As methods for high-resolution MRI continue to develop, our understanding of changes in brain structure in patients with psychiatric disorders improves. In patients with schizophrenia, decreases in the gray matter volume of a variety of cortical and subcortical brain regions have been repeatedly observed
(1) . Two articles in this issue of the
Journal add to this literature and go further by strengthening the hypothesis that schizophrenia involves abnormalities in specific cortical-subcortical networks. Ellison-Wright et al.
(2) present a meta-analysis of MRI studies that reveals different patterns of structural changes in first-episode and chronic schizophrenia. Adapting a technique developed to combine data from functional MRI studies
(3), the authors evaluated group differences in specific brain regions in reference to a three-dimensional coordinate system. The result of this adaptation, called anatomical likelihood estimation, adds to a growing literature on probabilistic approaches to neuroanatomical computation
(4) . In patients with first-episode schizophrenia, Ellison-Wright et al. found evidence for decreased gray matter volume in the hippocampus, the caudate nucleus, the thalamus (mediodorsal nucleus), the insula, the anterior cingulate gyrus, the inferior frontal gyrus, and the cerebellum. Subcortical changes were similar in patients with chronic schizophrenia, but cortical changes were even more extensive.
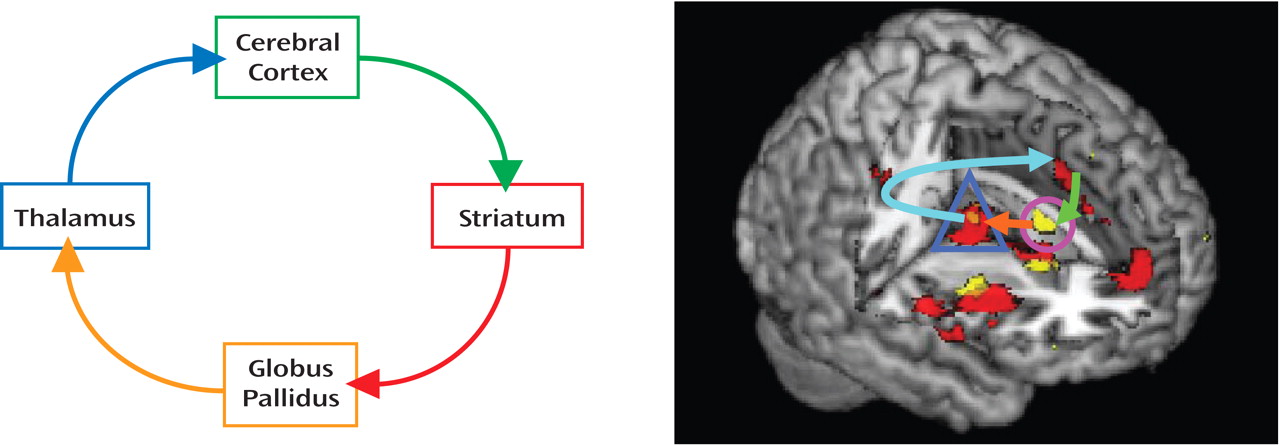
As Ellison-Wright et al. note, this pattern of abnormality implicates a neural circuit originating with limbic input to the striatum, then the thalamus, and finally to the prefrontal and cingulate cortex (
Figure 1 ). Abnormalities of thalamocortical circuitry have previously been implicated in schizophrenia, particularly in reference to the pathophysiological concept of cognitive dysmetria
(5) .
Also in this issue, Friedman et al.
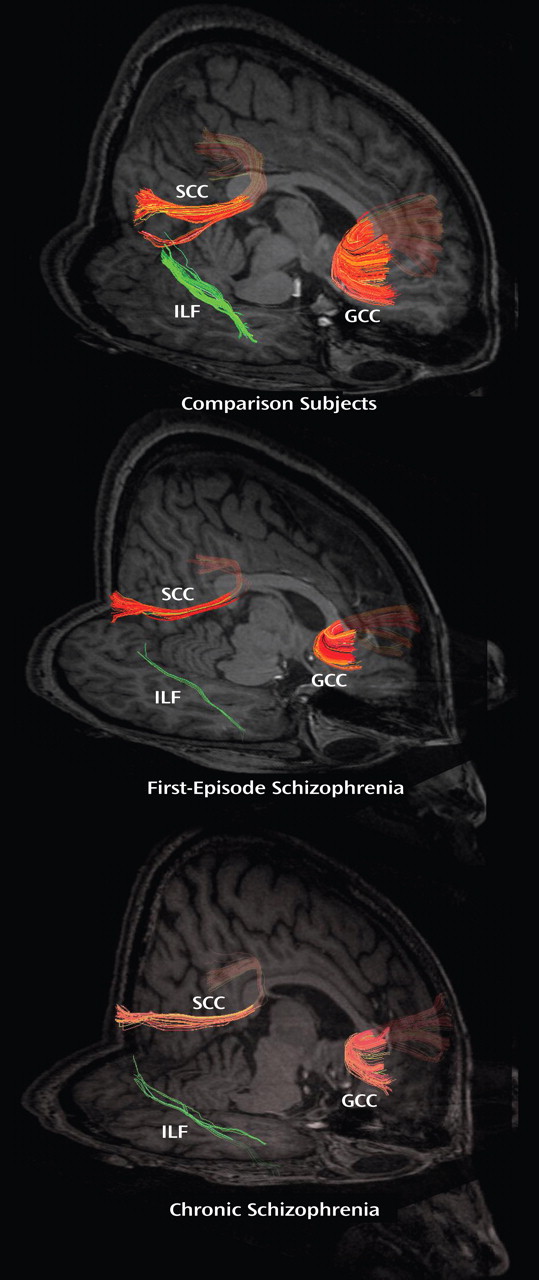
(6) report on their use of diffusion tensor imaging to examine the pattern of white matter changes in patients with first-episode and chronic schizophrenia. Using fractional anisotropy (FA) to assess the integrity of white matter connections
(7), they found evidence in first-episode patients for decreased connectivity only in the inferior longitudinal fasciculus (at the trend level), while chronic patients showed a broader pattern of white matter disturbances (
Figure 2 ).
The results of Friedman’s study, to date the largest to directly examine FA in first-episode and chronic schizophrenia patients, suggest a number of intriguing interpretations. As they note, one explanation may be that pathological white matter abnormalities may be present but too subtle to detect with current imaging methods in first-episode schizophrenia. Alternatively, white matter changes may develop as the disease process of schizophrenia progresses.
Taken together, the results of these two studies provide strong support for the hypothesis that schizophrenia involves abnormalities in networks of brain regions. They further suggest that such abnormalities may be progressive in at least some patients. If the “progression” hypothesis is confirmed in future studies, we must redouble our efforts at early and effective intervention for this potentially disabling disorder.