Speech disturbances have long been identified as a characteristic trait of schizophrenia, with reports dating back to the time of Kraepelin
(1) and Bleuler
(2). Earlier conceptualizations based on aphasia models
(1) were later replaced by theories that language dysfunction in schizophrenia reflected an underlying disorder of thought process
(2,
3). Over the past few decades, there has been increased interest in clarifying whether schizophrenia involves a primary language problem that is independent of formal thought disorder (i.e., deviant language that can be separated from abnormal thoughts
[4]). Although it remains unclear to what extent language abnormalities and thought disorder are dissociable
(5), there is increasing behavioral evidence that schizophrenia involves a primary disruption in language (e.g., references
6,
7). This conceptualization is further substantiated by findings in schizophrenia of structural and functional brain abnormalities in regions traditionally linked with language functions, such as the superior temporal gyrus
(8,
9) and its subcomponents
(10,
11), e.g., the planum temporale
(12–
14) and Heschl’s gyrus
(12,
15).
Language is a complex cognitive process comprising several components that generally include 1) phonology (production and processing of individual speech sounds), 2) semantics (meaning of words), 3) orthographics (visual representation of words), 4) lexical processing (integration of phonology, semantics, and syntax), 5) pragmatics (social/global uses of language), 6) articulation (vocal expression through motor acts), 7) grammar (language structure), and 8) prosody (e.g., melody/tone) (see references
16–18). With the advent of neuroimaging techniques, researchers have begun to examine the neural correlates of various aspects of language
(19,
20). There is extensive behavioral evidence of sex differences across many of these language components in healthy adults
(21,
22). Generally, adult women exhibit a relative advantage over men in verbal/associational fluency
(22), lexical and prelexical processing
(23), efficiency of phonological processing
(24), and perceptual speed
(25). These behavioral differences are consistent with results from imaging studies showing normal sexual brain dimorphisms in regions subserving language, such as the superior temporal gyrus
(26–
28) and Broca’s area
(28,
29), which are larger (relative to cerebrum size) in women than men. Functional imaging studies of phonological processing have revealed greater bilateral activation of Broca’s area in women and greater left-lateralized activation in men
(30,
31).
Schizophrenia is well known to be marked by abnormalities in temporoparietal and frontal brain regions (for review, see reference
11), which are believed to disrupt language functions and higher-order cognitive problems (e.g., frontal/executive systems dysfunction) that affect language functions, respectively. In light of these neuroanatomic abnormalities, it is not surprising that schizophrenia is characterized by cognitive dysfunction across a variety of domains
(20,
32,
33), making it difficult to disentangle the degree to which language or other cognitive problems may be due to thought disorder versus impairments in other affected cognitive domains
(34), such as attention
(35–
37), frontal/executive control
(38,
39), processing speed
(40), information processing
(41), and intellectual functioning (for review, see reference
42). This difficulty highlights the importance of considering potentially confounding cognitive factors when examining language dysfunction in schizophrenia.
It is interesting to note that language functions (e.g., semantic fluency
[43]) and related brain regions (e.g., Heschl’s gyrus and the planum temporale [
12,
44,
45]), in which sex differences have been reported in healthy adults, are aberrant in schizophrenia. Moreover, as with healthy adults, research with schizophrenia patients has demonstrated sex differences in some aspects of verbal functions (e.g., reference
46). Male schizophrenia patients performed more poorly on measures of verbal learning, verbal fluency
(47), and verbal memory
(48,
49), compared to female schizophrenia subjects, although findings were not consistent
(49–
51). Male patients had an advantage on spatial relative to language tasks, compared to female patients, who performed similarly across these domains
(52).
The literature includes some inconsistencies that raise questions about the general proposition of sex differences in cognition in schizophrenia
(53). For example, some studies have found worse cognitive performance among female patients
(50) or an absence of significant sex differences on measures of verbal IQ
(51,
54) and language
(49,
54). However, in a number of these latter studies, adjustments were made for age at illness onset, which may have attenuated potential sex effects, given that age of onset is known to be earlier in male patients than in female patients
(55). That is, accounting for sex effects in age at onset may have also accounted for sex effects in cognition. Moreover, the disproportionate representation of chronically disabled patients in some samples may have attenuated sex effects, given that these samples would include more severely ill women with cognitive impairments
(46,
56).
We previously demonstrated sex differences in a global construct of verbal functioning among adult schizophrenia patients that parallel findings in studies of healthy individuals in which female subjects outperformed male subjects
(46). The current study is novel in that we explore the possibility that schizophrenia involves problems in “lower-level” language processes, such as phonology, that may be differentially influenced by sex. Moreover, we are unaware of any studies that systematically examined 1) which specific components of language are most vulnerable in schizophrenia from a psycholinguistic viewpoint; 2) to what extent these components may be differentially influenced by sex; and 3) whether the pattern holds when patients are compared to healthy same-sex subjects, with adjustment for potential confounding cognitive factors. Our assumption is that identifying sex differences in specific language domains would have implications for understanding sex differences in brain abnormalities in language-associated regions. We sought to clarify these questions by examining the individual language domains of phonology, semantics, and grammar. We selected these domains because they are most closely linked with the language-associated brain regions for which normal volumetric sex differences have been identified (e.g., the planum temporale, superior temporal gyrus, Heschl’s gyrus, Broca’s area [
27–
29]) and in which disruptions in normal sexual brain dimorphisms in schizophrenia have been demonstrated (e.g., references
9,
15,
45).
Phonology and semantics were of particular interest in the light of mounting evidence that while semantics (e.g., semantic fluency) and phonology (e.g., phonemic fluency) are both disrupted in schizophrenia, semantics are affected more so (for a quantitative review, see reference
57)
(58,
59). This finding likely reflects the dual disruption in schizophrenia of frontal and temporoparietal functions associated with verbal fluency and is noteworthy given that a reverse pattern is typical in healthy comparison subjects. One implication is that although higher-order frontal/executive functions—namely activation/retrieval and organization/planning (which affect semantic and phonemic fluency)—play a role in language more generally and disruptions in these functions may contribute to thought disorder and disorganized speech in schizophrenia, concurrent problems arise at the lower level of semantic processing (see reference
60). We began to address this problem by investigating whether there are differential deficits by sex at the more basic levels of processing, such as phonology and grammar, compared with semantic processing. This cognitive study is the first step toward better understanding how sex differences in language dysfunction may be linked with disruptions in normal sexual brain dimorphisms in schizophrenia.
Method
Subjects
The patients were systematically ascertained from an extensive outpatient treatment system in Boston, which ensured clinical stability upon participation. The patients included 31 (17 male and 14 female) individuals who met the DSM-III-R diagnostic criteria for schizophrenia. The healthy comparison subjects (N=27; 13 male and 14 female subjects) were ascertained from the same catchment area through advertisements and bulletin board postings in local hospitals.
The comparison and overall patient groups did not significantly differ on age (patients: mean=39.1 years, SD=7.0), ethnicity (85% non-Hispanic white), education level (1 year of college), socioeconomic background (middle class), or Wide-Range Achievement Test, Revised reading subtest (WRAT-R)
(61) score (mean=102, SD=10). The estimated IQ (based on WAIS-R vocabulary and block design age-scaled scores
[62]) was significantly lower for male patients (mean=93, SD=13) than for female patients (mean=104, SD=14) and male comparison subjects (mean=113, SD=12). Cooperation and psychosis ratings
(63) for all patients (men and women) reflected clinical stability (mild to mild/moderate symptoms). The patients were receiving a mean daily neuroleptic dose of 520 mg (SD=428) in chlorpromazine equivalents; mean daily doses were comparable for men and women. Subjects were proportionately comparable between groups within sex on age, handedness, parental socioeconomic status, and ethnicity. A more detailed description of, and data for, demographic and clinical characteristics stratified by sex is provided elsewhere
(46).
Written informed consent was obtained from all subjects after a full explanation of the study procedures. The study was approved by Human Studies Committees at Harvard Medical School and Massachusetts Mental Health Center.
Diagnostic Assessment
Consensus diagnoses, based on DSM-III-R diagnostic criteria, were made by experienced diagnosticians (J.M.G. and L.J.S.) who were unaware of the patients’ neuropsychological data. The diagnosticians reviewed information obtained from structured research interviews with the Schedule for Affective Disorders and Schizophrenia
(64) and from systematic record reviews. The healthy comparison subjects received a brief clinical interview and were administered the MMPI-168 to screen for current psychopathological disorders; they were included if the T score was less than or equal to 70
(65).
Neuropsychological Assessment
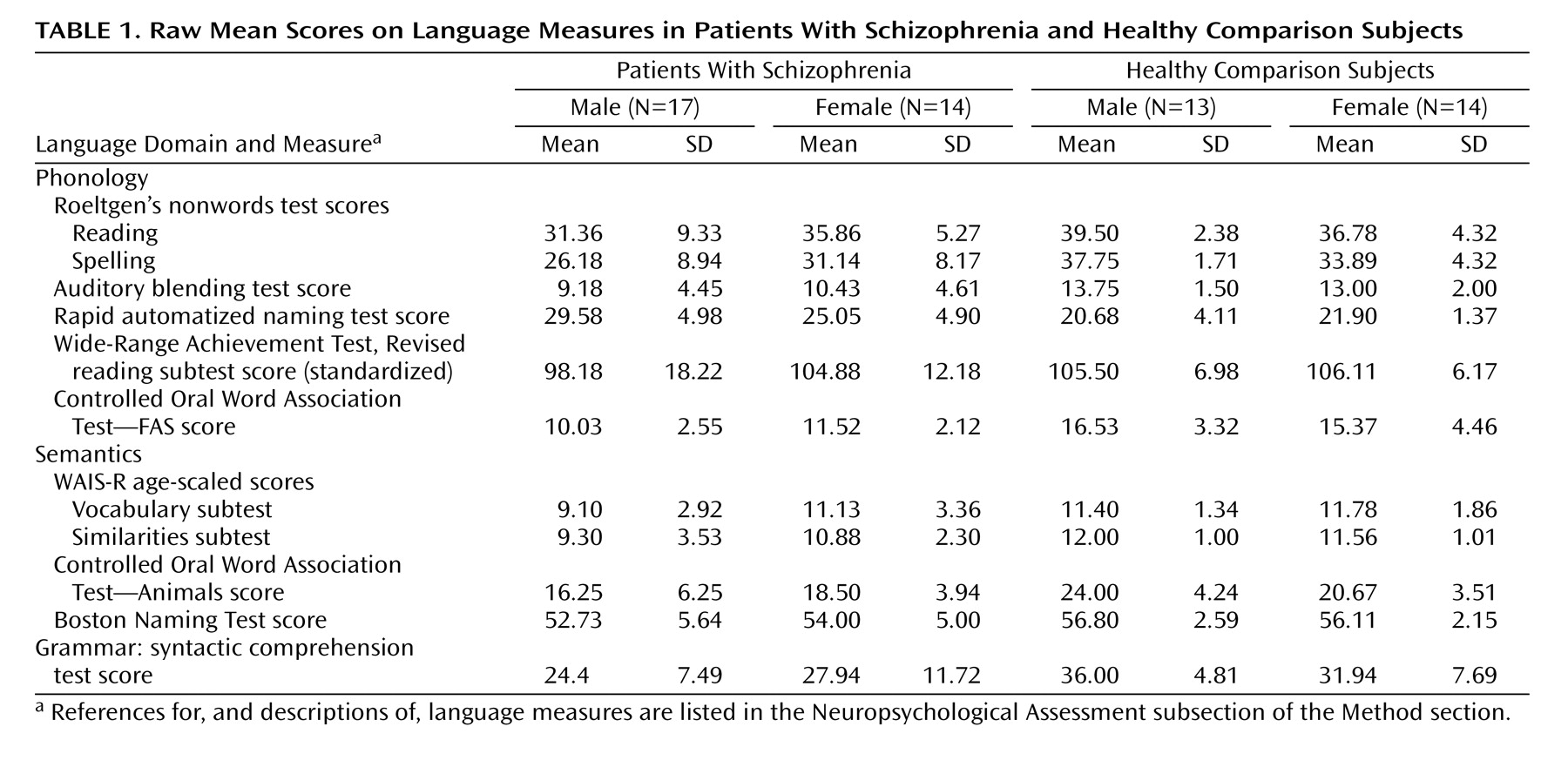
An extensive language battery, including tests of phonology, semantics, and grammar (
Table 1), was administered in the context of a comprehensive neuropsychological battery (see reference
46). The phonology composite measure included 1) Roeltgen’s Nonwords Reading Test
(66), total correct (read aloud a list of nonwords); 2) Roeltgen’s Nonwords Spelling Test, total correct (write down the proper spelling of a list of nonwords read to the subject one at a time); 3) auditory blending test, total correct (decipher words read to the subject in a broken form, e.g., “re…cor…der” = recorder); 4) rapid automatized naming test
(67), total time (name the letters, numbers, colors, or pictures presented on cards); 5) WRAT-R
(61), standardized score (single word reading); and 6) Controlled Oral Word Association Test—FAS
(68), total correct (generate as many words as possible that begin with a designated letter [F, A, or S] within a 60-second time period). The semantics composite measure included 1) WAIS-R Vocabulary subtest
(69), age-scaled score (provide definitions of vocabulary words); 2) WAIS-R Similarities subtest
(69), age-scaled score (deduce how two words are alike/the same); 3) Boston Naming Test
(70), total correct spontaneous responses (confrontation naming of 60 objects illustrated in line drawings); and 4) Controlled Oral Word Association Test—Animals
(68), total correct (generate as many words as possible that are names of animals within a 60-second time period). Use of age-scaled scores for the WAIS-R subtests is standard in the literature. The grammar index consisted of the syntactic comprehension test from the 20-minute short form of Caplan and Hildebrandt’s task
(71), total correct (identify the subject and object of the actions on the basis of various placement of prepositional phrases). Examiners had extensive experience in clinical assessment and neuropsychological testing with schizophrenia patients. Although the examiners were not blind to the patients’ status, they did not conduct the diagnostic interviews. The internal consistency reliability measures (Cronbach alpha for standardized variables) associated with the language measures composing the phonology (α=0.72) and semantics (α=0.81) domains were excellent. Language domains were created by standardizing all of the variables to a mean of 0 and standard deviation of 1 and averaging these standardized scores within each function. The grammar index was similarly standardized in order to use it in analyses of specificity with the other domains.
Clinical Description of the Language Assessments
The following patient description illustrates typical language dysfunctions related to our three domains of interest. A 31-year-old male patient with DSM-III-R chronic schizophrenia of 10 years’ duration was disorganized and delusional and had psychomotor symptoms at the time of assessment. He had 11 years of education and a current IQ of 92, average for a person with schizophrenia. His current IQ was higher than his ability on semantic processing tasks such as naming visual objects (Boston Naming Test) and defining words orally (WAIS-R vocabulary subtest). His performance on relatively basic tasks tapping into phonological processing and automatic knowledge, including a single-word oral reading test (WRAT-R reading subtest), was also impaired, even though performance on this test is typically preserved in schizophrenia and often better than performance on comparably normed IQ tests. This finding suggested that he had some premorbid developmental language impairment. In addition, he had gross difficulty in generating words on a verbal fluency test (Controlled Oral Word Association Test—FAS), producing approximately five words and then quitting after he perseverated on the last one. This latter performance was likely associated with a disorder of cognitive control and prefrontal/executive impairments superimposed on preexisting deficiencies. Regarding sentence comprehension, he (as well as a number of other patients) was able to correctly identify subjects and objects receiving actions in simple sentences. However, he and other patients had difficulty identifying subjects and objects of actions in complex sentences, such as “The boy that the old man pinched caught his friend.” This pattern reflects a common difficulty in abstract conceptual and sequential thinking in patients with schizophrenia. In summary, typical of many male patients in our sample, this patient’s expression of semantic knowledge, grammar, and phonological fluency were all impaired beyond what would be predicted from his IQ. These impairments became more pronounced when the patient had to search his own lexicon and initiate and sustain responses (such as on verbal fluency tests) or utilize abstract reasoning and interpret linguistic relationships. The pattern of performance suggests a combination of premorbid developmental language impairment and current dysfunction in executive control consistent with the relatively more severe linguistic impairments observed in the men with schizophrenia.
Data Analyses
A multivariate general linear model for correlated data
(72) was used to test for significant sex differences across language functions, with the independent predictors of sex, group, and sex-by-group interaction. Investigators have implicated a role of executive functions specifically in language dysfunction in schizophrenia
(38). We therefore covaried for attention (a core cognitive function that affects language processing independent of group effects) to control for the degree to which variability in this aspect of cognition contributes to language deficits and/or sex effects. The objective was to clarify whether sex differences in language problems in schizophrenia persist above and beyond underlying disruptions in complex attention/executive functions. We selected from our previous work the attention measure that captures a wide range of complex attention/executive functions. Attention was operationalized as a composite measure
(46) of the auditory continuous performance test (total correct), visual continuous performance test (discriminability and reaction time scores), dichotic listening test (total correct digits), WAIS-R digit symbol subtest (total), and visual cancellations test (total time and errors). The interaction term was used to test whether there was a “different difference” between women and men with schizophrenia, compared with their healthy counterparts. In addition, our stringent sampling procedures controlled for much extraneous variation, which is important when identifying significant sex effects in small samples.
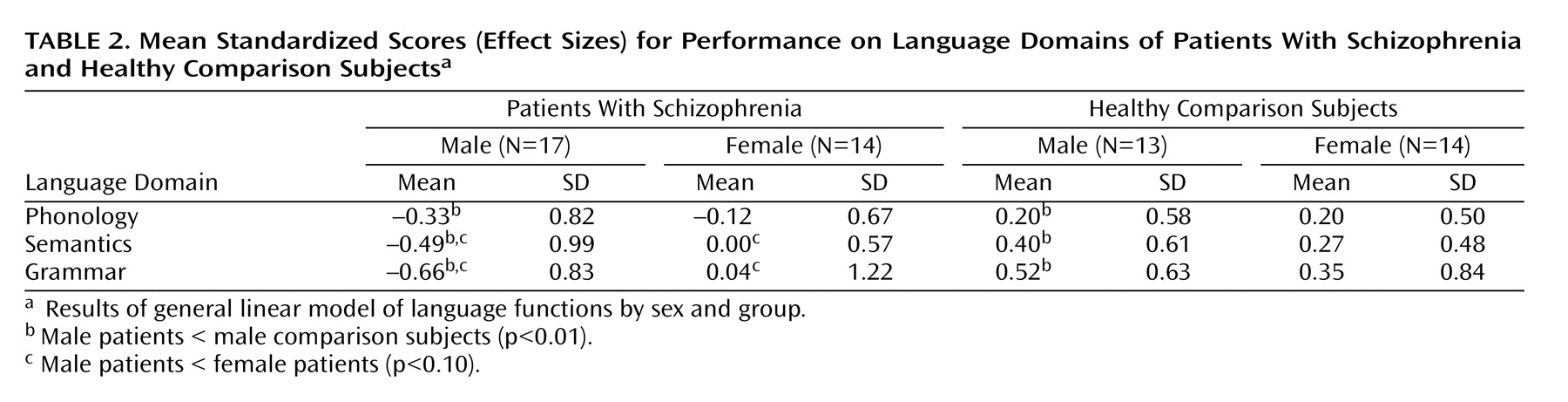
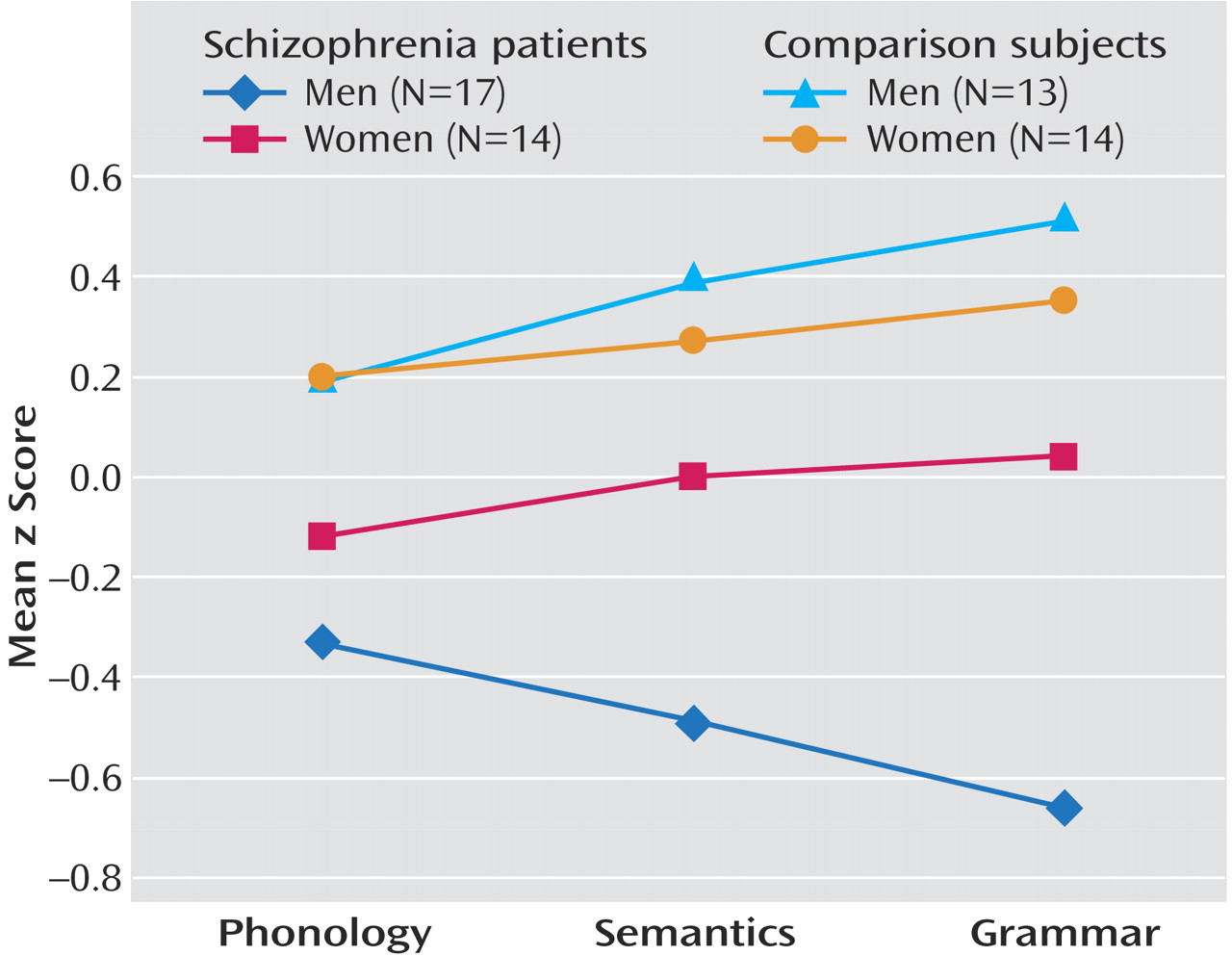
Table 1 presents raw mean scores for the individual measures that composed the language domains. The variables were standardized by using the standard deviations from the total sample, reflecting differences from general population averages. The mean standardized scores depicted in
Figure 1 reflect effect sizes within each group.
Results
The results of the multivariate general linear model for correlated data showed a significant group effect on subjects’ performance in the three language domains with adjustment for attention (F=2.92, df=3, 81, p<0.04). The univariate general linear models showed that the interaction of sex by group was significant for semantics (t=1.94, df=98, p=0.05) and grammar (t=2.09, df=89, p<0.04) and for phonology with adjustment for attention (t=2.31, df=97, p=0.02) (
Table 2). The univariate analyses showed that male patients performed significantly worse than their healthy male counterparts on all three domains, whereas female patients, compared to their healthy counterparts, had substantially smaller and nonsignificant functional reductions across all domains (
Figure 1). Further, between the sexes, male patients performed worse than female patients on grammar (t=–1.77, df=25, p<0.09) and semantics (t=–1.72, df=26.2, p<0.10). Although these differences did not reach statistical significance, male patients’ performance on these domains was approximately one-half of a standard deviation below that for female patients. Male and female patients performed more similarly on phonological processing.
Women with schizophrenia performed relatively worse on phonological processing than on semantics or grammar (effect size=–0.12 for phonology versus 0.00 and 0.04 for semantics and grammar, respectively). In contrast, men with schizophrenia were the least affected on phonology (effect size=–0.33 for phonology versus –0.49 and –0.66 for semantics and grammar, respectively). Across domains, the effect sizes for the male patients, compared with the healthy male comparison subjects, had a twofold difference, whereas the differences in effect sizes for the women were less.
Discussion
This study demonstrated significant sex differences in language domains in comparisons between healthy men and women and men and women with schizophrenia. Women with schizophrenia, compared to their healthy counterparts, had relative preservation of function across domains. Phonological processing performance in women with schizophrenia was below that in healthy female subjects and was not significantly different from that in men with schizophrenia. However, grammar and semantics were sexually differentiated. Men with schizophrenia, compared to healthy men, showed impairment across the three language domains. The finding of relatively worse performance across language domains in the male patients, relative to the healthy comparison subjects, was consistent with previous findings of impaired verbal functions among patients with schizophrenia, including findings from our earlier work
(46).
In the comparison of male patients with female patients, the relatively worse performance across all language domains among male patients was consistent with previous research demonstrating more impaired verbal learning and verbal fluency
(47,
73) among male patients, compared to female patients. The results from the current study extended our previous findings
(46) by demonstrating that although there was relative preservation of functioning among the women, there were some differences among individual language components (
Figure 1). Specifically, male patients (relative to their healthy counterparts) were more substantially affected in semantics and grammar, with a relatively smaller decline observed in phonology. A reverse pattern was observed among female patients (relative to their healthy counterparts). The direction of the findings (albeit not significant) suggested a relative preservation of grammar, which was the least affected domain (nonsignificantly less than semantics), whereas phonology was the most substantially affected domain (falling below the female population average).
One of the limitations of this study was the relatively small sample size. Previous literature showed a relative advantage for normal women compared with men regarding phonological processing, although in our sample normal men and women were comparable. This was most likely attributable to limited power due to small sample size, particularly given that there is greater variability within than between the sexes in the normal population. The present study, however, focused on how male and female patients
differed from their healthy counterparts on language domains. In fact, sample sizes within sex were similar, and there were significant differential sex effects. This may in part be due to the fact that the samples were tightly comparable within sex on important sociodemographic and other potential confounders that may affect language function. There were no significant sex differences in chlorpromazine equivalents or other clinical factors
(46). Moreover, because the study was designed to measure particular domains of language, the psychometric properties of these domains were strong.
Overall, the current findings suggested a divergent pattern of sex differences, namely a more pronounced “decline” in anterior (e.g., phonology) and posterior (e.g., semantics) language functions in male than in female patients (in comparisons of patients with their healthy counterparts). This finding was strikingly consistent with research implicating sex differences in
structural brain volumes in comparisons of normal sexual dimorphisms to patients’ sexual dimorphisms in regions associated with language functions, such as Heschl’s gyrus, planum temporale, Broca’s area, and superior temporal gyrus
(9,
12,
15,
27,
45,
74,
75). For example, in an earlier study, sex differences in planum temporale asymmetry were found, with male patients demonstrating exaggerated leftward planum temporale asymmetry, compared with healthy male subjects, and female patients demonstrating more right asymmetry, compared with healthy female subjects
(45). The current findings are also consistent with recent functional neuroimaging studies demonstrating relatively greater right hemisphere
(30,
31) or more symmetrical
(76) involvement in phonological processing in healthy women than in men, although not consistently (e.g., references
77,
78), and reduced lateralization of phonological processing in male patients relative to healthy comparison subjects
(79,
80) and female patients
(81), again although not consistently
(82).
It is possible that phonology—an aspect of language that ordinarily tends to be more left-lateralized functionally and more reliant on anterior functions (e.g., frontal/executive control) than aspects of language that are more evenly distributed across hemispheres (e.g., semantics) and believed to be reliant on both anterior (frontal
and posterior (temporal) language regions—is less affected in male patients, given the association with increased left asymmetry in planum temporale in male patients
(45). In contrast, findings in female patients, who as females are expected to show greater frontal and temporal symmetry and have shown greater asymmetry with increases in the right planum temporale
(45), suggest the potential for enhanced ability to recruit right hemisphere posterior regions for semantic task performance.