Polygenic Risk: Predicting Depression Outcomes in Clinical and Epidemiological Cohorts of Youths
Publication: American Journal of Psychiatry
Abstract
Objective:
Identifying risk factors for major depression and depressive symptoms in youths could have important implications for prevention efforts. This study examined the association of polygenic risk scores (PRSs) for a broad depression phenotype derived from a large-scale genome-wide association study (GWAS) in adults, and its interaction with childhood abuse, with clinically relevant depression outcomes in clinical and epidemiological youth cohorts.
Methods:
The clinical cohort comprised 279 youths with major depression (mean age=14.76 years [SD=2.00], 68% female) and 187 healthy control subjects (mean age=14.67 years [SD=2.45], 63% female). The first epidemiological cohort included 1,450 youths (mean age=13.99 years [SD=0.92], 63% female). Of those, 694 who were not clinically depressed at baseline underwent follow-ups at 6, 12, and 24 months. The replication epidemiological cohort comprised children assessed at ages 8 (N=184; 49.2% female) and 11 (N=317; 46.7% female) years. All cohorts were genome-wide genotyped and completed measures for major depression, depressive symptoms, and/or childhood abuse. Summary statistics from the largest GWAS to date on depression were used to calculate the depression PRS.
Results:
In the clinical cohort, the depression PRS predicted case-control status (odds ratio=1.560, 95% CI=1.230–1.980), depression severity (β=0.177, SE=0.069), and age at onset (β=−0.375, SE=0.160). In the first epidemiological cohort, the depression PRS predicted baseline depressive symptoms (β=0.557, SE=0.200) and prospectively predicted onset of moderate to severe depressive symptoms (hazard ratio=1.202, 95% CI=1.045–1.383). The associations with depressive symptoms were replicated in the second epidemiological cohort. Evidence was found for an additive, but not an interactive, effect of the depression PRS and childhood abuse on depression outcomes.
Conclusions:
Depression PRSs derived from adults generalize to depression outcomes in youths and may serve as an early indicator of clinically significant levels of depression.
Major depressive disorder is characterized by persistent depressed mood and/or anhedonia in conjunction with a constellation of other clinically significant symptoms. This severe psychiatric disorder is associated with lifelong poor mental health and general medical outcomes (1). A large body of research has shown that, in addition to the full syndrome of major depression, subsyndromal depressive symptoms in youths are associated with reduced quality of life and are a strong predictor of later major depression (2–5). Although this debilitating disorder and related symptoms can emerge at any age, their prevalence markedly increases during puberty (6). Accordingly, identifying early risk factors for major depression and potentially clinically significant depressive symptoms, especially during sensitive developmental stages such as childhood and adolescence, could have important implications for prevention efforts.
Major depression is a heritable psychiatric disorder. Heritability estimates from family studies range up to 40% (7), and estimates of heritability based on single-nucleotide polymorphisms (SNPs) range up to 8.7% (8). Despite the high heritability, efforts to uncover specific genetic variants associated with major depression through genome-wide association study (GWAS) designs have historically been unsuccessful (9). Building on research demonstrating the high genetic correlation of self-reported depressive symptoms and a clinical diagnosis of major depression (8), more recent GWASs have focused on a broader phenotype of depression. With >460,000 participants, the recent meta-analysis from the Psychiatric Genomics Consortium successfully identified 44 genome-wide significant loci associated with the broad phenotype of clinically diagnosed major depression and self-reported diagnosis of depression (8). GWAS results strongly suggest that this broad construct of depression is a complex, polygenic phenotype. One of the methods used to study such complex disorders involves polygenic risk scores (PRSs) (10). PRSs are created by taking genetic variants up to varying thresholds of significance from a GWAS discovery sample and applying a score from these variants, weighted by the associations in the discovery sample, to predict a trait in an independent target sample. PRSs hold great promise for supporting the identification of disease risk within different contexts, including identifying individuals at high risk for disease onset at an early age (10). Indeed, Wray et al. (8) found higher depression PRSs among adult case subjects who reported an early age at onset retrospectively; however, this has not been examined in youths.
In this study, we addressed whether GWAS signals built on reports of self-reported or clinically evaluated major depression in adult cohorts map onto depression status and other important clinical features of depression (e.g., severity, age at onset) in a clinical sample of youths with major depression and healthy control subjects. We also examined this broad depression PRS as a predictor of depressive symptoms (cross-sectionally and prospectively) among premorbid youths from epidemiological samples to establish whether this PRS can be used to identify at-risk individuals prior to the onset of clinically significant depressive symptoms. Lastly, we examined the additive and interactive effect of this depression PRS with exposure to childhood abuse, a robust environmental predictor of early age at onset of major depression (11). These analyses inform whether, and under what conditions, broad depression PRSs derived from adults generalize to depression and depressive symptoms in youths and serve as an early indicator of clinically significant levels of depression.
Methods
Samples
The clinical cohort comprised 279 Caucasian children and adolescents 7–18 years old with a current diagnosis or history of major depression and 187 healthy control subjects (ages 7–18 years old) with no past history of or current psychiatric disorders. Exclusion criteria included a current or past diagnosis of attention deficit hyperactivity disorder, schizophrenia, bipolar disorder, or autism spectrum disorder. Youths with other comorbid diagnoses were included (see Table S1 in the online supplement ).
The first epidemiological cohort comprised 1,450 12- to 17-year-old Caucasian adolescents recruited through schools. After the study entry assessment, participants with elevated levels of depressive symptoms entered an established prevention program targeting depression (12) and were not included in the follow-up analyses in this study. However, 694 participants with depressive symptoms below this cutoff who did not enter the prevention study were tracked over time, with follow-up assessments occurring at 6, 12, and 24 months after study entry.
The replication epidemiological cohort comprised genotyped youths at ages 8 (N=184) and 11 years (N=317) derived from a longitudinal prospective study of healthy infants born in 1998 in Helsinki (13).
All studies were approved by the local ethics committees and were conducted in accordance with the current version of the Declaration of Helsinki. All study subjects completed assent forms, and their parents completed consent forms prior to participation (see the online supplement for further description of the cohorts and recruitment procedures).
Psychometric Measures
Clinical cohort.
A well-established diagnostic interview (the Diagnostic Interview for Mental Disorders in Childhood and Adolescence) (14) was used to determine the presence or absence of ICD-10 diagnoses and age at onset of clinical depression. To assess the severity of depressive symptoms, the Depression Inventory for Children and Adolescents (15) was administered to youths ≤12 years old, and the Beck Depression Inventory–II (BDI-II) (16) was administered to participants >12 years old. Both instruments are commonly used self-report measures with good psychometric properties (15, 16), with higher scores suggesting greater depression severity. Scores from the Depression Inventory for Children and Adolescents and the BDI-II were standardized using z scores to perform the analyses on the whole sample.
Childhood abuse was measured with four items capturing emotional (i.e., yelled at and insulted at home), physical (i.e., beaten at home, victim of violence), and sexual abuse (i.e., victim of unwanted sexual acts) on a self-report questionnaire adapted from the Life Event Survey (17) and the Munich Life Event List (18). Each item was rated dichotomously (“yes” or “no”). Participants who endorsed any of these items positively were rated as having a history of abuse (see the online supplement for a more detailed description of the measure).
The first epidemiological cohort.
The Children’s Depression Inventory (CDI) (19, 20), a well-established self-report measure assessing depressive symptoms in youths, was administered. The CDI has been found to distinguish youths with depressive disorders from nondepressed youths (21). It was administered at study entry and then at 6, 12, and 24 months after study entry. The CDI total score was examined as a continuous measure in the cross-sectional analyses, with higher scores indicating higher levels of depression.
In addition to the CDI, a semistructured clinical diagnostic interview (Adolescent–Longitudinal Interval Follow-Up Evaluation) (based on an unpublished 2017 study of A.P. Soares de Matos, et al., available from the authors) was administered at follow-up time points. However, because substantially fewer participants completed this interview, we used moderate to severe levels of depressive symptoms based on the CDI (cutoff CDI score of ≥19) (19, 21) in the survival analyses to preserve statistical power (see Table S2 in the online supplement ). There was good congruent validity between the CDI and the diagnostic interview in this study; few participants met criteria for major depressive disorder on the diagnostic interview and did not score within the moderate to severe range on the CDI (three participants at the 6-month follow-up, two at the 12-month follow-up, and none at the 24-month follow-up). These participants were coded as cases in the survival analyses to capture all participants with clinically significant depressive symptoms since the last assessment, given that the CDI assesses depressive symptoms over the past 2 weeks. In other words, youths with potentially clinically significant depressive symptoms, as defined by the moderate to severe cutoff on the CDI, and/or a diagnosis of major depression according to a clinical interview, were considered cases in the longitudinal analyses.
The emotional, physical, and sexual abuse subscales of the Childhood Trauma Questionnaire (22) were used to measure abuse history. Scores on each subscale were categorized into none, mild, moderate, or severe levels of abuse based on predetermined cutoff scores (22). Youths endorsing moderate to severe levels on any of the scales were coded as having a history of abuse.
The replication epidemiological cohort.
Depressive symptoms were assessed with the depressive problems subscale of the Child Behavior Checklist (23), a standardized and validated rating scale. The checklist was completed by each parent when the child was 8 and 11 years old. As recommended in the manual, raw scores were analyzed.
Given the well-documented sex differences in depressive symptoms and the increase of depressive symptoms during adolescence compared with childhood (24, 25), all analyses were adjusted for sex and age. Similarly, parental education was used as a proxy for socioeconomic status and included as a covariate, given its association with depressive symptoms (26).
Genotyping Methods
DNA was extracted from EDTA blood in the clinical cohort using the automated system from the Chemagic 360 instrument from PerkinElmer (Waltham, Mass.), which applies a magnetic bead–based method for extraction and purification of nucleic acids from different tissues. In the first epidemiological cohort, saliva was obtained from each participant using Oragene saliva kits (DNA Genotek, Ottawa), and DNA was extracted using the same automated system as in the clinical cohort. In both cohorts, genotyping was performed with the Infinium Global Screening Array protocol (Illumina, San Diego), measuring >640,000 SNPs.
In the replication epidemiological cohort, DNA was extracted from blood samples (N=80) and saliva samples (N=277), and genotyping was performed with the Illumina OmniExpressExome 1.2 BeadChip (Illumina, San Diego), measuring >962,000 SNPs, according to standard protocols. See the online supplement for quality control and population stratification procedures.
Data Analysis
Multiple imputation was used to handle missing phenotype data (see the supplemental Methods section and Table S3 in the online supplement ). Group differences in demographic and clinical characteristics were examined with chi-square analyses and t tests. Depression PRSs were calculated from the imputed best guess genotypes using GWAS summary statistics from the latest Psychiatric Genomics Consortium study on major depressive disorder (8). Seven PRSs using different p-value thresholds of the GWAS summary statistics were calculated using PRSice (27) (in the online supplement , see the supplemental Methods section for further description and Table S4 for the number of SNPs included by threshold). Prediction accuracy was assessed using Nagelkerke’s pseudo R2.
Multivariate regression models were used to assess the association of the depression PRS and childhood abuse with each outcome. In total, three models were applied to each outcome measure: the main effect of the PRS (gene [G] model; the effect of G plus covariates on depression outcomes), an additive model (gene plus environment [G+E] model; the effect of G+E plus covariates on depression outcomes), and an interaction model (G×E model; the effect of G+E plus G×E plus covariates on depression outcomes). Analysis of variance (ANOVA) model comparisons were used to determine whether each model added explanatory value over the reduced model (i.e., null model containing only covariates compared with G model, G model compared with G+E model, G+E model compared with G×E model). Models that significantly differed from the reduced model were interpreted. See the online supplement for a description of variable coding. To control for the error rate related to multiple comparisons, false-discovery-rate correction was applied using the p.adjust function in R.
Power and area under the curve (AUC) analyses in the longitudinal analyses were calculated in R (using the packages AVENGEME and survivalROC, respectively). Using the SNPs included with the p threshold of 0.05 and the explained genetic variance set to 4% in the training set, the power was 64.9% in the clinical cohort. The power of the analyses in the epidemiological cohort was 5% using the p threshold of 0.05 and the explained genetic variance set to 0.1%. The power curves by effect size for the clinical and first epidemiological cohorts are presented in Figure S1 in the online supplement .
Given the small effect size in the epidemiological cohort, the predictive effect of the depression PRS on depressive symptoms in youths was replicated in a second, independent epidemiological cohort. The combined p value from the four regressions conducted (maternal and paternal report at ages 8 and 11) was calculated using the Fisher combined probability test (survcomp package in R).
Results
Table 1 presents demographic and clinical characteristics for the cohorts.
| Clinical Cohort | Replication Epidemiological Cohort | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Characteristic | Case Subjects (N=279) | Control Subjects (N=187) | Epidemiological Cohort (N=1,450) | Age 8 (N=184) | Age 11 (N=317) | |||||
| N | % | N | % | N | % | N | % | N | % | |
| Female | 190 | 68.1 | 118 | 63.1 | 914 | 63.0 | 91 | 49.2 | 148 | 46.7 |
| Maternal educationa | ||||||||||
| Less than secondary school | 10 | 3.6 | 2 | 1.0 | 708 | 48.8 | 67 | 36.4 | 111 | 35.0 |
| Secondary school or more | 269 | 96.4 | 185 | 98.9 | 742 | 51.2 | 117 | 63.6 | 206 | 65.0 |
| Paternal education | ||||||||||
| Less than secondary school | 13 | 4.7 | 5 | 2.7 | 834 | 57.5 | — | — | — | — |
| Secondary school or more | 266 | 95.3 | 182 | 97.3 | 616 | 42.5 | — | — | — | — |
| Childhood abuse | — | — | — | — | ||||||
| None | 131 | 47.0 | 118 | 63.1 | 1,049 | 72.3 | — | — | — | — |
| One or more mild abuse types | 148 | 53.0 | 69 | 36.9 | 269 | 18.6 | — | — | — | — |
| One or more moderate abuse types | — | — | — | — | 86 | 5.9 | — | — | — | — |
| One or more severe abuse types | — | — | — | — | 46 | 3.2 | — | — | — | — |
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | |
| Age | 14.76 | 2.00 | 14.67 | 2.45 | 13.99 | 0.92 | 8.12 | 0.30 | 11.32 | 0.52 |
| Depressive symptomsb | ||||||||||
| Self-report | 0.19 | 0.95 | –1.11 | 0.21 | 11.53 | 7.71 | — | — | — | — |
| Maternal report | — | — | — | — | — | — | 55.30 | 6.06 | 55.24 | 6.48 |
| Paternal report | — | — | — | — | — | — | 53.48 | 5.28 | 53.60 | 5.74 |
a
Parental education was coded as the highest education of either the father or the mother in the Finnish cohort.
b
Depressive symptoms were assessed with the Depression Inventory for Children and Adolescents or the Beck Depression Inventory–II in the clinical cohort (scores have been standardized), the Children’s Depression Inventory in the epidemiological cohort, and the Child Behavior Checklist (t scores reported) in the replication epidemiological cohort.
Clinical Cohort
The depression PRS significantly predicted case-control status, depression severity, and age at onset, with the prediction accuracy typically plateauing at p thresholds of 0.05 and 0.10 (Table 2). The depression PRS explained the most variance in case-control status, or 5%, followed by 1.8% of the variance in depression severity and 1.6% in age at onset among the case subjects. By comparison, this depression PRS (at a p threshold of 0.05) has previously been found to explain 1.9% of the variance in liability to major depression in adults (8).
| Clinical Cohort | Epidemiological Cohort | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Case-Control Status | Depression Severity | Age at Onset | Depressive Symptoms | Longitudinal Analyses | |||||||||||
| p Threshold | FDR | Original p | R2 | FDR | Original p | R2 | FDR | Original p | R2 | FDR | Original p | R2 | FDR | Original p | R2 |
| p<5×10−8 | 0.965 | 0.965 | 0 | 0.307 | 0.307 | 0.000 | 0.433 | 0.433 | 0 | 0.834 | 0.834 | 0 | 0.098 | 0.067 | 0.004 |
| p<1×10−5 | 0.915 | 0.784 | 0.048 | 0.051 | 0.029 | 0.014 | 0.076 | 0.054 | 0.009 | 0.584 | 0.500 | 0.000 | 0.367 | 0.367 | 0.001 |
| p<1×10−4 | 0.230 | 0.164 | 0.006 | 0.045 | 0.019 | 0.017 | 0.037 | 0.005 | 0.021 | 0.099 | 0.071 | 0.001 | 0.098 | 0.070 | 0.004 |
| p<1×10−3 | 0.136 | 0.078 | 0.010 | 0.087 | 0.074 | 0.008 | 0.176 | 0.148 | 0.004 | 0.028 | 0.012 | 0.003 | 0.180 | 0.154 | 0.002 |
| p<0.01 | 0.003 | 0.001 | 0.030 | 0.036 | 0.01 | 0.021 | 0.047 | 0.016 | 0.015 | 0.042 | 0.024 | 0.003 | 0.098 | 0.054 | 0.005 |
| p<0.05 | 4.97×10−4 | 1.17×10−4 | 0.050 | 0.029 | 0.004 | 0.018 | 0.047 | 0.02 | 0.016 | 0.020 | 0.005 | 0.004 | 0.067 | 0.010 | 0.009 |
| p<0.10 | 4.97×10−4 | 1.42×10−4 | 0.047 | 0.075 | 0.053 | 0.010 | 0.067 | 0.038 | 0.010 | 0.020 | 0.006 | 0.004 | 0.067 | 0.019 | 0.007 |
a
Nagelkerke’s pseudo R2 reflects the improvement in model fit generated by adding a polygenic risk score as a predictor to the model. FDR=false-discovery-rate-corrected p value; GWAS=genome-wide association study.
To illustrate the findings, the p threshold of 0.05 for the depression PRS was used, given that this cutoff was most consistent in significantly predicting the clinical features of depression and was found to explain most of the variance in depression status and severity. Higher depression PRSs were observed in case subjects relative to control subjects (odds ratio=1.560, 95% CI=1.230–1.980, corrected p=0.001; Figure 1A; see Table 3 for model comparisons). Similarly, Figure 1B displays the positive quantitative relationship between depressive symptoms and the depression PRS (β=0.177, SE=0.069, corrected p=0.010). In addition, case subjects with an earlier age at onset had a higher depression PRS than those with a later onset of major depression (β=−0.375, SE=0.160, corrected p=0.036; Figure 1C).
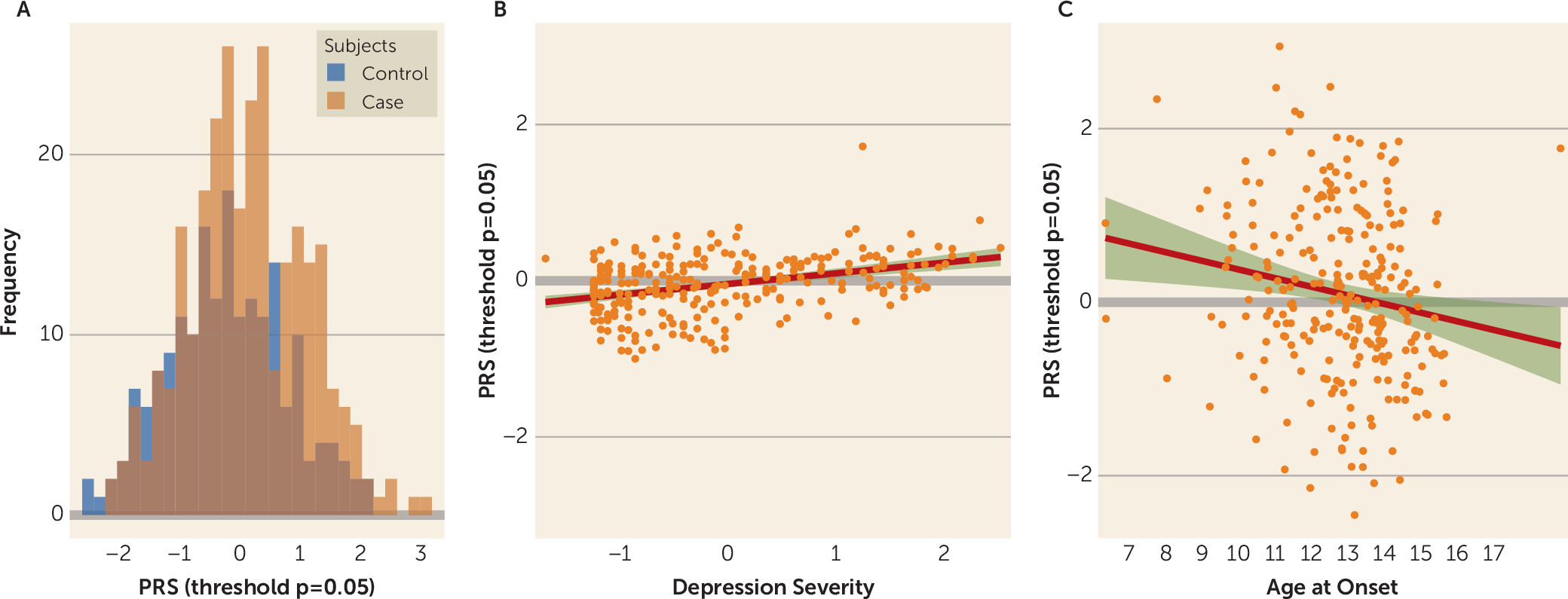
FIGURE 1. Depression polygenic risk score (PRS), depressive symptoms, and age at onset of depression in a clinical cohort of children and adolescentsa
aThe distribution of the depression PRS at a threshold of p=0.05 in the clinical cohort by group status (i.e., case and control subjects) is shown in panel A. Overlap between case and control subjects is indicated by the brown bars. Depression PRSs are shown at a threshold of p=0.05 by standardized scores of depression severity (panel B) and by age at onset in the clinical cohort (panel C). The PRS at a threshold of p=0.05 has been standardized in the models, and the shading represents 95% confidence intervals.
| Cohort, Outcome, and Model | Variable | Odds Ratio, β, or Hazard Ratio | SE | 95% CI | p (false-discovery-rate-corrected) | Original p | R2 | Model Comparison (p) |
|---|---|---|---|---|---|---|---|---|
| Clinical cohort | ||||||||
| Case-control status (odds ratio) | ||||||||
| Null model | — | — | — | — | — | — | 0.030 | — |
| G | PRS | 1.560 | 1.130 | 1.230, 1.980 | 0.001 | 2.48×10−4 | 0.079 | 1.637×10−4 |
| G+E | PRS | 1.578 | 1.135 | 1.230, 2.024 | 0.002 | 3.39×10−4 | 0.179 | 2.807×10−11 |
| Childhood abuse | 3.924 | 1.292 | 2.376, 6.472 | 8.12×10−4 | 9.020×10−8 | |||
| G×E | PRS | 1.677 | 1.171 | 1.231, 2.284 | 0.003 | 0.001 | 0.181 | 0.436 |
| Childhood abuse | 3.896 | 1.289 | 2.366, 6.411 | 8.12×10−4 | 8.950×10−8 | |||
| PRS and childhood abuse interaction | 0.838 | 1.300 | 0.502, 1.401 | 0.501 | 0.501 | |||
| Depression severity (β) | ||||||||
| Null model | — | — | — | — | — | — | 0.058 | — |
| G | PRS | 0.177 | 0.069 | 0.021, 0.288 | 0.010 | 0.004 | 0.077 | 0.004 |
| G+E | PRS | 0.149 | 0.066 | 0.019, 0.279 | 0.043 | 0.026 | 0.135 | 1.220×10−4 |
| Childhood abuse | 0.494 | 0.126 | 0.247, 0.741 | 0.002 | 6.20×10−4 | |||
| G×E | PRS | 0.239 | 0.091 | 0.060, 0.417 | 0.020 | 0.009 | 0.139 | 0.153 |
| Childhood abuse | 0.519 | 0.127 | 0.270, 0.768 | 0.087 | 6.250×10−5 | |||
| PRS and childhood abuse interaction | –0.187 | 0.131 | –0.444, 0.069 | 0.184 | 0.153 | |||
| Age at onset (β) | ||||||||
| Null model | — | — | — | — | — | — | 0.443 | — |
| G | PRS | –0.375 | 0.160 | –0.688, –0.062 | 0.036 | 0.020 | 0.459 | 0.024 |
| G+E | PRS | –0.374 | 0.158 | –0.683, –0.065 | 0.036 | 0.019 | 0.471 | 0.040 |
| Childhood abuse | –0.600 | 0.289 | –1.167, –0.034 | 0.060 | 0.040 | |||
| G×E | PRS | –0.191 | 0.238 | –0.658, 0.276 | 0.450 | 0.425 | 0.471 | 0.307 |
| Childhood abuse | –0.540 | 0.295 | –1.118, 0.038 | 0.089 | 0.069 | |||
| PRS and childhood abuse interaction | –0.321 | 0.313 | –0.934, 0.292 | 0.345 | 0.307 | |||
| Epidemiological cohort | ||||||||
| Depressive symptoms (β) | ||||||||
| Null model | — | — | — | — | — | — | 0.071 | — |
| G | PRS | 0.557 | 0.200 | 0.167, 0.947 | 0.012 | 0.005 | 0.075 | 0.005 |
| G+E | PRS | 0.439 | 0.196 | 0.055, 0.823 | 0.038 | 0.025 | 0.107 | 5.071×10−13 |
| Childhood abuse | 4.935 | 0.677 | 3.609, 6.262 | 6.080×10−6 | 5.070×10−13 | |||
| G×E | PRS | 0.346 | 0.206 | –0.057, 0.748 | 0.112 | 0.093 | 0.108 | 0.131 |
| Childhood abuse | 4.642 | 0.704 | 3.262, 6.022 | 3.620×10−4 | 6.040×10−11 | |||
| PRS and childhood abuse interaction | 1.010 | 0.669 | –0.301, 2.320 | 0.143 | 0.131 | |||
| Epidemiological cohort | ||||||||
| Prospective moderate to severe depressive symptoms (hazard ratio) | ||||||||
| Null model | — | — | — | — | — | — | 0.035 | — |
| G | PRS | 1.202 | 0.071 | 1.045, 1.383 | 0.020 | 0.010 | 0.044 | 0.010 |
| G+E | PRS | 1.171 | 0.073 | 1.016, 1.350 | 0.039 | 0.029 | 0.078 | 4.302×10−7 |
| Childhood abuse | 2.817 | 0.184 | 1.963, 4.043 | 6.750×10−5 | 1.940×10−8 | |||
| G×E | PRS | 1.194 | 0.079 | 1.024, 1.393 | 0.038 | 0.024 | 0.079 | 0.514 |
| Childhood abuse | 2.942 | 0.193 | 2.015, 4.294 | 6.750×10−5 | 2.250×10−8 | |||
| PRS and childhood abuse interaction | 0.877 | 0.201 | 0.592, 1.300 | 0.513 | 0.513 | |||
a
All the models have been adjusted for age, sex, parental education, and ancestry markers. Null models contain only the covariates. The PRS at p=0.05 has been standardized in the models. G=gene model; G+E=gene plus environment model; G×E=interaction model (the effect of G+E plus G×E).
ANOVA model comparison indicated that the G+E model added explanatory value to the G model for case-control status and depression severity, but not age at onset (Table 3). Both the depression PRS (odds ratio=1.578, 95% CI=1.230–2.024, corrected p=0.002) and childhood abuse (odds ratio=3.924, 95% CI=2.376–6.472, corrected p=8.120×10−4) significantly predicted case-control status. The PRS model alone explained 7.9% of the variance, and the combined model with additive effects of child abuse explained 17.9%. Addition of the interaction term did not significantly improve the model. Similarly, the depression PRS (β=0.149, SE=0.066, corrected p=0.043) and childhood abuse (β=0.494, SE=0.126, corrected p=0.002) independently significantly predicted depression severity. The depression PRS model alone explained 7.7% of the variance, and the additive model explained 13.5% of the variance. Addition of the interaction term did not significantly improve the model.
Epidemiological Cohorts
The depression PRS significantly predicted self-reported depressive symptoms at broader levels of the p threshold (Table 2), explaining up to 0.4% of variance. Using a p threshold of 0.05 to illustrate the findings in Figure 2A, a higher depression PRS was associated with greater depressive symptoms (β=0.557, SE=0.200, corrected p=0.012) (see Table 3 for model comparisons). The G+E model significantly added explanatory value to the G model for depressive symptoms (p=5.071×10−13). Both childhood abuse (β=4.935, SE=0.677, corrected p=6.080×10−6) and the depression PRS (β=0.439, SE=0.196, corrected p=0.038) significantly predicted depressive symptoms, together explaining 10.7% of the variance. The G×E model did not add explanatory value to the G+E model for depressive symptoms.
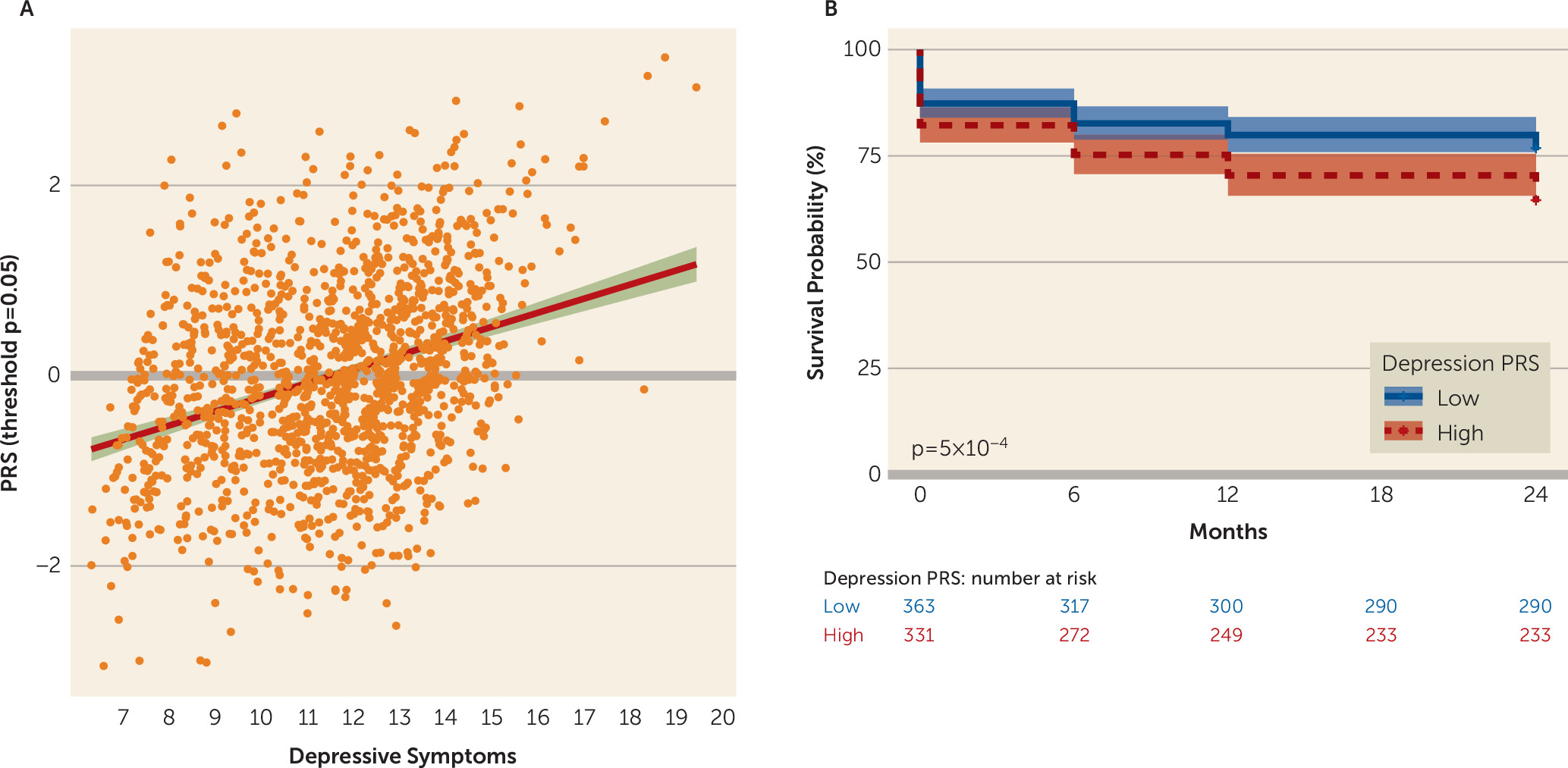
FIGURE 2. Association of the depression polygenic risk score (PRS) with depressive symptoms and survival rates in an epidemiological cohort of adolescentsa
a PRSs at a threshold of p=0.05 by depressive symptoms in the epidemiological cohort are shown in panel A. Comparisons of Kaplan-Meier survival curves for youths with low and high depression PRSs are shown in panel B. Median split was used to dichotomize the depression PRS to illustrate the findings in panel B, but the depression PRS was examined as a continuous variable in the reported analyses.
The depression PRS prospectively predicted the onset of moderate to severe levels of depressive symptoms or a clinical diagnosis of major depression (hazard ratio=1.202, 95% CI=1.045–1.383, corrected p=0.020) within the next 2 years, and those with higher depression PRSs had lower survival rates than those with lower depression PRSs (Figure 2B). The AUC summaries indicate that the probability that a participant who develops moderate to severe levels of depressive symptoms or a clinical diagnosis of major depression would have a depression PRS greater than that of a participant with mild or no depressive symptoms (probability ranging from 0.561 to 0.597 across the time points; see Figure S2 in the online supplement ). In the additive model, both the depression PRS (hazard ratio=1.171, 95% CI=1.016–1.350, corrected p=0.039) and exposure to childhood abuse (hazard ratio=2.817, 95% CI=1.963–4.043, corrected p=6.750×10−5) significantly predicted the onset of moderate to severe depressive symptoms or a clinical diagnosis of major depression. The addition of childhood abuse increased the AUC of the model to 0.628–0.631 (see Figure S2 in the online supplement ). The G×E model did not add explanatory value to the G+E model. Given the difference in prevalence of childhood exposure to abuse in the clinical and epidemiological cohorts, we examined the additive and interactive models with the Childhood Trauma Questionnaire cutoff of mild to severe, and the findings remained the same (see Table S5 in the online supplement ).
In the replication epidemiological cohort, there was a positive association between the depression PRS and parent-reported depressive symptoms at ages 8 and 11, after controlling for age, sex, and ancestry markers (Figure 3; see also Table S6 in the online supplement ). Of note, parent ratings of depressive symptoms were significantly correlated (p<0.022) at each time point. Using the Fisher combined probability test, the combined p value from these four regressions was significant (p=0.001).
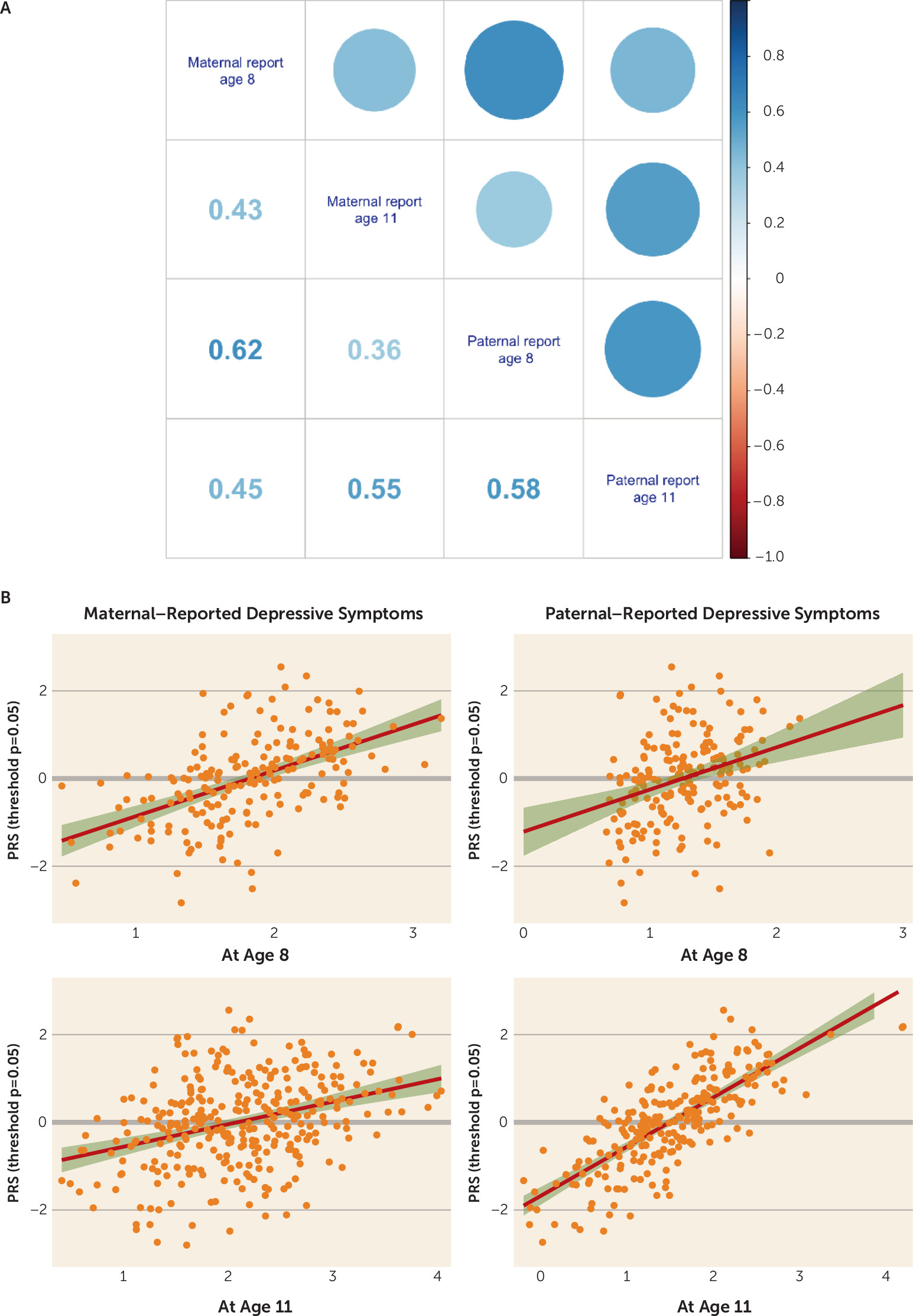
FIGURE 3. Parent-reported depressive symptoms and their association with the depression polygenic risk score (PRS) in an epidemiological cohort of childrena
a Correlations between maternal- and paternal-reported depressive symptoms are shown in panel A, and the positive associations between maternal- and paternal-reported depressive symptoms at ages 8 and 11 with the depression PRS at a threshold of p=0.05 are shown in panel B. In panel A, the correlation coefficient is depicted in the lower triangular of the correlation matrix, and a visual representation of the correlation is depicted in the upper triangular of the correlation matrix.
Discussion
This study investigated genetic liability to major depression and depressive symptoms in youths in three independent cohorts using a PRS derived from a recent GWAS of a broad phenotype of major depression and depressive symptoms among adult case and control subjects (8). This depression PRS consistently predicted clinically significant levels of depression and an earlier onset during childhood and adolescence, as well as heightened risk for the development of major depression over this critical period. The findings suggest that this depression PRS may support the identification of youths at risk for major depression prior to the emergence of clinically significant symptoms.
PRS, Major Depression, and Child and Adolescent Depression
To our knowledge, this study is the first to map a depression PRS derived from a broad phenotype of major depression in adults to clinical and epidemiological child and adolescent cohorts. We found that this depression PRS predicted childhood depression and depressive symptoms, as well as age at onset, within a child and adolescent cohort. These findings are consistent with the original study (8), in which this depression PRS was associated with early age at onset, and with the findings from the Generation Scotland cohort, which reported high genetic correlation between individuals at earlier (≤40) and later (>40) age at onset (R=0.85, 95% CI=0.66, 0.98) (28). The findings are discordant with other studies, however, including one that observed no association of depression PRS with age at onset in a Chinese cohort (29) and another that concluded that early-onset major depression was not under greater genetic control than general major depression (30). Moreover, Power and colleagues (31) described earlier-onset major depression as genetically more similar to schizophrenia and bipolar disorder than adult-onset major depression, suggesting that despite the shared genetic liability with adult-onset depression, early-onset major depression may still display genetic risk factors that are distinct from later-onset depression (31). These inconsistent results regarding the relationship of age at onset to genetic risk for major depression may be attributed to the methodological issues associated with retrospective age-at-onset assessments in the adult cohort, differences in the GWASs (8, 9) used to create the PRS, and the scarcity of studies examining the depression PRS in youths.
PRS, Major Depression, and Prediction of Future Risk
Moving beyond cross-sectional analyses, we found that this broad depression PRS prospectively predicted the onset of potentially clinically impairing depressive symptoms or a diagnosis of major depression within the next 2 years based on a reliable and valid self-report measure (the CDI) complemented with a clinical interview (the Adolescent–Longitudinal Interval Follow-Up Evaluation). Our findings also suggest that the depression PRS may serve as an indicator of depressive symptoms as early as age 8. To our knowledge, only one other study has reported on a PRS predicting disease onset using a prospective design. Specifically, the PRS of smoking quantity has been found to prospectively predict the rapid progression to heavy, persistent smoking, smoking cessation failure, and nicotine dependence in an epidemiological cohort (32). As with our findings, the association between the PRS and disease onset was small in magnitude (hazard ratio=1.544). Although it does not preclude public health relevance, low prediction accuracy does suggest that the PRS alone is not sufficient in predicting disease onset and that other factors need to be included in an optimized prediction model. One such factor examined in this study was childhood abuse, which is among the strongest predictors of childhood-onset major depression (11).
Depression PRS and Child Abuse
Our results showed that the combination of this broad depression PRS and child abuse explained 17.9% of the variance in case or control status and 13.5% in depression severity in the clinical cohort. In the epidemiological cohort, the depression PRS and child abuse explained 10.7% of the variance in depressive symptoms. Although childhood abuse (hazard ratio=2.817) significantly predicted the onset of moderate to severe depressive symptoms or major depression in the epidemiological cohort, there was little difference in the ability of the depression PRS to predict the onset of moderate to severe depressive symptoms or major depression in the epidemiological cohort when child abuse was added to the model (hazard ratio=1.202 and hazard ratio=1.171, respectively), suggesting independent, additive effects. In other words, the depression PRS may be informative when used in combination with other risk factors.
The interaction between this broad depression PRS and childhood abuse was not predictive of the clinical features of depression and did not improve the predictions over the additive model. Previous studies examining the interaction between depression PRS and early-life stress have been inconclusive (33–37). A meta-analytic study showed no evidence that the interaction of depression PRSs and childhood exposure to sexual or physical abuse predicted depression status (33). However, the most recent study, with >126,000 participants, did report a significant interaction, with higher depression PRSs among case subjects with a trauma history (childhood and adulthood trauma exposure) than case subjects with no trauma history and healthy control subjects (37). Potential explanations for these discrepant findings may lie in differences in the environmental stressor examined, the timing of the exposure, or the frequency or intensity of the exposure. Importantly, the interaction between the PRS and exposure to trauma may not predict disease directly but endophenotypes of disease (38). For instance, the schizophrenia PRS has been found to moderate the relationship between cannabis use and maturation in the cerebral cortex in male adolescents (39). The PRS for bipolar disorder has been found to interact with traumatic-event exposures to predict suicide attempts (40). Accordingly, more studies are needed to examine whether depression PRSs interact with different environmental factors or stressors to confer risk for major depression and comorbidity, possibly via effects on endophenotypes. On a similar note, the predictive power of PRSs of other psychiatric disorders (e.g., bipolar disorder or schizophrenia) and their interaction with early trauma (38) on clinically relevant depression outcomes in youths remains an important future venture. Alternatively, genetic loci not directly associated with disease status in large case-control GWASs may moderate the relationship between childhood trauma and depressive symptoms. Thus, G×E studies on environmentally reactive genes may continue to be informative, as they may represent relevant biological pathways associated with psychopathology not captured by case-control GWASs (41, 42).
Limitations
Caution is advised when interpreting our findings given the relatively small sample sizes and consequent power issues. Given the small sample size of the clinical cohort, no further investigation of the association of this broad depression PRS with relevant features of clinical depression (e.g., comparison of recurrent with first-onset depression or testing for differential diagnoses) was possible. Second, this study examined the depression PRS as a predictor of a clinical diagnosis of major depression and current depressive symptoms. Although elevated self-reported depressive symptoms are a strong predictor of future major depression (2–5), it is important to note that they are not equivalent to a diagnosis of major depression. Moreover, the measure used to assess self-reported depressive symptoms in the first epidemiological cohort covered symptoms 2 weeks prior to each assessment. Consequently, this measure would fail to capture depressive symptoms outside this time frame. To address these difficulties, the measure was complemented with a clinical interview spanning the time from the last assessment in our follow-up analyses. Importantly, given that the PRS used in the present study was derived from a GWAS using a broad phenotype in major depression, it may be that a PRS derived from a discovery sample composed only of cases with a clinician-determined diagnosis of major depression would better discriminate between a clinical diagnosis of major depression in youths and depressive symptoms in community cohorts that do not progress to a clinical diagnosis. Given the study design, we were unable to examine or control for whether depressive symptoms or childhood abuse occurred first, as well as time variations between trauma exposure and the assessment of depression or depressive symptoms in the samples. Furthermore, our measure of childhood abuse in the clinical sample did not take into account the severity of exposure to childhood abuse. Lastly, our cohorts were composed of Caucasian adolescents, and the findings may not generalize to other ethnicities.
Conclusions
PRSs derived from a broad phenotype of major depression in adults predict depression and depressive symptoms early in development. Polygenic risk may therefore be a meaningful marker of the development of clinically significant depressive symptoms in youths. However, given that this depression PRS explains a limited amount of variance in the phenotypes, the depression PRS may have the most utility in combination with other predictive variables.
Acknowledgments
The authors thank all youths and families participating in the clinical and epidemiological studies, making the present study possible; the research participants and employees of 23andMe for contributing to the meta-analysis of major depressive disorder incorporated here; and the Fuqua Family Foundation for its support of the genetics component of the Portugal Prevention of Depression Study.
Supplementary Material
File (appi.ajp.2019.18091014.ds001.pdf)
- View/Download
- 346.84 KB
References
1.
Global Burden of Disease Study 2013 Collaborators: Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015; 386:743–800
2.
Klein DN, Glenn CR, Kosty DB, et al: Predictors of first lifetime onset of major depressive disorder in young adulthood. J Abnorm Psychol 2013; 122:1–6
3.
Klein DN, Shankman SA, Lewinsohn PM, et al: Subthreshold depressive disorder in adolescents: predictors of escalation to full-syndrome depressive disorders. J Am Acad Child Adolesc Psychiatry 2009; 48:703–710
4.
Lewinsohn PM, Solomon A, Seeley JR, et al: Clinical implications of “subthreshold” depressive symptoms. J Abnorm Psychol 2000; 109:345–351
5.
McLeod GF, Horwood LJ, Fergusson DM: Adolescent depression, adult mental health and psychosocial outcomes at 30 and 35 years. Psychol Med 2016; 46:1401–1412
6.
Ahrnsbrak R, Bose J, Hedden SL, et al: Key Substance Use and Mental Health Indicators in the United States: Results From the 2016 National Survey on Drug Use and Health. Rockville, Md, Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration, 2017
7.
Smoller JW: The genetics of stress-related disorders: PTSD, depression, and anxiety disorders. Neuropsychopharmacology 2016; 41:297–319
8.
Wray NR, Ripke S, Mattheisen M, et al: Genome-wide association analyses identify 44 risk variants and refine the genetic architecture of major depression. Nat Genet 2018; 50:668–681
9.
Ripke S, Wray NR, Lewis CM, et al: A mega-analysis of genome-wide association studies for major depressive disorder. Mol Psychiatry 2013; 18:497–511
10.
Torkamani A, Wineinger NE, Topol EJ: The personal and clinical utility of polygenic risk scores. Nat Rev Genet 2018; 19:581–590
11.
Mandelli L, Petrelli C, Serretti A: The role of specific early trauma in adult depression: a meta-analysis of published literature: childhood trauma and adult depression. Eur Psychiatry 2015; 30:665–680
12.
Arnarson EO, Craighead WE: Prevention of depression among Icelandic adolescents: a 12-month follow-up. Behav Res Ther 2011; 49:170–174
13.
Strandberg TE, Järvenpää A-L, Vanhanen H, et al: Birth outcome in relation to licorice consumption during pregnancy. Am J Epidemiol 2001; 153:1085–1088
14.
Adornetto C, In-Albon T, Schneider S: Diagnostik im Kindes-und Jugendalter anhand strukturierter Interviews: Anwendung und Durchführung des Kinder-DIPS. Klinische Diagnostik und Evaluation 2008; 1:363–377
15.
Stiensmeier-Pelster J, Schürmann M, Duda K: Depressions Inventar für Kinder und Jugendliche (DIJK). Göttingen, Germany, Hogrefe, Verlag für Psychologie, 2000
16.
Hautzinger M, Keller F, Kühner C: Das Beck Depressions Inventar II: Deutsche Bearbeitung und Handbuch Zum BDI II. Frankfurt, Germany, Harcourt Test Services, 2006
17.
Adams M, Adams J: Life events, depression, and perceived problem solving alternatives in adolescents. J Child Psychol Psychiatry 1991; 32:811–820
18.
Wittchen H-U, Essau CA, Hecht H, et al: Reliability of life event assessments: test-retest reliability and fall-off effects of the Munich Interview for the Assessment of Life Events and Conditions. J Affect Disord 1989; 16:77–91
19.
Kovacs M: Children’s Depression Inventory. North Tonawanda, NY, Multi-Health Systems, 1992
20.
Marujo H: Síndromas depressivos na infância e na adolescência [Depressive syndromes in childhood and adolescence] (doctoral dissertation). Lisbon, University of Lisbon, Faculty of Psychology and Educational Sciences, 1994
21.
Smucker MR, Craighead WE, Craighead LW, et al: Normative and reliability data for the Children’s Depression Inventory. J Abnorm Child Psychol 1986; 14:25–39
22.
Bernstein DP, Fink L: Childhood Trauma Questionnaire (CTQ): A Retrospective Self-Report Manual. San Antonio, The Psychological Corporation, 1998
23.
Achenbach TM: Manual for the Child Behavior Checklist/4-18 and 1991 Profile. Burlington, Department of Psychiatry, University of Vermont, 1991
24.
Salk RH, Hyde JS, Abramson LY: Gender differences in depression in representative national samples: meta-analyses of diagnoses and symptoms. Psychol Bull 2017; 143:783–822
25.
Lewinsohn PM, Clarke GN, Seeley JR, et al: Major depression in community adolescents: age at onset, episode duration, and time to recurrence. J Am Acad Child Adolesc Psychiatry 1994; 33:809–818
26.
Goodman E, Slap GB, Huang B: The public health impact of socioeconomic status on adolescent depression and obesity. Am J Public Health 2003; 93:1844–1850
27.
Euesden J, Lewis CM, O’Reilly PF: PRSice: polygenic risk score software. Bioinformatics 2015; 31:1466–1468
28.
Fernandez-Pujals AM, Adams MJ, Thomson P, et al: Epidemiology and heritability of major depressive disorder, stratified by age of onset, sex, and illness course in Generation Scotland: Scottish Family Health Study (GS:SFHS). PLoS One 2015; 10:e0142197
29.
Docherty AR, Edwards AC, Yang F, et al: Age of onset and family history as indicators of polygenic risk for major depression. Depress Anxiety 2017; 34:446–452
30.
Guffanti G, Gameroff MJ, Warner V, et al: Heritability of major depressive and comorbid anxiety disorders in multi-generational families at high risk for depression. Am J Med Genet B Neuropsychiatr Genet 2016; 171:1072–1079
31.
Power RA, Tansey KE, Buttenschøn HN, et al: Genome-wide association for major depression through age at onset stratification: Major Depressive Disorder Working Group of the Psychiatric Genomics Consortium. Biol Psychiatry 2017; 81:325–335
32.
Belsky DW, Moffitt TE, Baker TB, et al: Polygenic risk and the developmental progression to heavy, persistent smoking and nicotine dependence: evidence from a 4-decade longitudinal study. JAMA Psychiatry 2013; 70:534–542
33.
Peyrot WJ, Van der Auwera S, Milaneschi Y, et al: Does childhood trauma moderate polygenic risk for depression? A meta-analysis of 5765 subjects from the Psychiatric Genomics Consortium. Biol Psychiatry 2017; 84:138–147
34.
Mullins N, Power RA, Fisher HL, et al: Polygenic interactions with environmental adversity in the aetiology of major depressive disorder. Psychol Med 2016; 46:759–770
35.
Musliner KL, Seifuddin F, Judy JA, et al: Polygenic risk, stressful life events and depressive symptoms in older adults: a polygenic score analysis. Psychol Med 2015; 45:1709–1720
36.
Peyrot WJ, Milaneschi Y, Abdellaoui A, et al: Effect of polygenic risk scores on depression in childhood trauma. Br J Psychiatry 2014; 205:113–119
37.
Coleman JRI, Peyrot WJ, Purves KL, et al: Genome-wide gene-environment analyses of major depressive disorder and reported lifetime traumatic experiences in UK Biobank. bioRxiv 2018;
38.
Riglin L, Hammerton G, Heron J, et al: Developmental contributions of schizophrenia risk alleles and childhood peer victimization to early-onset mental health trajectories. Am J Psychiatry 2019; 176:36–43
39.
French L, Gray C, Leonard G, et al: Early cannabis use, polygenic risk score for schizophrenia and brain maturation in adolescence. JAMA Psychiatry 2015; 72:1002–1011
40.
Wilcox HC, Fullerton JM, Glowinski AL, et al: Traumatic stress interacts with bipolar disorder genetic risk to increase risk for suicide attempts. J Am Acad Child Adolesc Psychiatry 2017; 56:1073–1080
41.
Halldorsdottir T, Binder EB: Gene × environment interactions: from molecular mechanisms to behavior. Annu Rev Psychol 2017; 68:215–241
42.
Arloth J, Bogdan R, Weber P, et al: Genetic differences in the immediate transcriptome response to stress predict risk-related brain function and psychiatric disorders. Neuron 2015; 86:1189–1202
Information & Authors
Information
Published In
History
Received: 2 September 2018
Revision received: 23 November 2018
Revision received: 22 January 2019
Accepted: 28 January 2019
Published online: 5 April 2019
Published in print: August 01, 2019
Keywords
Authors
Author Contributions
Drs. Craighead, Schulte-Körne, and Binder contributed equally to this article.
Funding Information
Dr. Halldorsdottir receives funding from European Research Council Consolidator Grant 726413. Drs. Arnarson and Craighead are board members of Hugarheill, an Icelandic company dedicated to the prevention of depression. Dr. Craighead receives book royalties from John Wiley & Sons; he has received research support from the Fuqua Family Foundation, the Mary and John Brock Foundation, and NIH; and he is a consultant to the George West Mental Health Foundation and AIM for Mental Health Foundation. Dr. Binder is a co-inventor on a patent on FKBP5, a novel target for antidepressant therapy (European patent 1687443 B1), and receives research funding from Boehringer Ingelheim for a collaboration on functional investigations of FKBP5. The other authors report no financial relationships with commercial interests.
Metrics & Citations
Metrics
Citations
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
View Options
View options
PDF/EPUB
View PDF/EPUBFigures
FIGURE 1. Depression polygenic risk score (PRS), depressive symptoms, and age at onset of depression in a clinical cohort of children and adolescentsa
aThe distribution of the depression PRS at a threshold of p=0.05 in the clinical cohort by group status (i.e., case and control subjects) is shown in panel A. Overlap between case and control subjects is indicated by the brown bars. Depression PRSs are shown at a threshold of p=0.05 by standardized scores of depression severity (panel B) and by age at onset in the clinical cohort (panel C). The PRS at a threshold of p=0.05 has been standardized in the models, and the shading represents 95% confidence intervals.
FIGURE 2. Association of the depression polygenic risk score (PRS) with depressive symptoms and survival rates in an epidemiological cohort of adolescentsa
a PRSs at a threshold of p=0.05 by depressive symptoms in the epidemiological cohort are shown in panel A. Comparisons of Kaplan-Meier survival curves for youths with low and high depression PRSs are shown in panel B. Median split was used to dichotomize the depression PRS to illustrate the findings in panel B, but the depression PRS was examined as a continuous variable in the reported analyses.
FIGURE 3. Parent-reported depressive symptoms and their association with the depression polygenic risk score (PRS) in an epidemiological cohort of childrena
a Correlations between maternal- and paternal-reported depressive symptoms are shown in panel A, and the positive associations between maternal- and paternal-reported depressive symptoms at ages 8 and 11 with the depression PRS at a threshold of p=0.05 are shown in panel B. In panel A, the correlation coefficient is depicted in the lower triangular of the correlation matrix, and a visual representation of the correlation is depicted in the upper triangular of the correlation matrix.
Tables
Media
References
References
1.
Global Burden of Disease Study 2013 Collaborators: Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015; 386:743–800
2.
Klein DN, Glenn CR, Kosty DB, et al: Predictors of first lifetime onset of major depressive disorder in young adulthood. J Abnorm Psychol 2013; 122:1–6
3.
Klein DN, Shankman SA, Lewinsohn PM, et al: Subthreshold depressive disorder in adolescents: predictors of escalation to full-syndrome depressive disorders. J Am Acad Child Adolesc Psychiatry 2009; 48:703–710
4.
Lewinsohn PM, Solomon A, Seeley JR, et al: Clinical implications of “subthreshold” depressive symptoms. J Abnorm Psychol 2000; 109:345–351
5.
McLeod GF, Horwood LJ, Fergusson DM: Adolescent depression, adult mental health and psychosocial outcomes at 30 and 35 years. Psychol Med 2016; 46:1401–1412
6.
Ahrnsbrak R, Bose J, Hedden SL, et al: Key Substance Use and Mental Health Indicators in the United States: Results From the 2016 National Survey on Drug Use and Health. Rockville, Md, Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration, 2017
7.
Smoller JW: The genetics of stress-related disorders: PTSD, depression, and anxiety disorders. Neuropsychopharmacology 2016; 41:297–319
8.
Wray NR, Ripke S, Mattheisen M, et al: Genome-wide association analyses identify 44 risk variants and refine the genetic architecture of major depression. Nat Genet 2018; 50:668–681
9.
Ripke S, Wray NR, Lewis CM, et al: A mega-analysis of genome-wide association studies for major depressive disorder. Mol Psychiatry 2013; 18:497–511
10.
Torkamani A, Wineinger NE, Topol EJ: The personal and clinical utility of polygenic risk scores. Nat Rev Genet 2018; 19:581–590
11.
Mandelli L, Petrelli C, Serretti A: The role of specific early trauma in adult depression: a meta-analysis of published literature: childhood trauma and adult depression. Eur Psychiatry 2015; 30:665–680
12.
Arnarson EO, Craighead WE: Prevention of depression among Icelandic adolescents: a 12-month follow-up. Behav Res Ther 2011; 49:170–174
13.
Strandberg TE, Järvenpää A-L, Vanhanen H, et al: Birth outcome in relation to licorice consumption during pregnancy. Am J Epidemiol 2001; 153:1085–1088
14.
Adornetto C, In-Albon T, Schneider S: Diagnostik im Kindes-und Jugendalter anhand strukturierter Interviews: Anwendung und Durchführung des Kinder-DIPS. Klinische Diagnostik und Evaluation 2008; 1:363–377
15.
Stiensmeier-Pelster J, Schürmann M, Duda K: Depressions Inventar für Kinder und Jugendliche (DIJK). Göttingen, Germany, Hogrefe, Verlag für Psychologie, 2000
16.
Hautzinger M, Keller F, Kühner C: Das Beck Depressions Inventar II: Deutsche Bearbeitung und Handbuch Zum BDI II. Frankfurt, Germany, Harcourt Test Services, 2006
17.
Adams M, Adams J: Life events, depression, and perceived problem solving alternatives in adolescents. J Child Psychol Psychiatry 1991; 32:811–820
18.
Wittchen H-U, Essau CA, Hecht H, et al: Reliability of life event assessments: test-retest reliability and fall-off effects of the Munich Interview for the Assessment of Life Events and Conditions. J Affect Disord 1989; 16:77–91
19.
Kovacs M: Children’s Depression Inventory. North Tonawanda, NY, Multi-Health Systems, 1992
20.
Marujo H: Síndromas depressivos na infância e na adolescência [Depressive syndromes in childhood and adolescence] (doctoral dissertation). Lisbon, University of Lisbon, Faculty of Psychology and Educational Sciences, 1994
21.
Smucker MR, Craighead WE, Craighead LW, et al: Normative and reliability data for the Children’s Depression Inventory. J Abnorm Child Psychol 1986; 14:25–39
22.
Bernstein DP, Fink L: Childhood Trauma Questionnaire (CTQ): A Retrospective Self-Report Manual. San Antonio, The Psychological Corporation, 1998
23.
Achenbach TM: Manual for the Child Behavior Checklist/4-18 and 1991 Profile. Burlington, Department of Psychiatry, University of Vermont, 1991
24.
Salk RH, Hyde JS, Abramson LY: Gender differences in depression in representative national samples: meta-analyses of diagnoses and symptoms. Psychol Bull 2017; 143:783–822
25.
Lewinsohn PM, Clarke GN, Seeley JR, et al: Major depression in community adolescents: age at onset, episode duration, and time to recurrence. J Am Acad Child Adolesc Psychiatry 1994; 33:809–818
26.
Goodman E, Slap GB, Huang B: The public health impact of socioeconomic status on adolescent depression and obesity. Am J Public Health 2003; 93:1844–1850
27.
Euesden J, Lewis CM, O’Reilly PF: PRSice: polygenic risk score software. Bioinformatics 2015; 31:1466–1468
28.
Fernandez-Pujals AM, Adams MJ, Thomson P, et al: Epidemiology and heritability of major depressive disorder, stratified by age of onset, sex, and illness course in Generation Scotland: Scottish Family Health Study (GS:SFHS). PLoS One 2015; 10:e0142197
29.
Docherty AR, Edwards AC, Yang F, et al: Age of onset and family history as indicators of polygenic risk for major depression. Depress Anxiety 2017; 34:446–452
30.
Guffanti G, Gameroff MJ, Warner V, et al: Heritability of major depressive and comorbid anxiety disorders in multi-generational families at high risk for depression. Am J Med Genet B Neuropsychiatr Genet 2016; 171:1072–1079
31.
Power RA, Tansey KE, Buttenschøn HN, et al: Genome-wide association for major depression through age at onset stratification: Major Depressive Disorder Working Group of the Psychiatric Genomics Consortium. Biol Psychiatry 2017; 81:325–335
32.
Belsky DW, Moffitt TE, Baker TB, et al: Polygenic risk and the developmental progression to heavy, persistent smoking and nicotine dependence: evidence from a 4-decade longitudinal study. JAMA Psychiatry 2013; 70:534–542
33.
Peyrot WJ, Van der Auwera S, Milaneschi Y, et al: Does childhood trauma moderate polygenic risk for depression? A meta-analysis of 5765 subjects from the Psychiatric Genomics Consortium. Biol Psychiatry 2017; 84:138–147
34.
Mullins N, Power RA, Fisher HL, et al: Polygenic interactions with environmental adversity in the aetiology of major depressive disorder. Psychol Med 2016; 46:759–770
35.
Musliner KL, Seifuddin F, Judy JA, et al: Polygenic risk, stressful life events and depressive symptoms in older adults: a polygenic score analysis. Psychol Med 2015; 45:1709–1720
36.
Peyrot WJ, Milaneschi Y, Abdellaoui A, et al: Effect of polygenic risk scores on depression in childhood trauma. Br J Psychiatry 2014; 205:113–119
37.
Coleman JRI, Peyrot WJ, Purves KL, et al: Genome-wide gene-environment analyses of major depressive disorder and reported lifetime traumatic experiences in UK Biobank. bioRxiv 2018;
38.
Riglin L, Hammerton G, Heron J, et al: Developmental contributions of schizophrenia risk alleles and childhood peer victimization to early-onset mental health trajectories. Am J Psychiatry 2019; 176:36–43
39.
French L, Gray C, Leonard G, et al: Early cannabis use, polygenic risk score for schizophrenia and brain maturation in adolescence. JAMA Psychiatry 2015; 72:1002–1011
40.
Wilcox HC, Fullerton JM, Glowinski AL, et al: Traumatic stress interacts with bipolar disorder genetic risk to increase risk for suicide attempts. J Am Acad Child Adolesc Psychiatry 2017; 56:1073–1080
41.
Halldorsdottir T, Binder EB: Gene × environment interactions: from molecular mechanisms to behavior. Annu Rev Psychol 2017; 68:215–241
42.
Arloth J, Bogdan R, Weber P, et al: Genetic differences in the immediate transcriptome response to stress predict risk-related brain function and psychiatric disorders. Neuron 2015; 86:1189–1202