Gender Differences
No significant gender differences were found in age (women: mean=24.7 years, SD=7.8; men: mean=29.8 years, SD=12.4), number of years smoked (women: mean=5.6, SD=4.8; men: mean=7.9, SD=8.0), Fagerström scores (women: mean=3.0, SD=0.3; men: mean=4.5, SD=2.5), arterial nicotine values (women: mean=3.3 ng/ml, SD=2.6; men: mean=2.6 ng/ml, SD=2.3), and arterial cotinine values (women: mean=91.3 ng/ml, SD=62.3; men: mean=110.6 ng/ml, SD=59.5) (unpaired, two-tailed t tests, p>0.05). However, the average number of cigarettes smoked per day was higher in men than in women (men: mean=19.0, SD=6.6; women: mean=13.5, SD=3.0) (t=2.47, df=17, p=0.02). There was no main effect of gender on rCBF responses (unpaired, two-tailed t tests, p>0.05), and therefore the data for men and women were combined for all analyses.
Visual Analogue Scale Scores
The only statistically significant change in visual analogue scale scores from before smoking to after smoking was a decrease in the score for craving from before to after the first cigarette (mean=5.1, SD=2.6, to mean=2.8, SD=2.5) (t=2.11, df=16, p<0.01). There was no change in craving from before to after the second average-nicotine cigarette or from before to after the denicotinized cigarette. Furthermore, there were no changes in score for feeling relaxed, sick, wakeful, and nervous from pre- to postsmoking for any cigarette. To determine whether the average-nicotine and denicotinized cigarettes had similar effects on these measures, we conducted an unpaired t test comparing the change in visual analogue scale scores from before to after the second average-nicotine cigarette for those who smoked it second and from before to after the denicotinized cigarette for those who smoked it second. In this way, the previous experience was held constant—i.e., both groups had smoked an average-nicotine cigarette 24 minutes earlier. No significant differences were found, although a difference in scores indicating an increase in sickness after the second average-nicotine cigarette but not after the denicotinized cigarette approached significance (t=2.03, df=17, p=0.06).
Pharmacokinetic and Cardiovascular Data
Peak plasma levels of nicotine were higher during the second average-nicotine cigarette than during the first (mean=59 ng/ml, SD=38, versus mean=41 ng/ml, SD=21) (t=2.85, df=16, p<0.05). Given that the half-life of nicotine is greater than 1 hour, this difference was presumably related to carryover effects, because subjects smoked the second average-nictone cigarette 24 or 48 minutes after the first. However, the increase in peak plasma levels of nicotine from before to after smoking was not significantly different between the first and second average-nicotine cigarettes (mean=40 ng/ml, SD=21, and mean=52 ng/ml, SD=37, respectively) (t=–1.86, df=15, p=0.08). Compared to the peak plasma level of nicotine associated with the denicotinized cigarette, the peak plasma levels of nicotine were much greater for both the first average-nicotine cigarette (mean=16 ng/ml, SD=8, versus mean=43 ng/ml, SD=20) (t=6.98, df=16, p<0.001) and the second average-nicotine cigarette (16 ng/ml, SD=9, versus mean=61 ng/ml, SD=38) (t=5.41, df=15, p<0.001). The increase in peak plasma nicotine levels from pre- to postcigarette was also much greater for the first average-nicotine cigarette than for the denicotinized cigarette (mean increase=40 ng/ml, SD=20, versus mean increase=3 ng/ml, SD=3) (t=7.77, df=16, p<0.001) and for the second average-nicotine cigarette than for the denicotinized cigarettes (mean increase=54 ng/ml, SD=37, versus mean increase=3 ng/ml, SD=3) (t=5.58, df=14, p<0.001).
Because the half-life of nicotine is 1 hour and the order of the second average-nicotine cigarette and denicotinized cigarette was randomized between subjects, there was some concern that this aspect of the study design may have resulted in a large carryover effect for subjects who smoked the denicotinized cigarette third, given that they had already smoked two average-nicotine cigarettes. For this reason, we looked at the differences in peak nicotine level after the denicotinized cigarette between those who smoked it second and those who smoked it third. We found no significant difference (mean=14 ng/ml, SD=9, versus mean=20 ng/ml, SD=7 ng/ml) (t=1.71, df=15, p=0.11). There was also no significant difference in peak nicotine level after the second average-nicotine cigarette between those who smoked it second and those who smoked it third (mean=53 ng/ml, SD=33, versus mean=64 ng/ml, SD=44) (t=–0.61, df=15, p=0.54).
There were no significant differences in peak heart rate, diastolic blood pressure, or systolic blood pressure after smoking the first versus the second average-nicotine cigarette. Compared to smoking the denicotinized cigarette, smoking the first average-nicotine cigarette resulted in a significant increase in heart rate (mean=84 bpm, SD=8, versus mean=97 bpm, SD=11) (t=5.65, df=16, p<0.05) and systolic blood pressure (mean=126, SD=13, versus mean=128, SD=14) (t=2.32, df=16, p<0.05), but not diastolic blood pressure (mean=67, SD=11, versus mean=68, SD=8) (t=1.43, df=16, p=0.17), and the second average-nicotine cigarette resulted in a significant increase in heart rate (mean=84 bpm, SD=9, versus mean=95 bpm, SD=10) (t=7.17, df=15, p<0.001) and systolic blood pressure (mean=126, SD=13, versus mean=129, SD=11) (t=3.30, df=15, p<0.01), but not diastolic blood pressure (mean=67, SD=11, versus mean=69, SD=11) (t=2.01, df=15, p=0.06).
rCBF
Partial data were lost for three female subjects. Because of computer failures during data acquisition, data from the baseline scan were lost for one subject and data from the scan during the first average-nicotine cigarette were lost for another subject. Data from the scan during the second average-nicotine cigarette were lost for a third subject because of radiotracer synthesis failure. The remaining data for each subject were used for the following analysis.
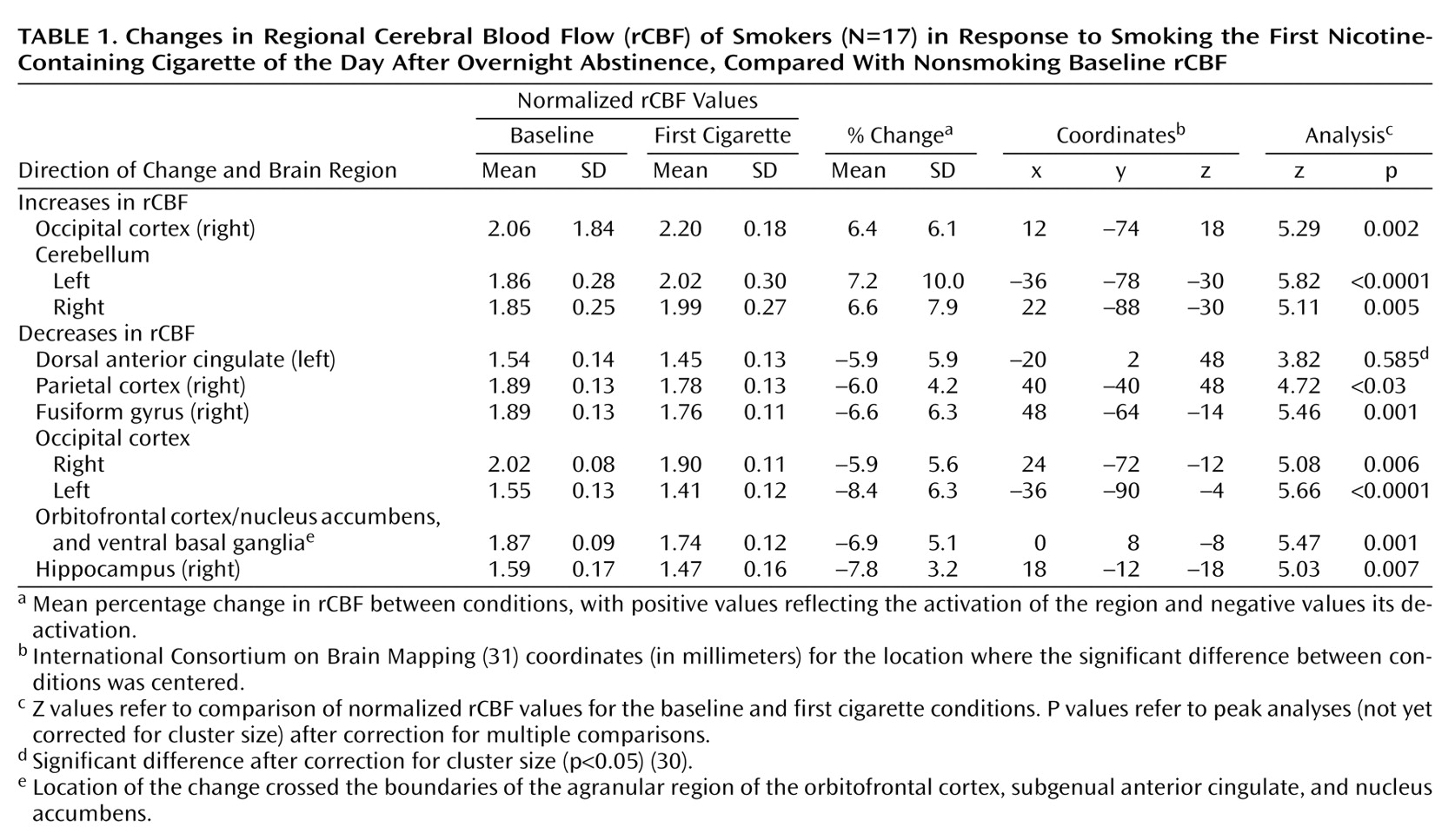
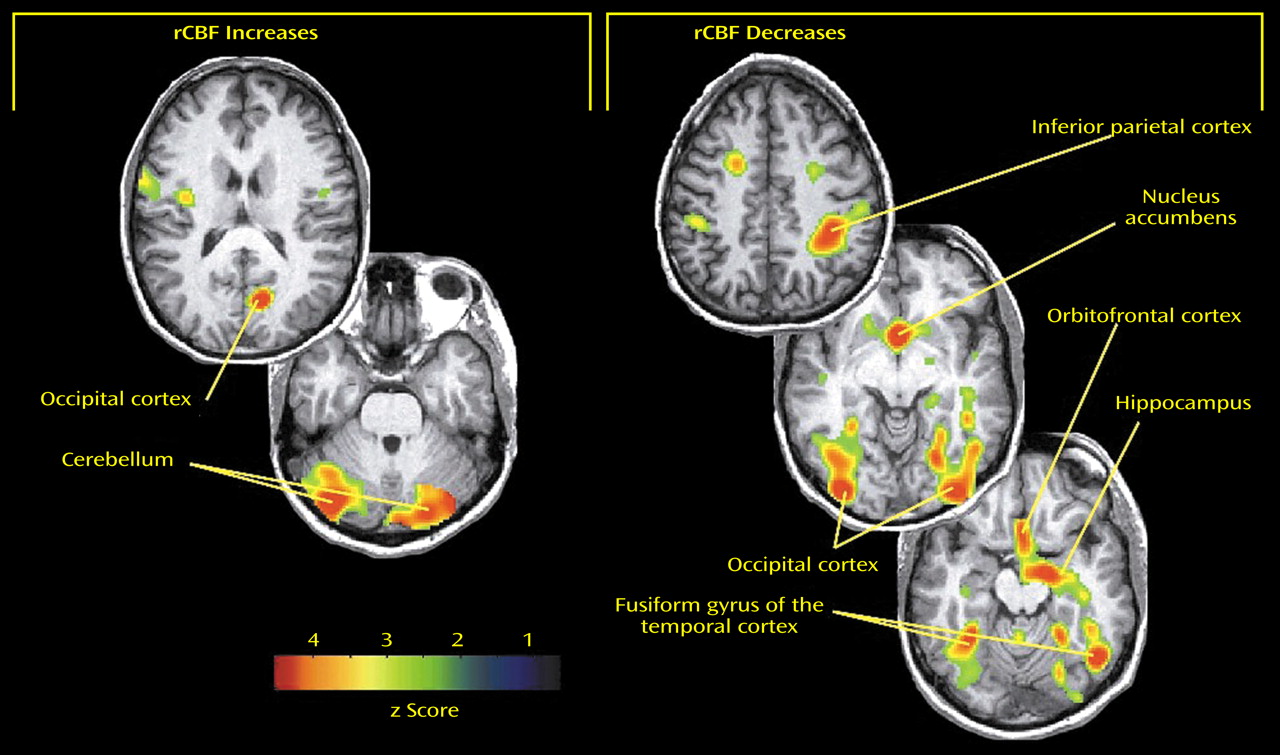
Significant differences in rCBF from the initial baseline scan to the scan during the first average-nicotine cigarette were observed (
Table 1 and
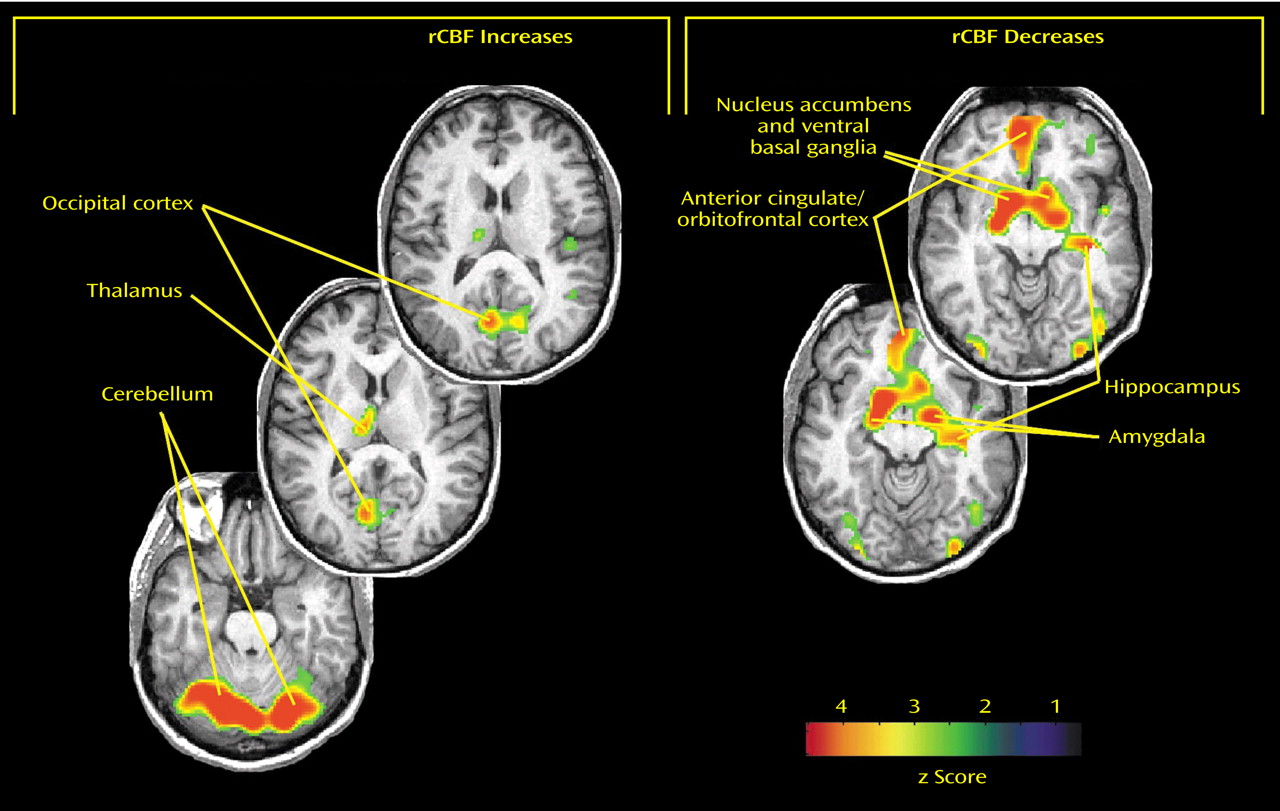
Figure 1). Significantly higher rCBF during the first average-nicotine cigarette, compared to the preceding baseline, was observed in the right occipital cortex (Brodmann’s area 17/18) and the cerebellum bilaterally. Significant reductions in rCBF during the first cigarette were observed in the occipital cortex bilaterally (Brodmann’s area 18/19), right parietal cortex (Brodmann’s area 1/2), right fusiform gyrus, and right hippocampus and in a large area that overlapped both the ventral anterior cingulate (Brodmann’s area 25) and the nucleus accumbens bilaterally. When the size of the region involved was taken into account with cluster-level correction for multiple comparisons
(30), the left dorsal anterior cingulate (Brodmann’s area 32/24) also showed decreased rCBF during the first cigarette, compared to baseline.
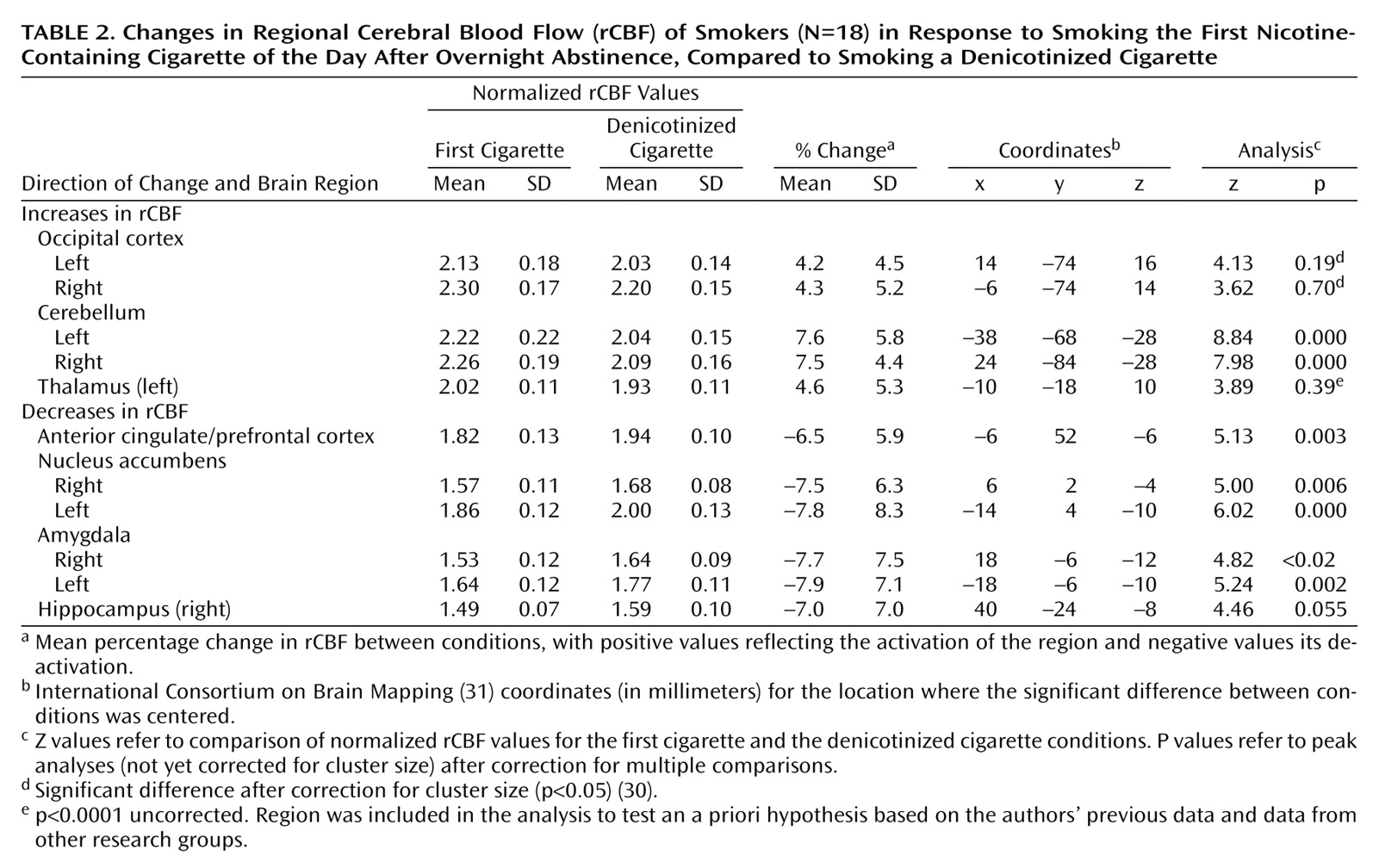
Differences in rCBF between the scan during the first cigarette of the day and the scan during the denicotinized cigarette were also tested for statistical significance to determine the effect of smoking the first cigarette of the day, with control for nonnicotine aspects of smoking (
Table 2 and
Figure 2). Significantly higher rCBF during the first average-nicotine cigarette, compared to the denicotinized cigarette, was observed in the cerebellum bilaterally. With cluster-level correction for multiple comparisons, the bilateral occipital cortex (Brodmann’s area 17/18) also showed increased rCBF. Furthermore, the left thalamus, an area for which we had an a priori hypothesis based on our previous data and those from other groups, registered enhancements in rCBF during the first cigarette, compared to the denicotinized cigarette. These increases in rCBF were slightly below the standard threshold of significance after correction for multiple comparisons (p<0.0001, uncorrected). It is noteworthy that lower rCBF during the first cigarette, compared to the denicotinized cigarette, was observed in the nucleus accumbens bilaterally, the left rostral and ventral anterior cingulate and the adjacent prefrontal cortex (Brodmann’s area 10/25/32), the amygdala bilaterally, and the right hippocampus.
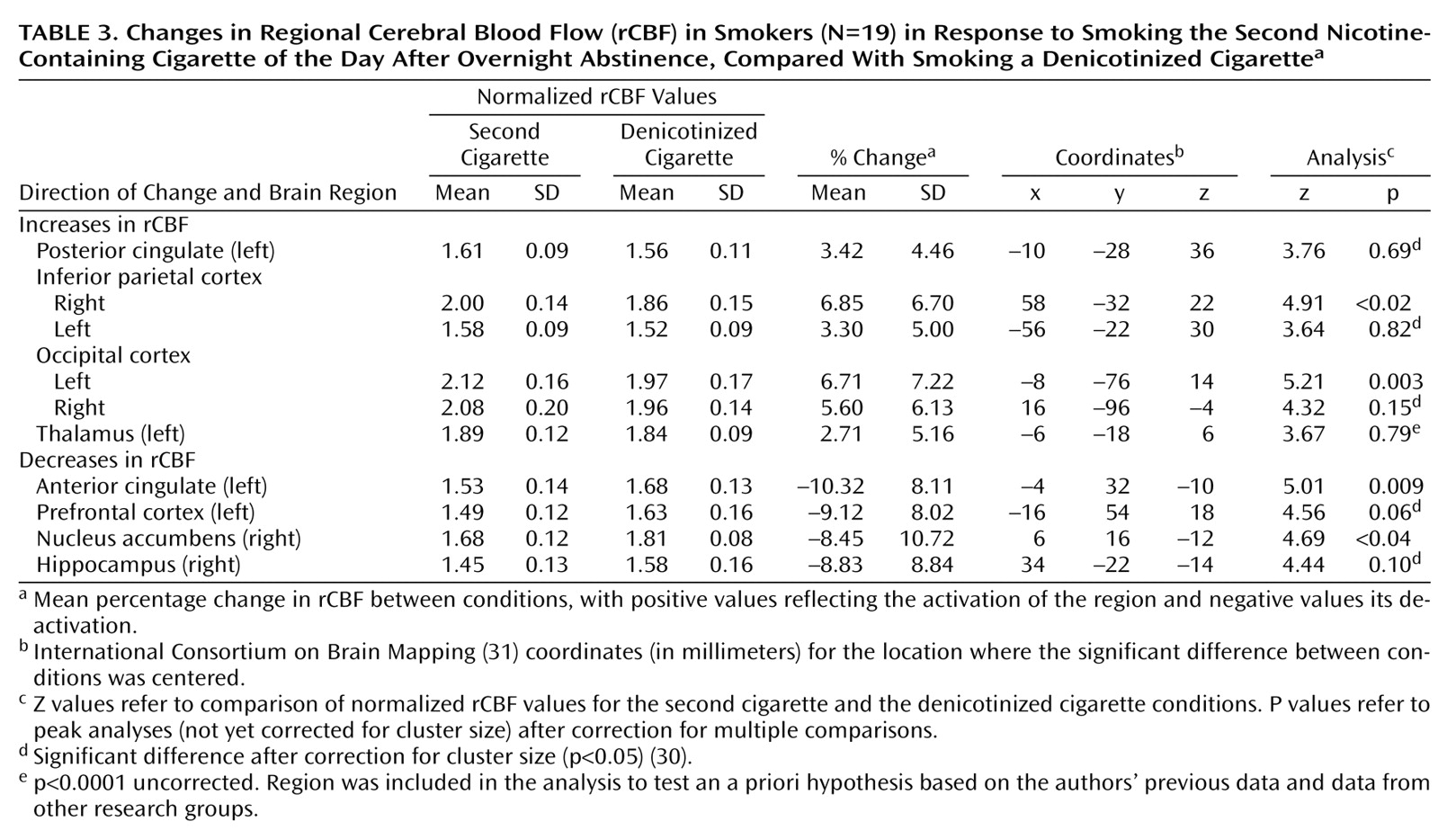
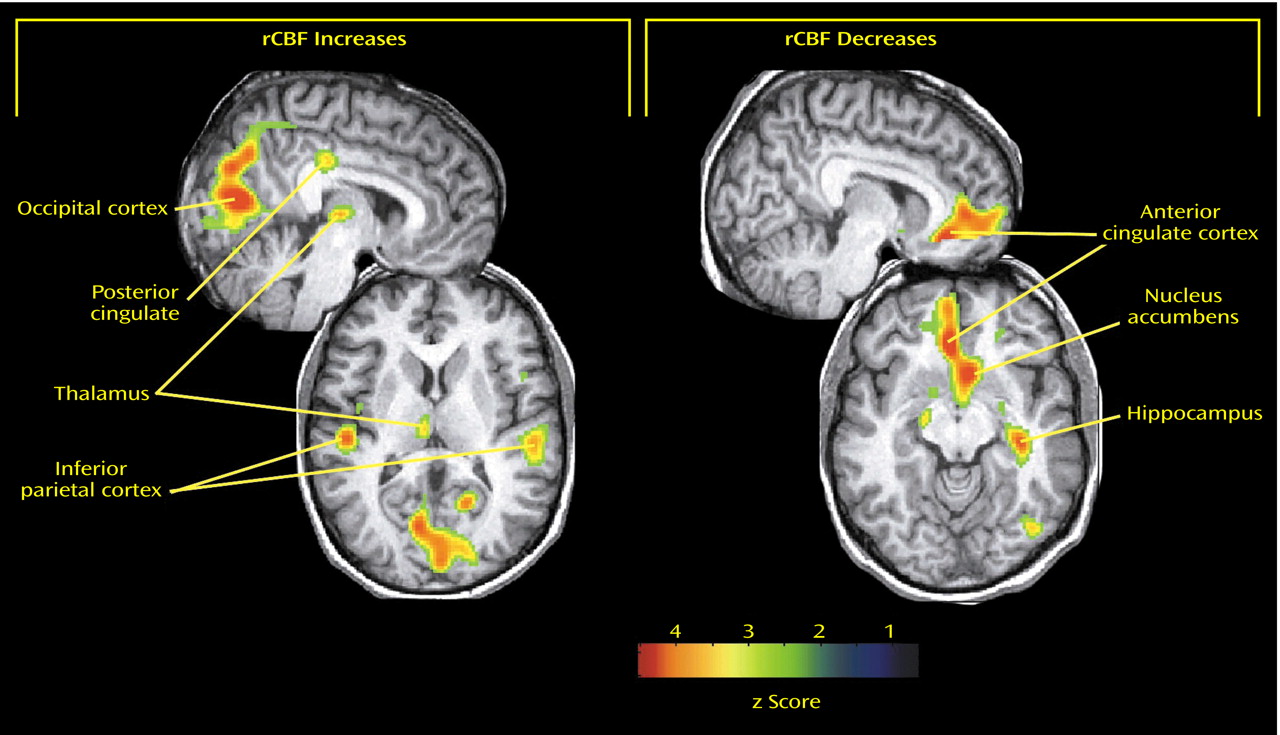
We then determined the effect of subsequent cigarette smoking by comparing rCBF responses during the second average-nicotine cigarette to those during the denicotinized cigarette (randomized order of conditions) (
Table 3 and
Figure 3). Significantly higher rCBF during the second average-nicotine cigarette, compared to the denicotinized cigarette, was observed in the left occipital cortex (Brodmann’s area 17/18) and the right inferior parietal lobe (Brodmann’s area 40). When the size of the region involved was taken into account with cluster-level correction for multiple comparisons, the right occipital cortex (Brodmann’s area 17/18), left inferior parietal lobe (Brodmann’s area 40), and posterior cingulate (Brodmann’s area 31/23) also showed increased rCBF. Furthermore, the left thalamus registered higher rCBF responses to the second average-nicotine cigarette, compared to the denicotinized cigarette, that were slightly below the standard threshold of significance after correction for multiple comparisons (p<0.0001, uncorrected). Significant reductions in rCBF during the second cigarette, compared to the denicotinized cigarette, were observed in the left rostral and ventral anterior cingulate and adjacent prefrontal cortex (Brodmann’s area 9/10/25/32) and in the right nucleus accumbens. When the size of the region involved was taken into account with cluster-level correction for multiple comparisons, the right hippocampus also showed decreased rCBF in this analysis.
The differences in rCBF responses (both increases and reductions) between the first and second average-nicotine cigarettes were then tested for statistical significance. The first cigarette of the day induced more prominent rCBF increases in the cerebellum bilaterally. In addition, the first cigarette of the day was associated with more prominent reductions in rCBF in the ventral pallidum bilaterally, extending to the nucleus accumbens, compared to the second cigarette of the day (p<0.0001, uncorrected).
As reported earlier, the only statistically significant change in visual analogue scale scores was a decrease in craving from before to after the first cigarette. To further examine this finding, a correlation analysis was performed between the significant changes in rCBF from baseline to the first cigarette (
Table 1) and the change in visual analogue scale craving scores during this time (Pearson’s correlations, p<0.05). The decrease in craving from baseline to after the first cigarette was smoked was correlated with the decrease in rCBF in the left dorsal anterior cingulate (r=0.49, N=17, p<0.05) and the right hippocampus (r=0.50, N=17, p<0.05).