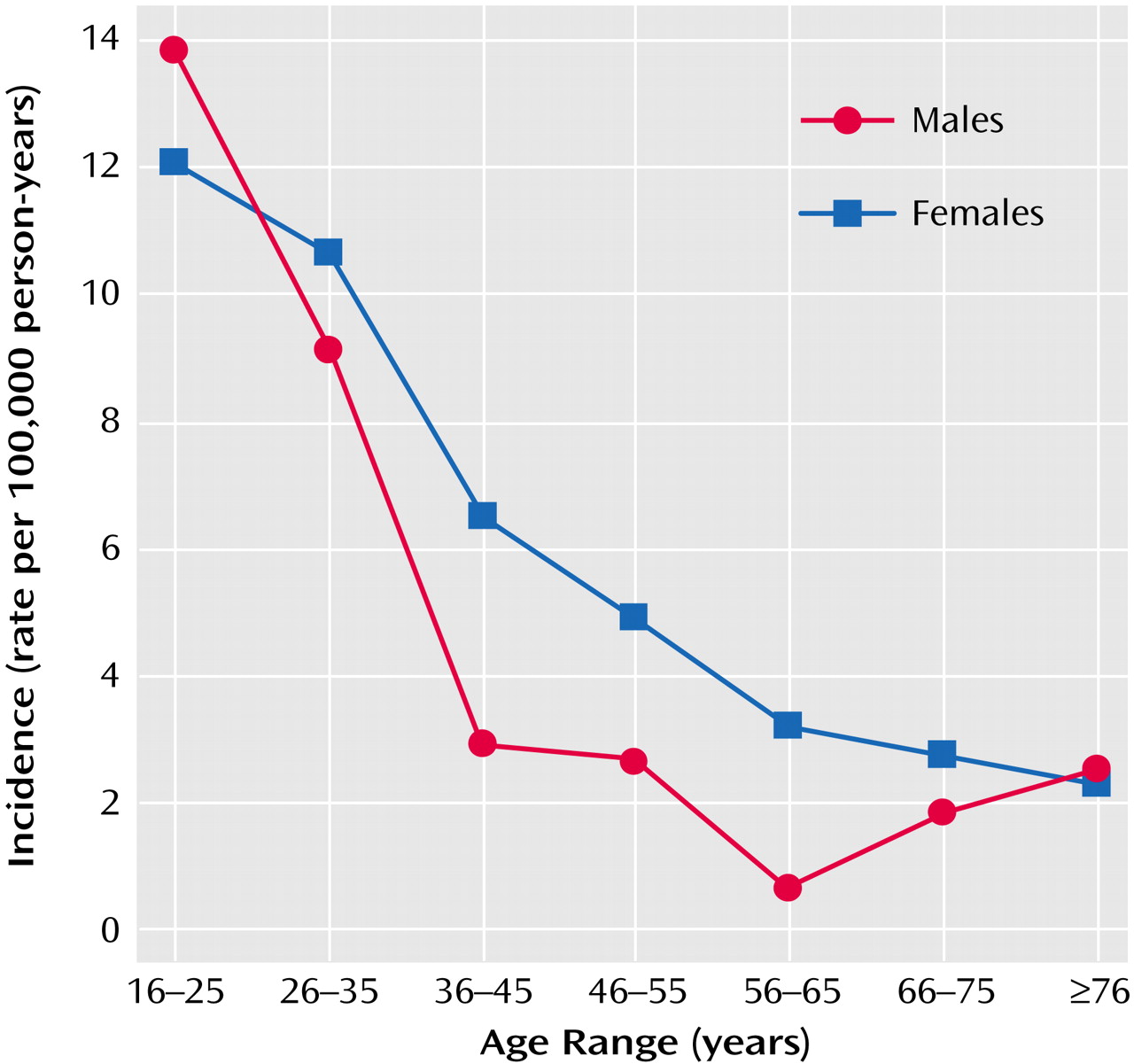
Figure 1 shows the incidence by 10-year age-at-onset bands for bipolar I disorder, first manic episode. The incidence for males peaked in the 16–25-year-old age group and fell dramatically in successive age bands, whereas the incidence was lower for females in the 16–25-year-old age group but did not fall as dramatically thereafter. Incidence was higher for females in all age bands, except for the 16–25 and ≥76 age bands (
Table 1). Male-female rate ratios were <1 for each age band, with the exception of the youngest and eldest bands, although gender differences in incidence in the individual bands did not reach statistical significance.
Influence of Psychosocial Variables on Gender Differences in Age at Onset
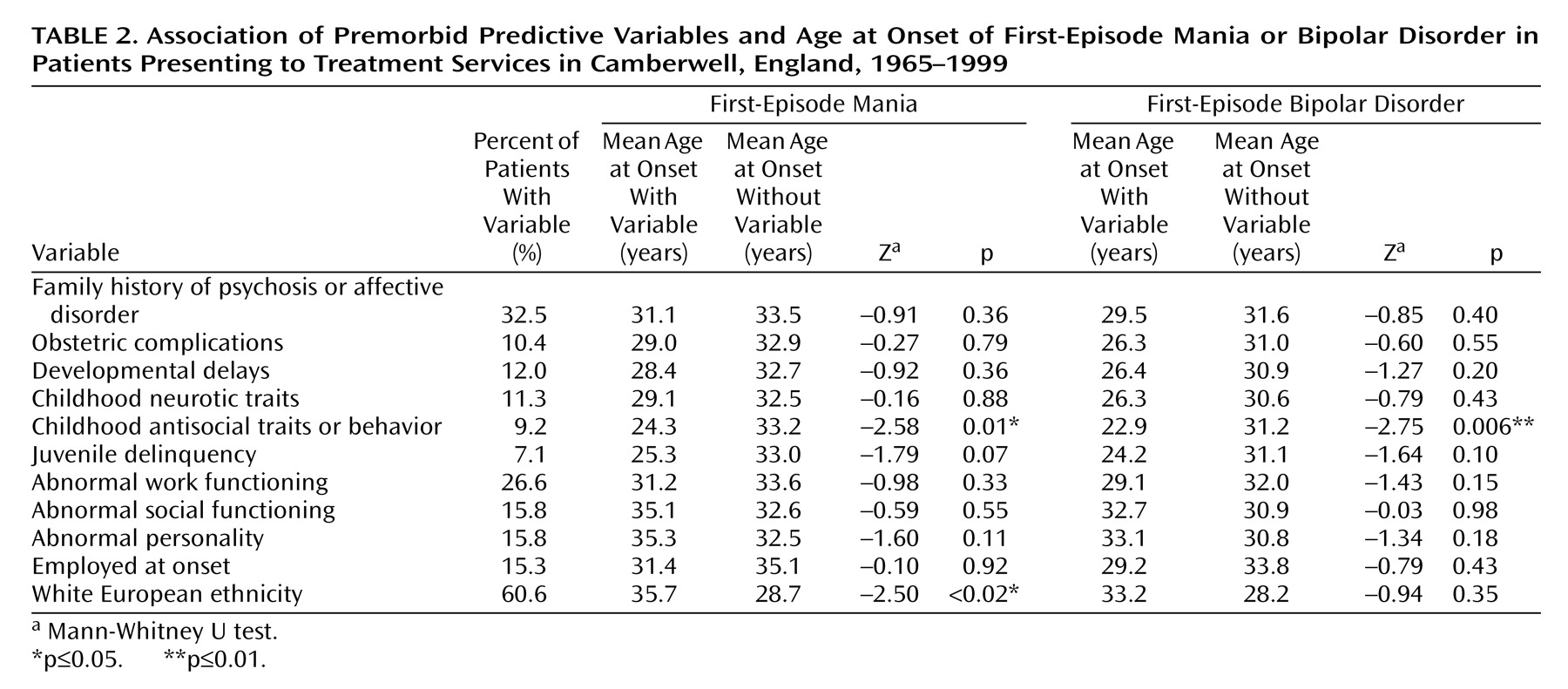
Associations between selected premorbid psychosocial variables, including family history, developmental variables, premorbid functioning, personality and ethnicity, and age at onset of first-episode mania or bipolar disorder were sought 1) to ascertain whether any of these variables were associated with age at onset and 2) to identify whether they would influence gender differences in age at onset. As
Table 2 shows, childhood antisocial traits or behavior and nonwhite ethnicity were associated with younger age at onset of mania; childhood antisocial traits were associated with age at onset of bipolar disorder, with juvenile delinquency and abnormal personality nearing statistical significance on these measures.
Variables for which significant or near-significant differences were found in the univariate analysis were entered into ANCOVA models along with gender and with log-transformed age at onset of first-episode mania or bipolar disorder as the dependent variable. In multivariate analysis, ethnicity (F=9.50, df=1, 217, p=0.002), gender (F=5.3, df=1, 217, p<0.03), and childhood antisocial behavior (F=5.9, df=1, 217, p<0.02) emerged as significant independent predictors of age at onset, when age at onset of first-episode mania was used as the dependent variable; childhood antisocial behavior (F=4.3, df=1, 217, p=0.04) and gender (F=3.9, df=1, 217, p<0.05) were significant predictors of age at onset, when age at onset of bipolar disorder was used as the dependent variable.
When the relationship between gender, ethnicity, and childhood antisocial behavior was investigated, male gender was found to be significantly associated with childhood antisocial behavior (χ2=5.46, df=1, p<0.02), although no other significant associations were found. No significant interactions between these three variables and age at onset of mania or bipolar disorder were identified.
Discussion
We found a robust association between gender and age at onset of first-episode mania and bipolar disorder. Men had an earlier age at onset, even after adjustment for premorbid variables. In multivariate analysis, childhood antisocial behavior remained independently associated with earlier onset of mania and bipolar disorder, and nonwhite ethnicity remained independently associated with earlier onset of mania. Men also had a higher incidence of bipolar disorder in early adult life, and women had a higher incidence throughout the rest of adult life until late life, although these differences did not reach statistical significance for individual age bands.
The association of male gender and childhood antisocial behavior with early onset of bipolar disorder raises the possibility of a subgroup of early-onset, predominantly male bipolar disorder patients with behavioral difficulties. Antisocial behavior in childhood could be a manifestation of neurodevelopmental abnormality or even of early-onset bipolar disorder. The findings in this study were strikingly similar to those reported by Carlson et al.
(16), who compared 23 early-onset (age <21 years) with 30 later-onset (age >30 years) patients with psychotic mania and found that early onset was associated with male gender and childhood behavioral difficulties. Other studies have also reported associations between early-onset bipolar disorder and neurodevelopmental or psychosocial impairment
(29,
30). The higher incidence of bipolar disorder in men in early adult life, in contrast to the rest of adult life, in this study also supported a predominantly male early-onset subgroup. However, the interpretation must be made with caution, as only 10% of cases with an early onset (age <25 years) both reported childhood antisocial behavior and were male. By contrast, the association between nonwhite ethnicity and early-onset mania is likely to be due to younger age distributions in ethnic minority groups, compared with the white European population, over the course of this study.
Most of the older studies that investigated age at onset of bipolar disorder by gender found no significant differences between men and women, although a minority of studies found a later mean age at onset in women
(10). More recent studies, which have used strict operational criteria for diagnosis, have mainly found a later onset of bipolar disorder in women
(6). Thus, Viguera et al.
(7), in a study of 360 outpatients with DSM-IV bipolar I disorder or bipolar II disorder, found that women were a mean of 3.2 years older at onset than men. Another study of 69 subjects mainly with bipolar I disorder found that women had significantly older age at onset of both depression and mania
(11). Finally, a recent study of bipolar I disorder patients in the suburbs of London found that onset in women occurred a mean of 8.3 years later than in men
(12). The current study showed that onset of bipolar disorder and mania in women occurred a mean of 4.4 years later and 5.1 years later, respectively, than in men; these results add weight to previous findings suggesting a gender difference in age at onset of bipolar disorder.
A number of studies have also shown that the onset of schizophrenia occurs approximately 4–5 years later in female patients than in male patients
(4,
5,
26). However, incidence and age-at-onset distributions appear to be different in bipolar disorder and schizophrenia. In this study we found that women had a somewhat higher incidence of bipolar disorder throughout adult life, except in early life and late life. Similar findings have been described in national admission data
(13,
31). By contrast, in schizophrenia, male patients predominate among those with an early onset, and a marked excess of female patients is found among those with an onset in late life
(4,
26). The higher incidence of schizophrenia in early life among men, compared with women, has largely been explained by a greater likelihood that abnormal neurodevelopment affects men, because of later brain maturation, and by the protective effects of higher estrogen levels in women
(32,
33). The high incidence in late life in women may in turn be related to the decrease in the level of estrogen during menopause
(33). However, hormonal effects of estrogen are unlikely to have mainly accounted for the gender differences in onset of bipolar disorder observed in this study, as the incidence of bipolar disorder continued to decline even after menopausal age in women and the incidence of bipolar disorder remained higher in women than in men until late adult life.
Gender differences in age at onset of mania and bipolar disorder could also have been related to women’s seeking assessment or treatment later than men. One study has shown that women are more likely than men to have delays in receiving a prescription for maintenance treatment for bipolar disorder and in receiving a diagnosis of bipolar disorder
(7). However, delays in assessment, particularly for mania, are less likely. Stressful life events that may differentially affect women, particularly pregnancy and the puerperium, have been associated with onset of mania
(34). However, postpartum psychosis was unlikely to have contributed to the higher incidence among women in adult life in this study, as only five incident cases of first-episode mania occurred within 1 month of delivery and three of these cases were in the youngest age band, in which the incidence in males was higher. Similarly, other possible psychosocial factors such as unemployment or abnormal work or social functioning were not associated with either gender or age at onset of bipolar disorder in this study. Furthermore, gender differences in migration patterns were unlikely to have markedly influenced differences in age at onset, as gender differences in age at onset in nonwhite groups were less pronounced than in white Europeans. However, the influence of other social factors, which may particularly affect young men, including urban living, social deprivation, and alcohol or illicit drug abuse, cannot be discounted.
The main strengths of this study were that we identified all psychiatric contacts, not just contacts that resulted in admission or contacts involving cases of psychotic disorders, in an epidemiologically defined catchment area. Our sample was therefore representative of first-onset bipolar disorder, and our findings are more likely to be generalizable than are those of previous studies of age at onset. The design of the current study allowed us to estimate incidence rates of first-episode mania by age and gender, by using adjusted population data. Furthermore, the long time frame of this study allowed identification of a large number of incident cases, despite the relatively low incidence of bipolar I disorder in the general population. Diagnostic stringency was ensured by using computer-generated diagnoses. Finally, potentially confounding premorbid variables were considered.
The main limitation was the high proportion of missing case notes for the early years of the study. Almost 10% of the case notes for the first 10 years of the study period were missing, compared with less than 3% for the subsequent 25 years. However, if adjustment was made for missing notes in proportion to the number of cases examined, only approximately another 14 cases would have been detected, and the additional data would have been unlikely to affect the gender differences found in this study. This study was also confined to adult cases, as the original Camberwell Case Register identified only patients age 16 years or older at first contact. Therefore, the incidence of childhood-onset bipolar disorder in Camberwell could not be evaluated. Furthermore, over the long study period, the style or content of the case records may have changed, given the evolving nature of diagnosis and classification. However, in practice, case records compiled in the Bethlem and Maudsley Hospitals have used a standardized format that has varied little since the early 1970s
(35).
Significant gender differences in age at onset of mania and bipolar disorder were observed in this study, and these differences persisted even after adjustment for potentially confounding variables. Furthermore, childhood antisocial behavior remained independently associated with early onset, raising the possibility of the existence of an early-onset bipolar subgroup.
These findings need replication in large-scale prospective epidemiological studies in which putative causal mechanisms could be further explored.