Newborns who will later develop schizophrenia already have discernible motor problems in the first year of life, and by early childhood they show signs of attention difficulties and social withdrawal (
1,
2). Similar behavioral symptoms have been observed in children with attention deficit hyperactivity disorder (ADHD) and autism spectrum disorder (ASD), which suggests the possibility of common underlying neurobiological substrates (
3,
4). Common genetic elements have been identified as well. These illnesses have complex, multigenic risk, but one gene that is associated with all three is
CHRNA7 (
5–
8). Chromosomal copy number variants in the
CHRNA7 region, some isolating the gene itself, have been found in all three illnesses, along with positive association studies and genetic linkage (
6–
8).
CHRNA7 is the most significantly decreased neocortical mRNA in schizophrenia, and it is decreased in ASD as well (
9,
10). The aim of this study was to assess whether this genetic diathesis can be mitigated by an intervention during perinatal brain development.
CHRNA7 and its receptor product, the α7-nicotinic receptor, are expressed at levels nearly one order of magnitude greater in fetuses than in adults or children, including newborns, which is consistent with a developmental role (
11,
12). The α7-nicotinic receptor is activated by acetylcholine in adults, but in fetuses, cholinergic innervation does not reach the cerebrum until near birth, despite the receptor’s appearance at the earliest stage of neuronal development (
13,
14). Choline at millimolar levels is an effective agonist (
15,
16). Millimolar levels of choline are normally present in the amniotic fluid, but high fetal demands for choline for the membrane phospholipids required for fetal growth can overwhelm the mother’s ability to supply fetal needs through synthesis and dietary intake (
17). There are no evidence-based standards for maternal diet, but it is estimated that 20% of pregnant women fail to meet the minimum recommended intake of choline (
17). Maternal plasma levels of choline and its metabolites are associated with development of cognitive function of children as old as 7 years (
18–
21).
We previously reported a double-blind, placebo-controlled intervention with phosphatidylcholine treatment at twice the recommended dietary level in pregnant women (
22). Their newborns received similar supplementation until 52 weeks past the mother’s last menstrual period. The control group received placebo, and both groups received multiple home visits with dietary instruction sufficient to obtain recommended choline levels.
The biomarker of the intervention’s effect was inhibition of the P50 auditory evoked response to the second of paired stimuli measured during the infants’ active sleep, a marker of cerebral inhibition, 1 month after birth. Schizophrenia patients have long been observed to be hypervigilant and to feel “flooded” by sensations in noisy environments (
23,
24). A deficit in the normal decrease in the amplitude of the P50 response to paired auditory stimuli demonstrates an inhibitory deficit that might underlie their decreased sensory filtering and the corresponding difficulty they have in tasks that require focused attention (
25,
26). Diminished P50 response inhibition in newborns has been associated with their parent’s psychosis, the greatest risk factor for future psychotic illness (
27). Newborns’ failure to decrement the P50 response also predicted child behavior problems at 40 months of age, some of which are associated with schizophrenia in adulthood (
28). Our randomized placebo-controlled trial of perinatal phosphatidylcholine supplementation (
22) demonstrated that newborns whose mothers received prenatal phosphatidylcholine supplements were more likely to have normal levels of cerebral inhibition. We hypothesized that the perinatal choline intervention, by normalizing development of cerebral inhibition, would prevent the emergence of behaviors associated with later mental illnesses such as ADHD and schizophrenia. Such behaviors are not observable within the limited newborn behavioral repertoire. The children from this trial have now reached 40 months of age, when parents can reliably discern and rate their child’s behavioral development (
28–
30).
Method
Pregnant Women
Pregnant women were recruited from Denver obstetrical practices toward the end of their first trimester. They had no self-reported illicit substance or medical marijuana use in the past 6 months, no alcohol dependence, and no current nicotine use (confirmed by urinary cotinine levels). Exclusions included maternal history of trimethylaminuria, renal disease, liver disease, Parkinson’s disease, fetal death, fetal congenital malformation, fetal genetic abnormality, current multiparous pregnancy, or fetal abnormality on initial ultrasound examination. The study was approved by the University of Colorado Institutional Review Board. Mothers were compensated for participation in the research project. After written informed consent was obtained, along with the assent of the father when available, women completed a 7-day placebo lead-in. Mothers whose compliance exceeded 70% of capsules at initial medication vial counts were randomly assigned to identical-appearing placebo or drug by gestational week 16. Mothers received standard prenatal care, including standard folate and multivitamin supplements and high-resolution ultrasound examinations during pregnancy. Mothers’ and fathers’ psychiatric histories were elicited via the Structured Clinical Interview for DSM-IV Axis I Disorders. Mild or intermittent anxiety disorders that could generally be avoided by behavioral changes, such as specific phobia and social phobia, were not considered positive. Psychiatric symptoms were defined as current if the mother had sufficient symptoms to meet criteria for an anxiety or depression diagnosis during her pregnancy or had an illness with onset prior to pregnancy with continued symptoms that caused impairment during pregnancy. The study nurse visited mothers at least three times during pregnancy to inquire about compliance with the study medication and prenatal care. Compliance was monitored by capsule counts at all visits.
All participants agreed to abstain completely from smoking by 15 weeks of gestation, before choline was first administered. Eleven mothers smoked intermittently nonetheless, and their infants’ P50 responses were recorded but excluded a priori from the initial analysis of newborn data. Subsequently, this level of smoking was not found to be associated with differences in P50 development. Therefore, the seven children in this group who were available were included in the 40-month analysis. Maternal smoking that is limited to the first trimester has also not been found to cause problems with fetal lung development (
31). Smoking continuously throughout pregnancy may have more deleterious effects. Choline has been shown to have additive effects with nicotine on some parameters of neuron development in the offspring of nonhuman primates exposed to both throughout gestation (
32).
A power analysis conducted before the initiation of the trial showed that the 50 newborns in each treatment group (phosphatidylcholine or placebo) in the 1-month newborn analysis had 85% power for determining a significant difference in P50 stimulus 2/stimulus 1 (S2/S1) ratios of 30%, the primary outcome in the initial phase of the study. The planned enrollment was completed. Stopping criteria—fully detailed in the initial report (
22)—were not reached for any subject; they included serious complications of pregnancy, fetal death, and increase in psychiatric symptoms that could not be controlled through outpatient treatment. Significant dropout occurred for the 40-month follow-up because of mothers’ stressed circumstances and lack of permanent housing.
Choline Administration as Phosphatidylcholine
Choline is catabolized by intestinal flora to trimethylurea, which has an obnoxious odor. Phosphatidylcholine cannot be catabolized, is well absorbed, and, once absorbed, is interchangeably metabolized with choline; oral intake of phosphatidylcholine increases serum choline levels (
17). Doses of 3,600 mg each morning and 2,700 mg each evening were administered beginning at or before 16 weeks after the mother’s last menstrual period, continuing until delivery. Phosphatidylcholine is 13%−15% choline; thus, this dosage should provide approximately 900 mg of choline per day, about the same amount as in three large eggs. All mothers, regardless of treatment assignment, were fully advised of dietary practices that would result in similar levels of choline intake. After birth, infants received 600 mg of phosphatidylcholine once daily in an oral suspension, approximately equivalent to 100 mg choline, or placebo, the same treatment assignment as in utero. Choline supplementation continued for the infant until 52 weeks after the mother’s last menstrual period before the pregnancy (until approximately 3 months of age) as estimated by first-trimester ultrasound. The Institute of Medicine recommendation for daily adequate choline intake for infants is 125 mg/day (
33).
Phosphatidylcholine was administered as capsules or drops (Nutrasal, Scottsdale, Ariz.). The placebo was corn oil, which is quite low in choline and, as dispensed in identical-appearing capsules, indistinguishable from the active treatment. All clinical personnel were blind to treatment except the pharmacist and the statistician who prepared the randomization scheme. The capsules were dispensed in bottles labeled “Experimental Drug.”
Electrophysiological and genetic methods were reported previously (
22).
Parent Report of Child Behavior
The Child Behavior Checklist, version 1.5-5, has 99 items, each scored in a range of 0–2 (
29). Subsets of items are grouped as subscales (attention, aggression, emotionality, anxious/depressed, sleep, somatic, and withdrawn). The internal reliability ranges from acceptable to excellent (Cronbach’s alpha values, 0.66–0.95). The externalizing subscale is the sum of the attention and aggression items; the internalizing subscale is the sum of the emotionality, anxious/depressed, somatic, and withdrawn items. All item scores are added for a total problems score, which also includes some items not in any subscale.
The clinical trials registration extended only to 18 months for safety follow-up studies. Testing with the Mullen Scales of Early Learning (
43) at 12 months showed no differences between the two treatment groups (
22). The 40-month follow-up was originally not deemed to be practical and therefore was not specified as an outcome before the trial began. Although the follow-up study thus did not have a prespecified primary outcome, all parameters—Child Behavior Checklist subscales, dichotomization of P50 S2/S1 ratios, and
CHRNA7 genotype—were specified in previous studies (
5,
22,
27,
28,
34).
Statistical Analysis
As in the previous study, effects of phosphatidylcholine treatment compared with placebo on Child Behavior Checklist scales were assessed by an analysis of variance with the Child Behavior Checklist scores converted to rank scores and gender, treatment, and genotype as main effects (
28). Interactions were added to test for moderation. There were no outliers, and no data were excluded. The SAS procedure GLM was used to execute the analysis of variance. The threshold for significance was an alpha of 0.05 (two-tailed).
Results
Childhood Behavioral Symptoms
Of the 100 pregnant women initially enrolled, 86 delivered children from whom we recorded auditory evoked potentials at 1 month; of these, 49 were rated on the Child Behavior Checklist at 40 months by a parent (48 by the mother and one by the father) (see Figure S1 in the
data supplement that accompanies the online edition of this article). The 50% loss from the initial enrollment at 40 months is consistent with the disadvantaged socioeconomic status and lack of permanent housing of the mothers, a population in whom dietary supplementation might most be needed. There was no attrition attributable to a specific demographic difference between those who remained in study and those who did not, nor to participants’ initial assignment or response to choline (
Table 1).
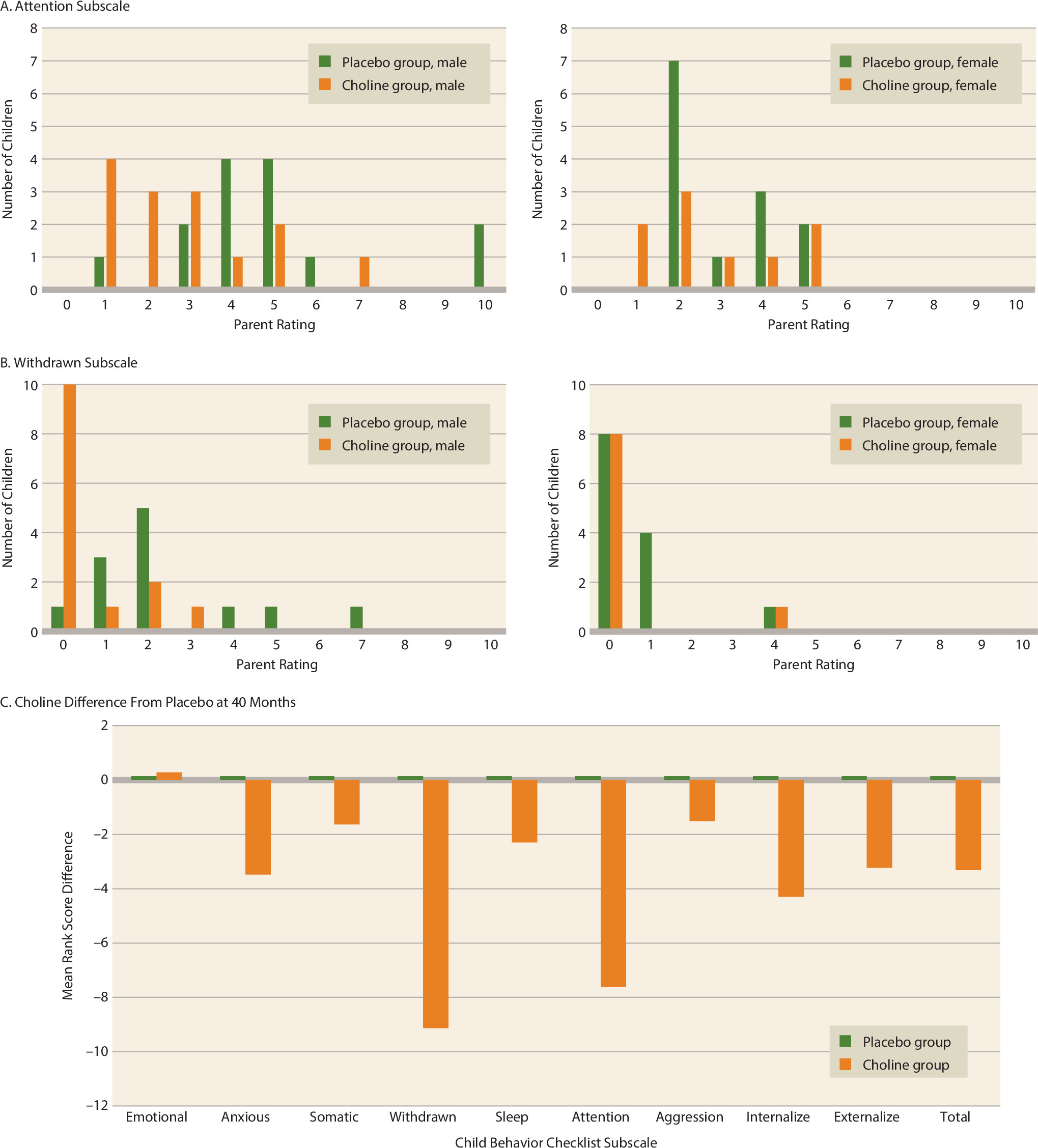
The parents were not aware of their child’s earlier treatment group. Parent ratings on the Child Behavior Checklist attention subscale were significantly lower in those children who had been treated with choline (gender-adjusted F=4.56, df=1, 46, p=0.038) (
Figure 1A). Parent ratings on the withdrawn subscale were also significantly lower (gender-adjusted F=9.61, df=1, 46, p=0.003) (
Figure 1B). The complete statistical model is presented in Table S1 in the online
data supplement. Scores for other primary behavior problems, the externalizing and internalizing subscales, and total problems were lower as well, but the differences between groups did not reach significance (
Figure 1C). Only the withdrawn subscale remained significant after Bonferroni correction for the 10 Child Behavior Checklist axes (p=0.033).
Moderation by CHRNA7 Genotype
In addition to its
CHRNA7 agonist function, choline has fetal roles in membrane synthesis and one-carbon metabolism; the latter two require lower choline concentrations (
15,
35,
36). In animal models, α7-nicotinic receptor activation is required for the effect of choline on inhibitory neurotransmission. In vitro, tissues derived from
Chrna7 null mouse mutants do not show prenatal conversion of chloride transporter and development of inhibition; in vivo,
Chrna7 null mutants do not respond to perinatal choline treatments with increased inhibition of the murine analog of human P50 responses (
37,
38). A similar definitive test of the specific action of choline on α7-nicotinic receptors is not possible in humans. However, we genotyped the children for
CHRNA7 rs3087454, a 5′ promoter single-nucleotide polymorphism (SNP).
CHRNA7 rs3087454 was chosen because its minor allele was previously associated with both schizophrenia and diminished effects of an α7-nicotinic agonist in adults (
34,
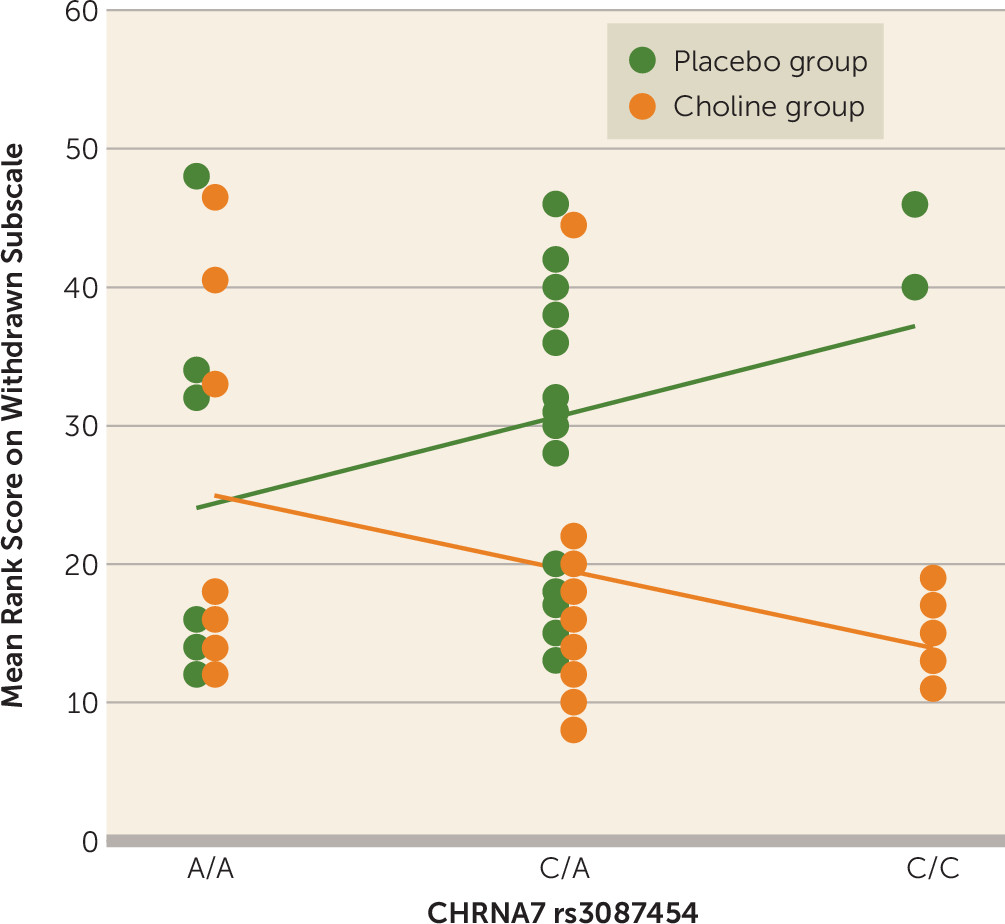
39). The effect of choline treatment is moderated by the child’s
CHRNA7 rs3087454 genotype; the interaction between the effect of choline and the effect of the
CHRNA7 SNP is significant for score on the withdrawn subscale (gender-adjusted F=4.41, df=1, 39, p=0.042) (
Figure 2; see also Table S1 in the online
data supplement).
Relationship to Neonatal Cerebral Inhibition
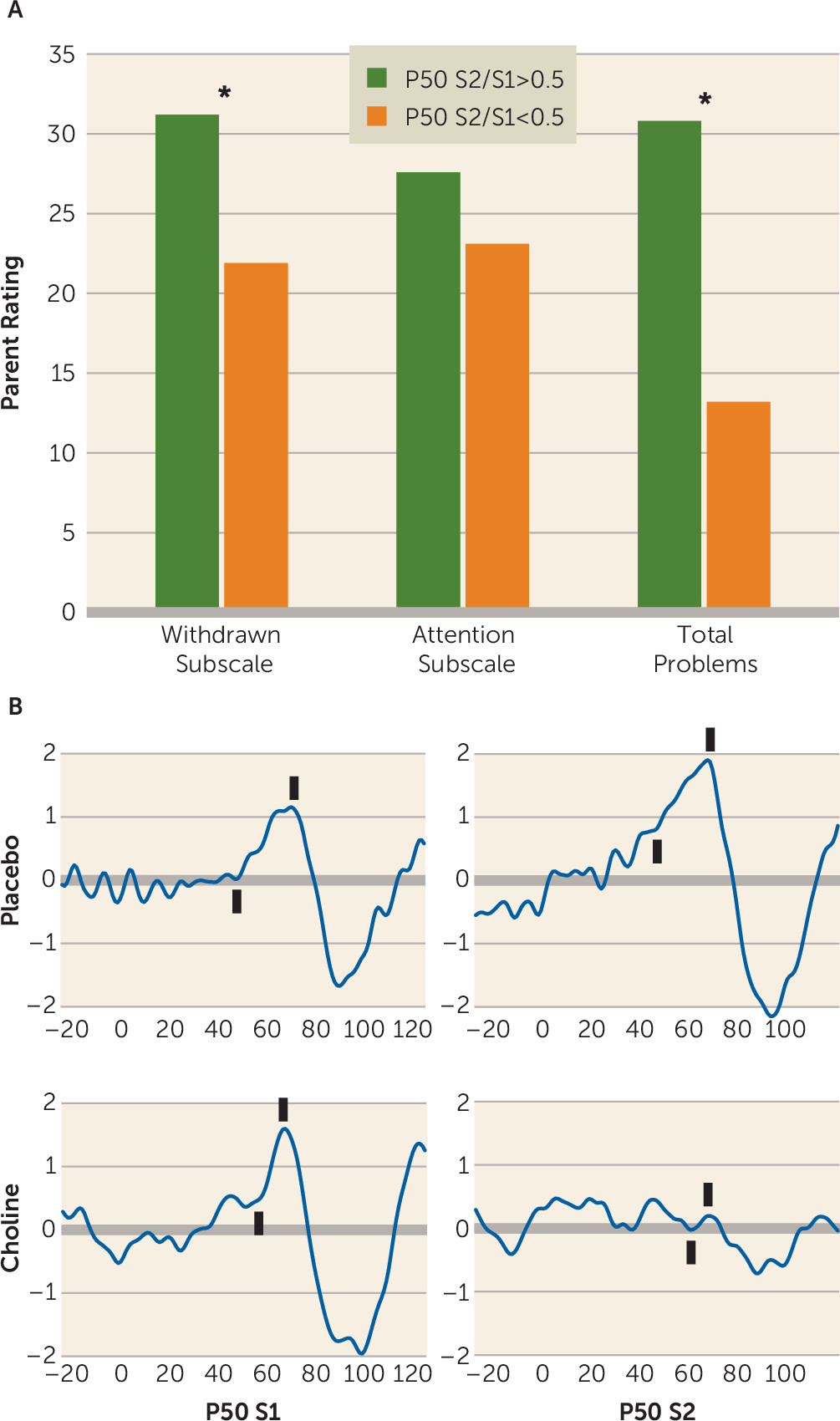
The 40-month Child Behavior Checklist ratings were also related to newborn P50 inhibition, with significant effects on scores for both the withdrawn subscale and total problems (
Figure 3A,B). A similar analysis was performed in a previous study in 50 children who were recorded as newborns but were not in the intervention trial (
38). That study found significant effects of newborn P50 S2/S1 ratio on 40-month Child Behavior Checklist ratings for total problems and the anxious/depressed and attention subscales. In the present study, significant effects of P50 S2/S1 ratio were found for total problems and the withdrawn subscale (
Figure 3A).
Further Follow-Up
Thirty-two mothers returned at 48 months to complete the Child Behavior Checklist a second time. This subsample was now too small to find significant differences, but the findings were qualitatively similar at 40 and 48 months. Ratings at 48 months correlated with those at 40 months for the withdrawn subscale (r=0.53, p=0.002), the attention subscale (r=0.54, p=0.001), and total problems (r=0.68, p<0.001).
Discussion
Mental illness, despite its early developmental basis, typically emerges gradually in the first three decades of life. Perinatal choline supplementation reduced the frequency of attention and social problems already noticed by the parents of children in this study. The earliest signs of schizophrenia include childhood symptoms of withdrawal and attention disturbance, symptoms we have now found to be modified as early as 40 months by choline supplementation (
2). A study by another group obtained retrospective Child Behavior Checklist ratings before 3 years of age from parents of schizophrenia patients and found increased ratings for the attention (effect size d′=0.45) and withdrawn (d′=1.73) subscales, the symptoms with the highest predictive value for later schizophrenia (
40). In the present study, choline supplementation produced decreases of comparable magnitude (for the attention subscale, d′=0.59; for the withdrawn subscale, d′=0.79). These symptoms are also prominent in both ADHD and ASD (
3,
4). Schizophrenia itself does not generally manifest this early in life, and its incidence is too infrequent to be observable in anything short of a population cohort. Even the conversion to schizophrenia in individuals who already have psychotic symptoms occurs at rates less than 50% (
41).
Although attention and withdrawal problems have high significance for indicating the risk for future mental illness, the ratings for total problems and the scores for both internalizing and externalizing problems, although lower for the children in the phosphatidylcholine group, were not significantly changed. We were not able to stratify the 40-month sample post hoc for presence or absence of parental psychopathology that would also indicate future risk for the child. However, in the larger 1-month sample, where the P50 S2/S1 ratio was the outcome measure, we conducted such a stratification and found similar effects in both subgroups. Only 45% of the newborns of mothers with anxiety, depression, psychosis, or nicotine use who were treated with placebo had P50 ratios <0.5, compared with 53% of those whose mothers did not have these risk factors. For newborns in the phosphatidylcholine group, 76% of those whose mothers had these risk factors had P50 ratios <0.5, compared with 83% of those whose mothers did not. We also recruited a small cohort of women with psychosis themselves or in the father of their child. Of 27 enrolled over 5 years, 17 had newborns who completed the 1-month recording, reflecting the difficulty of this population. Among those treated with placebo, 38% had a P50 ratio <0.5, compared with 69% of those treated with phosphatidylcholine. Thus, even for this very-high-risk group, the treatment appears to be effective. In all samples, no families ever asked to withdraw or were withdrawn for adverse effects. Attrition was caused by loss of contact as mothers moved between temporary addresses.
Prenatal folic acid supplementation is now general medical practice to decrease the incidence of cleft palate, spina bifida, and other neurodevelopmental abnormalities. Unlike prevention of mental illness, these abnormalities are evident at birth and immediately verify the value of high-dose folate supplementation. In the present study, repeated dietary instruction alone was insufficient for the placebo group to benefit fully, and pharmacological doses of phosphatidylcholine were required. A similar requirement for pharmacological doses of folate despite good diet was found in population cohort studies of its effects, and pharmacological treatment with folate is effective even with poor diet (
42).
Because of the sample size and the attrition over the 6 months of gestation and 4 years of childhood to only 50% of the enrolled sample, our results are preliminary and require further verification. Larger samples followed up later into childhood and adulthood are needed to provide definitive data on the value of phosphatidylcholine supplementation, but currently no similar controlled trials are listed in public registries. Initiation of a new trial would not produce results in 40-month-old children for 4 years, which makes the present results unique.
The outcome of the fetal stage of brain development has lifelong consequences for mental function, and there is little prospect of reversing these developmental problems later in life when mental illnesses appear. Thus, perinatal intervention, even before individuals at risk for mental illness can be identified, is the only opportunity for potentially reversing this initial major aspect of the pathogenesis of mental illness. A primary, low-cost, low-risk intervention during fetal development will not prevent all cases of mental illness, but even a partial decrease in their incidence or severity would have substantial global value.
Acknowledgments
The authors thank Drs. Steve Zeisel for his help in study design and Drs. William Hay, Henry Galan, Brian Stafford, and Kim Kelsay for their role on the data safety monitoring board.