Suicide Attempt as the Presenting Symptom of C9orf72 Dementia
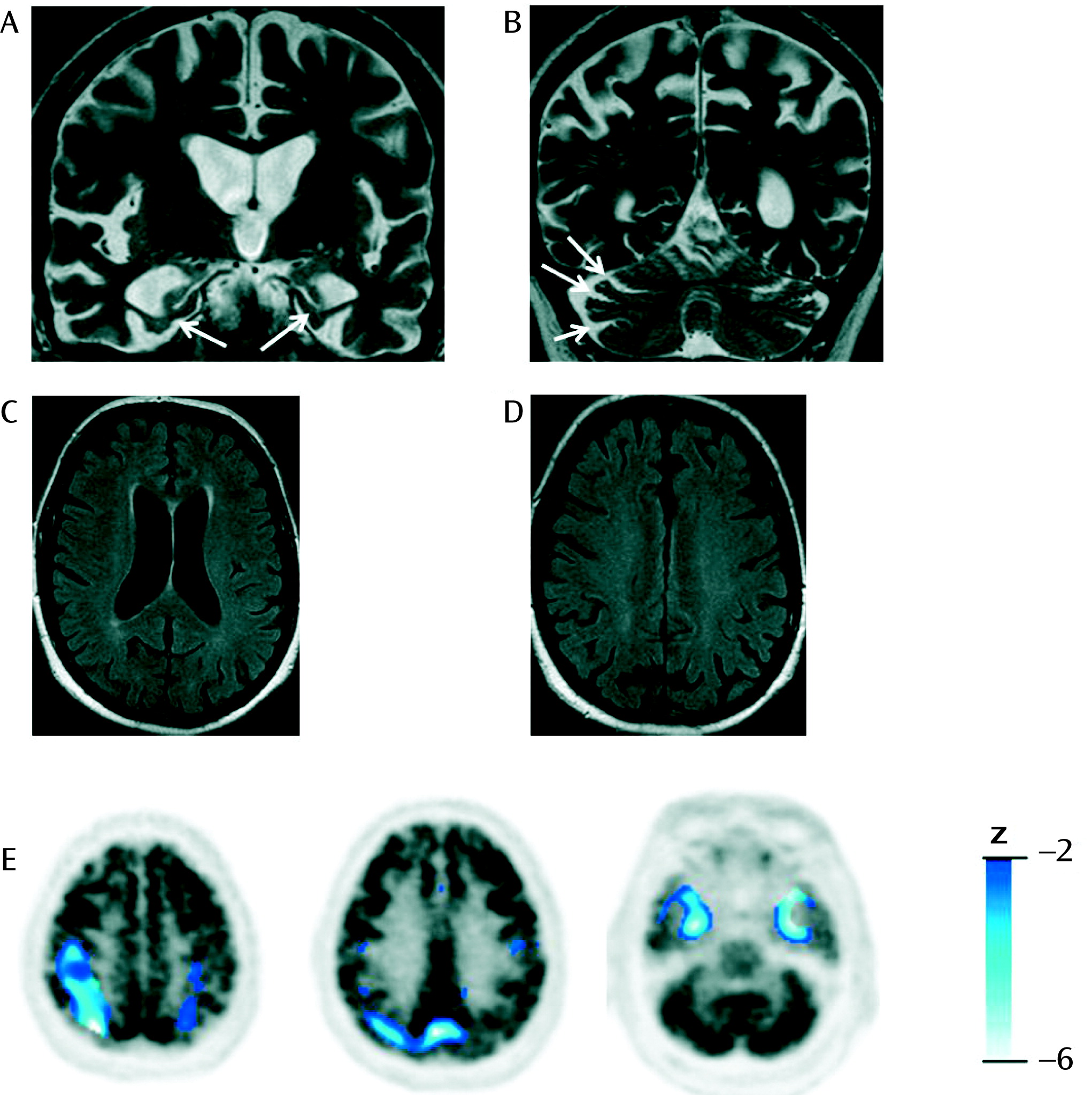
A 72-year-old German man without significant previous medical or psychiatric illnesses was admitted after trying to hang himself. An adjustment disorder was assumed at first, but psychiatric examination revealed a striking lack of concern about the suicide attempt, frequent irrelevant answers, and inappropriate jocularity without any signs of depression. His wife reported a 2-year history of subtle behavioral disinhibition (short episodes of socially inappropriate behavior and impulsive reactions) and deficits in short-term memory and face recognition in her husband, but history and observation did not reveal additional symptoms necessary for a diagnosis of possible behavioral frontotemporal dementia (5). (For details of the diagnostic workup, see the data supplement that accompanies the online edition of this letter.) Neuropsychological testing results revealed mild deficits in the domains of verbal episodic memory and visuospatial abilities but not in executive functions such as strategic thinking and executive flexibility (see the online data supplement). MRI and [18F]fluorodeoxyglucose positron emission tomography (FDG-PET) revealed several abnormalities, including temporal atrophy with hippocampal degeneration and biparietal and temporomesial hypometabolism, but no frontal atrophy or hypometabolism (Figure 1). Although behavioral frontotemporal dementia can present with anterior temporal atrophy without frontal atrophy or hypometabolism (5), this imaging pattern was considered to be atypical for behavioral frontotemporal dementia or, at least, to be unspecific. The patient’s sister died by suicide at age 50, and his mother began to show late-onset progressive nonfluent aphasia at age 85. Based on this family history, C9orf72 genotyping was initiated, revealing a pathogenic expansion of more than 50 repeats (2, 3). A written informed consent was obtained from the patient after the procedures and the publication had been fully explained to him and his family.
Acknowledgments
References
Information & Authors
Information
Published In


History
Authors
Competing Interests
Metrics & Citations
Metrics
Citations
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
View Options
View options
PDF/EPUB
View PDF/EPUBLogin options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
Personal login Institutional Login Open Athens loginNot a subscriber?
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).