Several independent studies (
1–
4) have provided data suggesting that a clinically significant form of depression can arise as early as age 3. The identification of the earliest developmental manifestations of depression is critical to targeting interventions before a chronic and relapsing illness trajectory is established. Preschool-onset depression, a form of depression observed in children between the ages of 3 and 6, is characterized by age-adjusted manifestations of the core DSM symptoms of major depressive disorder (e.g., neurovegetative signs, anhedonia, and guilt) known in older children and adults. Preschool depression has been shown to have content and discriminant validity, homotypic continuity over 18–24 months, higher rates of familial affective disorders compared with healthy subjects, and biological correlates (
2,
5,
6). These features are markers of validation for psychiatric disorders according to criteria originally outlined by Robins and Guze (
7). The validity of preschool depression has been established across multiple independent study samples, providing support for the public health importance of this construct (see Table S1 in the
data supplement that accompanies the online edition of this article). More recently, alterations in brain function and structure similar to those observed in depressed adults have been detected at school age in children who experienced an episode of preschool-onset depression as well as in depressed preschoolers themselves (
8–
11). Given these findings, the importance of early identification and intervention is enhanced by the potential to interrupt the disease trajectory during a period of greater neural plasticity.
Based on estimates of prevalence and reports of referral in clinical settings, depression in preschool children appears to be a clinically underrecognized disorder (
4,
12,
13). As preschool depression is not inherently disruptive, and preschoolers are less likely than older children to spontaneously report their internalized distress, these early-onset depressive symptoms often go undetected by caregivers. However, findings that depressed preschoolers were significantly impaired across contexts and activities when rated by teachers and parents support its clinical significance (
2). Sadness and irritability are common but nonspecific clinical symptoms of preschool depression. More specific markers that are useful in distinguishing preschool depression from other preschool disorders include increased expression of and preoccupation with guilt; changes in sleep, appetite, and activity level; and decreased pleasure in activities and play. The latter is not normative during the preschool period, when joyful play exploration is a central developmental theme (
2), and thus a lack of joyfulness may be more apparent than overt sadness in the preschool child. Persistent preoccupation with negative play themes may also be a tangible clinical sign. Because depressed preschoolers rarely appear persistently withdrawn, sad, or vegetative and do not appear to exhibit sustained depressive symptoms for a 2-week period, but instead show periods of age-appropriate brightening, it is important to look for circumscribed yet recurrent manifestations of these symptoms over time.
Preschool depression is characterized by subthreshold DSM criteria for major depressive disorder (14). As noted above, when identifying preschool depression, the 2-week duration criterion is not strictly enforced, and preschoolers who meet at least four (rather than the required five) symptoms for a major depressive episode have been included in this clinical group based on markers of validation (
6,
14,
15). The fact that depressed preschoolers have failed to meet full DSM criteria for major depression has raised questions about the clinical and public health significance of preschool depression, with some suggesting that it represents a risk state or a “minor” depression. Alternatively, others have argued that there may be developmental differences in the temporal manifestations of affective disorders in early childhood and that adjustments to clinical criteria for some axis I disorders may be indicated. An example of this is the criteria for early-childhood posttraumatic stress disorder (PTSD) in DSM-5, allowing for the use of developmentally modified symptom manifestations as well as requiring fewer symptoms to qualify for the disorder. Whether this is scientifically justified in depression remains an issue of debate, leaving the precise public health and clinical significance of preschool depression unresolved.
In an attempt to further clarify the public health significance of preschool depression, we investigated the risk of meeting full DSM-5 criteria for major depressive disorder at school age and in early adolescence in a longitudinal sample of depressed preschool children as well as healthy and psychiatric comparison subjects. Longitudinal outcomes of childhood disorders have been an important element of establishing diagnostic validity, and this criterion was prioritized in decision making for modifications to childhood disorders in DSM-5. Notably, both heterotypic and homotypic longitudinal outcomes of school-age and adolescent depression have been reported in several key study samples (
16,
17). Therefore, whether preschool depression was also a risk factor for other axis I disorders at school age and in early adolescence was also explored.
Also of interest was whether psychosocial factors could be identified that predict which preschoolers were at greater risk for later diagnosis of major depressive disorder. We hypothesized that specific environmental/familial conditions, including maternal history of depression, nonsupportive parenting, and traumatic or stressful life events, would be predictors of later meeting full criteria. Of additional interest was what other preschool-onset axis I disorders increased the risk for major depression at school age and in early adolescence, and particularly whether a preschool-onset anxiety disorder would be a predictor of later major depression, as has been demonstrated by studies in older children (
18).
Based on the notion that preschool-onset depression is an early manifestation of the well-validated later childhood disorder, we hypothesized that preschool depression would exceed other axis I preschool disorders and salient risk factors as a robust risk factor for meeting full criteria for major depressive disorder at school age and in early adolescence. Given the clear importance of income-to-needs ratio and negative parenting as risk factors for a variety of poor developmental outcomes and maternal history of depression as a risk factor for childhood depression (
19–
21), these variables were of particular interest. If clear predictors of the later full disorder could be identified, they could be used to determine which preschoolers should be targeted for early intervention.
Method
Study Population
Preschoolers between the ages of 3 years and 5 years 11 months were recruited from primary care and day care sites in St. Louis and screened with the Preschool Feelings Checklist, a validated screening measure for identifying children at high risk for preschool-onset depression (
22,
23). Children with symptoms of depression were oversampled, and children with symptoms of other psychiatric disorders and healthy children were included as comparison groups. Details of the study’s recruitment methods and participant flow have been described previously (
24; see also the flow diagram in Figure S1 in the online
data supplement). Study subjects and their primary caregivers participated in up to six comprehensive annual (and up to four semiannual) assessments conducted at the Early Emotional Development Program at the Washington University School of Medicine (mean, minimum, and maximum numbers of assessments are summarized in Table S2 in the
data supplement). After receiving a complete description of the study, parents provided written informed consent and children provided assent. All study procedures were approved by the Washington University School of Medicine institutional review board.
Measures
Child psychopathology and stressful and traumatic life events.
Assessments included a comprehensive age-appropriate diagnostic interview that assessed for the presence of DSM axis I psychiatric disorders as well as stressful and traumatic life events at each study wave. When children were between the ages of 3 years and 7 years 11 months, the Preschool Age Psychiatric Assessment (PAPA) was administered to caregivers (
25). When children were age 8.0 years or older, both child and caregiver reports of psychiatric symptoms were collected using the Child and Adolescent Psychiatric Assessment (CAPA, the interview from which the PAPA was adapted) (
26,
27). The PAPA and CAPA include all relevant DSM criteria and their age-appropriate manifestations and have been shown to have test-retest reliability (
26,
28) as well as reliability for the assessment of stressful/traumatic life events (
29). Parent and child report on the CAPA were combined by taking the most severe rating, as is standard in child depression research. Raters trained to reliability and blind to the child’s diagnostic status from prior waves administered the PAPA or CAPA at each assessment point. Blind ratings could be achieved because of the large study sample and assessments over a 10-year period, allowing the use of different interviewers to rate participants at each wave. In addition, the diagnosis is derived through a computer-based DSM algorithm, using all endorsed symptoms, making diagnostic determinations more objective. High test-retest reliability for the major depressive disorder module on the PAPA (for diagnosis, kappa=0.62, and mean symptom endorsement intraclass correlation coefficient=0.88) and high interrater reliability (kappa=0.79, intraclass correlation coefficient=0.97) have been established in our laboratory (
9,
30). All interviews were audiotaped, and methods to maintain reliability and prevent drift, which included ongoing calibration of interviews by master raters for 20% of each interviewer’s cases, were implemented in consultation with an experienced clinician (J.L.L.) at each study wave.
The PAPA/CAPA assesses 18 stressful life events (e.g., change in day care/school) and 21 traumatic life events (e.g., death of a loved one). The frequencies of all types of stressful and traumatic life events were summed to create an overall stressful life event frequency and an overall traumatic life event frequency.
Income-to-needs ratio.
The income-to-needs ratio was computed as the total family income at baseline divided by the federal poverty level, based on family size, at the time of data collection (
31).
Pubertal status.
Pubertal status was rated at each study wave for children age 10 and older using the Pubertal Status Questionnaire, a validated self-report measure of pubertal development (
32).
Maternal history of depression.
The Family Interview for Genetic Studies (
33) was used to obtain family history of depression and other affective disorders in first- and second-degree relatives. At each wave of data collection, primary caregivers (93% of them mothers) were interviewed about family history of psychiatric disorders, and the screening checklist for major depression was given when screening items were endorsed. Therefore, data on maternal history of depression were based on mothers’ self-report using the Family Interview for Genetic Studies major depression screen or on history of clinician diagnosis in 93% of cases (7% were based on other caregiver report). The Family Interview for Genetic Studies is a fully structured instrument for which the senior investigator (J.L.L.) trained interviewers to reliability (
33). Questions about the diagnostic status of a family member were reviewed by a senior psychiatrist (J.L.L.) blind to the child’s diagnostic status. The Family Interview for Genetic Studies was administered to all participants and updated at each annual study wave.
Nonsupportive parenting.
At the first annual follow-up wave, children and parents were observed interacting during a mildly stressful task in which the child was required to wait for 8 minutes before opening an attractive gift sitting within arm’s reach. The interaction was coded for parents’ use of nonsupportive parenting strategies (e.g., threats about negative consequences). High interrater reliability (>0.83) of coders has been established in the study sample. This task, which is used for assessing parenting strategies, is well validated and has good psychometric properties (
34,
35).
Data Analysis
In the analyses that follow, dichotomous variables were used for the presence or absence of preschool-onset diagnoses. This approach was used to account for the effect of specific disorders independent of levels of comorbidity (common in childhood psychopathology). Specifically, children who met the previously validated criteria for depression (described above) before age 6 were considered to have preschool-onset depression. Similarly, those who met criteria before age 6 for attention deficit hyperactivity disorder (ADHD), oppositional defiant disorder, or conduct disorder were categorized into preschool-onset groups for these disorders. Children who had separation anxiety, generalized anxiety, or PTSD before age 6 were categorized into a broader preschool-onset anxiety group. Children’s school-age axis I diagnostic outcomes at 6–13 years of age were defined in the same fashion (see
Table 1 for details on preschool and school-age comorbidity). No exclusions were applied, so any child who met criteria for a given diagnosis was included in that group regardless of comorbidity. For school-age diagnoses, participants had to meet full DSM-5 criteria; thus, for example, participants classified as having depression at age 6 or older had to meet full criteria for a major depressive episode (i.e., five or more symptoms at a clinically impairing severity level lasting at least 2 weeks).
In the analyses that follow, continuous variables were centered by subtracting the mean, and dichotomous variables were centered by assigning values of −1 and 1 to the two outcomes.
Potential covariates.
Independent logistic regression analyses were conducted to determine whether children’s gender and age at baseline were significantly associated with the likelihood of being diagnosed with school-age depression. Variables significantly associated with school-age depression status were then included as covariates in the final analysis.
Preschool-onset psychiatric disorders predicting school-age depression diagnosis.
Using logistic regression analyses, we calculated the odds ratios for diagnosis of depression at school age based on the presence or absence of five possible preschool-onset psychiatric disorders. School-age depression (present or absent) was the dependent variable, and preschool-onset depression, conduct disorder, anxiety disorders, ADHD, and oppositional defiant disorder were entered simultaneously as dichotomous predictor variables. Although school-age depression was the outcome diagnosis of most interest, four additional logistic regression models were constructed for comparison purposes using school-age conduct disorder, anxiety disorders, ADHD, and oppositional defiant disorder as the outcome variables.
Environmental/familial predictors of school-age depression.
Five separate logistic regression analyses were conducted to test for main effects of environmental/familial risk factors on school-age depression as well as to test for interaction effects between environmental/familial variables and preschool-onset diagnoses in relation to school-age diagnoses. Interactions between preschool diagnosis and environmental/familial variables were explored to test for mediation or moderation effects that are known in risk trajectories. For each regression, the independent variables were the main effect of a single environmental/familial variable (income-to-needs ratio, maternal history of depression, traumatic life events, stressful life events, or observed nonsupportive parenting behaviors), the main effect of one or more preschool-onset psychiatric disorders that significantly predicted school-age depression in the preceding analyses, and the interaction term(s) between the environmental/familial variable and presence of a preschool-onset disorder. School-age depression was the outcome variable for each analysis.
Final cumulative model predicting school-age depression.
Based on findings from the previous analyses, we tested all significant predictors of school-age depression simultaneously using hierarchical logistic regression.
Nonsupportive parenting as a mediator of the relationship between preschool-onset diagnoses and school-age depression.
Nonsupportive parenting has been found to mediate the effects of preschool-onset psychiatric disorders on numerous behavioral and biological outcomes in this sample as well as in other independent samples (
19,
20). Thus, we conducted formal tests for nonsupport as a possible mediator of the significant association between preschool-onset psychiatric disorders and school-age depression. In keeping with a traditional approach to mediation and its definition, we proceeded with tests for mediation only if the preschool-onset disorder significantly predicted school-age depression and the same preschool-onset disorder significantly predicted nonsupport. When a preschool-onset diagnosis predicted school-age depression but did not significantly predict nonsupport (the mediator), mediation was not tested, as this would violate a fundamental tenet of mediation, making formal mediation analysis unreliable. Mediation analyses were conducted using the process macro for SAS (
36).
Analyses were conducted with SAS, version 9.2 (SAS Institute, Cary, N.C.) and SPSS, version 21 (IBM, Armonk, N.Y.).
Results
Of 306 children enrolled at baseline, 246 had complete data on the variables of interest and were included in the analyses. The children included in the analyses did not differ significantly in demographic characteristics from the 60 who were not, except that the mean level of parental education was higher in those included (χ
2=8.10, p=0.044). The demographic and clinical characteristics of the study sample are summarized in
Table 2. Of children with school-age depression, 82.3% were prepubertal at the time of onset. Of those without school-age depression, 43.5% were prepubertal at the time of the last completed assessment. The mean duration of follow-up was 6.44 years (SD=1.04).
Potential Covariates
Children’s baseline age, but not gender, predicted the likelihood of having school-age depression (odds ratio=1.88, 95% CI=1.31, 2.70, p<0.001). That is, the older children were at baseline, the more likely they were to be diagnosed with depression at school age. Thus, final analyses included children’s age but not gender as a covariate.
Preschool-Onset Psychiatric Disorders as Predictors of School-Age Depression
Children previously diagnosed with preschool-onset depression were more than 2.5 times as likely as those without preschool depression to be diagnosed with school-age depression (Table 3). The rate of school-age depression was 51.4% in the 74 children with preschool-onset depression and 23.8% in the 172 children without preschool-onset depression. Preschool-onset conduct disorder was the only other significant predictor of school-age depression (p=0.003). No other axis I preschool diagnosis significantly increased the likelihood of school-age depression.
Preschool-Onset Depression as a Predictor of Other School-Age Disorders
Table 3 outlines the relationships between preschool disorders and school-age disorders. Notably, children with preschool-onset depression were on average three times as likely as children without preschool depression to have school-age depression, school-age anxiety, and school-age ADHD. Also, children with preschool-onset depression or anxiety disorders were significantly more likely than children without these diagnoses to have a school-age anxiety disorder.
As our aim in this study was to identify risk factors for DSM-5 major depressive disorder in later childhood, the remaining analyses include only the two preschool-onset disorders found to significantly predict school-age depression (i.e., preschool-onset depression and preschool-onset conduct disorder).
Familial/Environmental Predictors of School-Age Depression
Income-to-needs ratio.
Children from families with lower income-to-needs ratios (measured at baseline when participants were preschool age) were significantly more likely to have school-age depression (odds ratio=1.35, 95% CI=1.07, 1.70, p=0.012). The interaction effects of income-to-needs ratio by preschool-onset depression and income-to-needs ratio by preschool-onset conduct disorder were nonsignificant in relation to school-age depression diagnosis.
Maternal history of depression.
Children with school-age depression were almost twice as likely to have a mother with a history of depression compared with those without school-age depression (odds ratio=1.88, 95% CI=1.09, 3.24, p=0.023). The interaction effects of maternal history of depression by preschool-onset depression and maternal history of depression by preschool-onset conduct disorder were nonsignificant in relation to school-age depression diagnosis.
Observed nonsupportive parenting strategies.
Children whose primary caregivers were observed using nonsupportive parenting strategies more frequently during the parent-child interaction task were significantly more likely to have school-age depression (odds ratio=1.08, 95% CI=1.01, 1.15, p=0.020). The interaction effects of nonsupportive parenting by preschool-onset depression and nonsupportive parenting by preschool-onset conduct disorder were nonsignificant in relation to school-age depression diagnosis.
Stressful and traumatic life events.
The frequency of stressful life events experienced by children was unrelated to school-age depression. Children’s experiences of traumatic life events approached statistical significance as a predictor of school-age depression (odds ratio=1.02, 95% CI=1.00, 1.05, p=0.090). The interaction effects of trauma by preschool-onset depression and of trauma by preschool-onset conduct disorder were nonsignificant in relation to school-age depression diagnosis. Because of its importance in the literature and in our own sample as a predictor of school-age depression, trauma was also included in the final model despite its falling short of statistical significance.
Examining Diagnostic and Environmental/Familial Predictors of School-Age Depression Simultaneously
As seen in
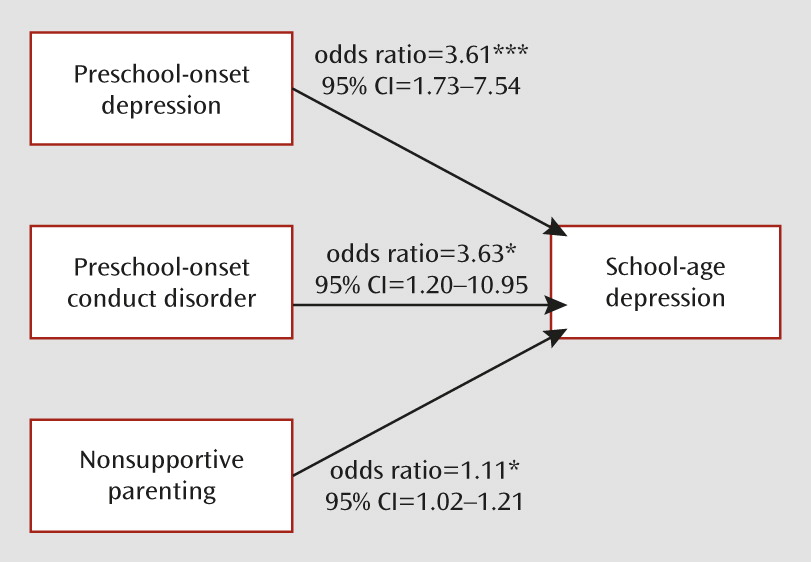
Table 4, step 1 of the analyses included children’s age at baseline and the significant environmental/familial variables. At step 2, the main effect of preschool-onset depression, preschool-onset conduct disorder, and the preschool-onset depression by preschool-onset conduct disorder interaction term were entered into the regression equation. Results indicated that when examined simultaneously in step 1 of the model, nonsupportive parenting and children’s age at baseline were the only significant environmental/familial predictors of school-age depression. That is, preschoolers with caregivers who used nonsupportive parenting strategies more frequently were significantly (p=0.019) more likely to have school-age depression. When preschool-onset depression and conduct disorder were included at step 2, children’s baseline age, nonsupportive parenting, preschool-onset conduct disorder, and preschool-onset depression were all significant predictors of school-age depression (
Figure 1).
Associations Between Preschool-Onset Conduct Disorder and School-Age Depression: Nonsupportive Parenting as a Mediator
Before conducting formal tests of nonsupportive parenting as a mediator of the relationship between preschool-onset depression or conduct disorder and school-age depression, mean scores of nonsupport in four diagnostic groups (preschool depression and conduct disorder; preschool depression only; preschool conduct disorder only; and neither preschool depression nor conduct disorder) were calculated. As shown in
Table 5, in a general linear model with pairwise group contrasts, nonsupportive parenting was significantly greater in the preschool conduct disorder only group compared with the other three diagnostic groups (preschool depression and conduct disorder: F=11.73, p<0.001; preschool depression only: F=35.21, p<0.001; neither preschool depression nor conduct disorder: F=24.41, p<0.001). Based on this result, a formal test of mediation was conducted for the relationship between preschool conduct disorder and school-age depression (mediation was not tested for preschool depression because it was not significantly associated with nonsupport).
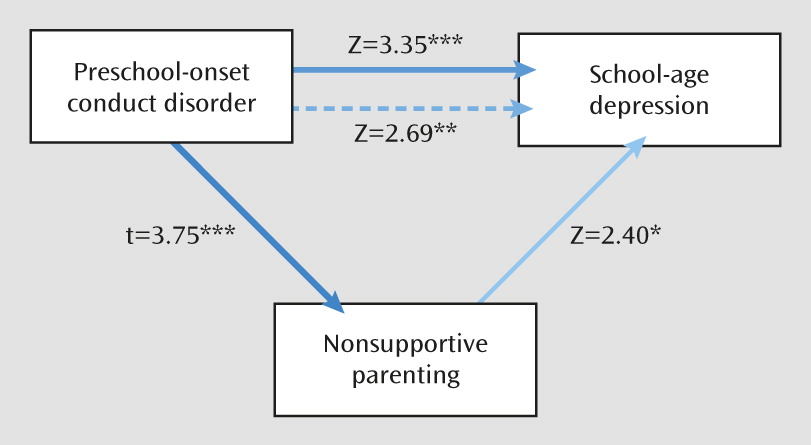
The effect of preschool conduct disorder on school-age depression was partially mediated through nonsupportive parenting (95% bootstrap CI=0.019, 0.364). The effect of preschool conduct disorder on school-age depression was reduced by 21% when nonsupport was accounted for in the model (
Figure 2).
Discussion
The study findings demonstrate that preschool depression was a significant and robust predictor of meeting full DSM-5 criteria for major depressive disorder in later childhood and early adolescence (i.e., at ages 6–13). The predictive power of preschool depression for school-age depression remained strong and undiminished even when other key environmental and familial risk factors were included in the model. Preschool conduct disorder also remained significant, although its effect was diminished when nonsupportive parenting was accounted for. This finding extends the available data by demonstrating that preschool depression not only shows homotypic continuity up to 2 years later but also converts to meet all formal DSM-5 criteria for major depressive disorder during school age and early adolescence (a mean of 6 years later). This finding of major depressive disorder as a longitudinal outcome of preschool-onset depression further supports the significance and robustness of the preschool depression construct.
Preschool depression was also a risk factor for school-age anxiety disorders (odds ratio=3.48) and ADHD (odds ratio=3.69), underscoring its heterotypic in addition to homotypic outcomes. Heterotypic, and well as homotypic, outcomes of prepubertal depression have been reported in several other longitudinal samples (
16,
17). Weissman et al. (
17) have suggested further that children with prepubertal depression and a family history of depression have the highest risk of a recurrence of depression during adulthood. Consistent with the literature on risk for depression in older children, preschool conduct disorder also emerged as a significant predictor of later major depressive disorder. The finding that disruptive disorders are a risk factor for childhood depression has been established in several studies of school-age children (
37). In a previous analysis of this sample, disruptive disorders during the preschool period also emerged as a risk factor for depression at the 2-year follow-up (
6). However, the predictive power of this relationship was diminished in the present study when the effects of nonsupportive parenting were considered in the analysis. Formal testing for mediation showed that the effect of preschool conduct disorder on school-age depression was partially mediated by nonsupportive parenting. This suggests that nonsupport in the context of conduct disorder is an important factor in the mechanism by which the risk for later depression is transmitted. Targeted study of this risk trajectory is indicated.
After accounting for other known significant risk factors, we found that preschool depression remained a highly significant predictor of later meeting full criteria for major depressive disorder. These findings suggest that the preschool diagnosis is a stronger predictor of later major depression than maternal history of depression or traumatic life events. This finding contradicts common clinical belief and practice, in which these latter risk factors are viewed as highly significant risk markers, while symptom characteristics in young children and a preschool depression diagnosis are generally considered more secondarily (or not at all) in the domain of risk for later depression. While these findings do not address the question of whether preschool depression represents minor depression or a risk state, they should dispel any doubt that children with preschool-onset depression constitute a group that is clearly and uniquely at high risk for later depression and therefore should be targeted for early intervention.
This study also provides data to inform the relationship between preschool anxiety disorders and later childhood depression. In contrast to findings in adults and older children, preschool anxiety disorders did not emerge as a precursor of school-age and early adolescent depression. However, preschool depression emerged as a risk factor for school-age anxiety disorders (as well as school-age ADHD). The inconsistency of this finding relative to the established risk trajectory in older children and adults could be related to a number of developmental factors. One possibility is the more transient nature of early-onset anxiety disorders, which in some cases may represent a developmental extreme (e.g., separation anxiety disorder) rather than an enduring clinical disorder.
The most salient limitations of the study include the relatively small sample of children with preschool depression and the fact that the majority of study participants have not yet been followed through puberty. Thus, further studies that carefully track the sample through the pubertal period are needed to identify which preschoolers displaying depressive symptoms will not be at risk for a recurrent course. Nevertheless, the finding that preschool depression is a robust predictor of future major depressive disorder makes a strong case for using validated age-adjusted criteria to identify this early depressive phenotype before school age. The study findings are also of importance when considering that early intervention for depression in the preschool period, a point of high relative neuroplasticity, may provide a window of therapeutic opportunity to alter the chronic and relapsing course known in depressive disorders.