The neurobehavioral effects of closed head injury (CHI) in young adults include alterations in cognition, mood, and social functioning that reduce the quality of life for both the patient and significant others.
1–7 These changes often disrupt rehabilitation efforts, return to work, and family relationships.
4,5,8,9 Significant others find the emotional and cognitive sequelae such as slowness, irritability, and memory deficit more stressful than the physical symptoms.
8,10 Early research by Oddy et al.
7 reported that relatives of severely injured patients who were 6 months postinjury described changes in the patients encompassing poor memory and concentration, as well as impatience and irritability. Many of these symptoms were present 7 years later.
11 More recent studies have also confirmed the high incidence of behavioral and cognitive changes after CHI. Dikmen et al.
12 had survivors of moderate to severe CHI rate their functioning at 1 month, 1 year, and 2 years postinjury. At 1 month, the greatest problems concerned fatigue, memory disturbance, dizziness, and concentration. Memory problems and irritability persisted at 1 and 2 years. Schalén et al.
13 examined survivors of severe CHI who had good recoveries or moderate disabilities on the Glasgow Outcome Scale.
14 At 5 to 8 years postinjury, relatives reported symptoms in the patients that included hostile feelings, poor memory, and fatigue.
These previous studies have characterized the outcome of predominantly young survivors of head injury. As a result, little is known about the neurobehavioral sequelae and their pattern of recovery in older patients who are in their fifth decade and beyond. Although the incidence of head injury is highest in persons 18 to 30 years of age, epidemiological studies reveal that head injury also poses a significant problem for older persons.
15–17 Moreover, studies in young adults have tended to focus on patients with severe CHI. Although mortality following CHI rises with age,
18,19 a number of older adults with mild and moderate injuries may survive and thus require postacute rehabilitation and ongoing family supervision. Thus, it is important to examine whether a similar pattern of behavioral changes is found in this older at-risk population.
In an earlier review of the neurobehavioral sequelae in older CHI patients,
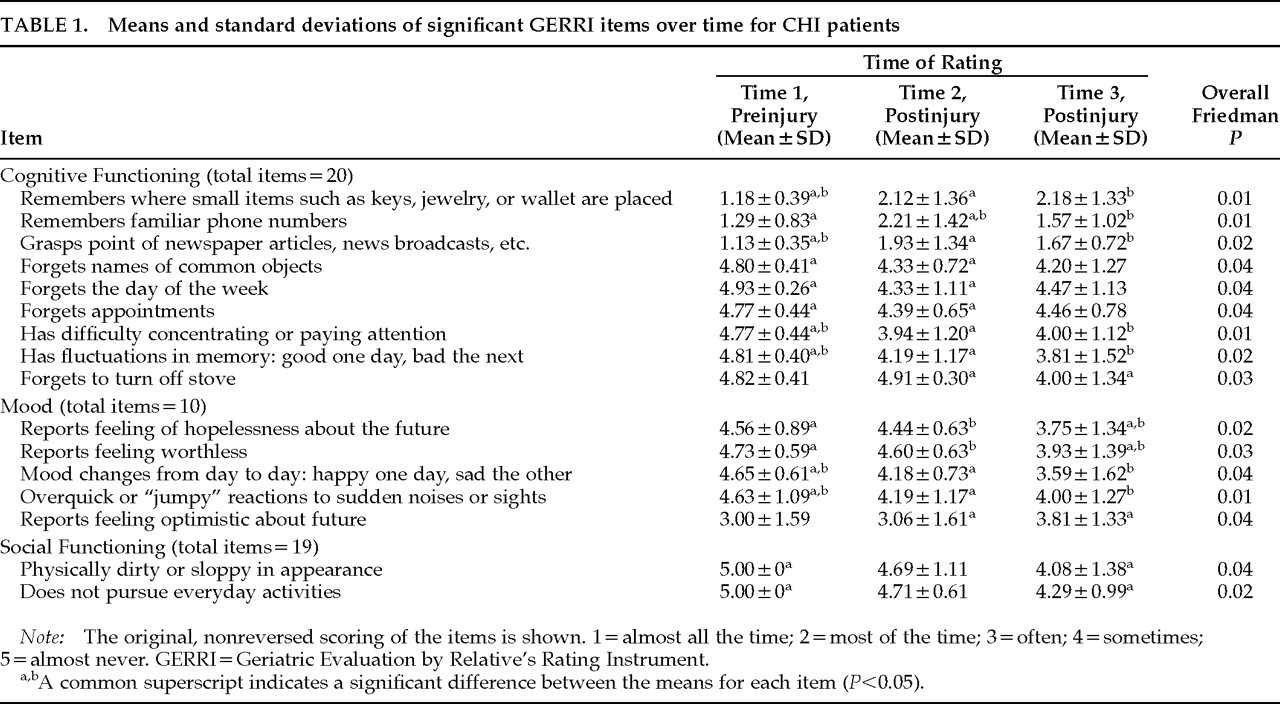
20 we described the findings regarding the cognitive and behavioral changes reported by significant others of 13 patients ≥50 years old who were in the initial 5 months of recovery following mild and moderate CHI. Significant others completed the Geriatric Evaluation by Relative's Rating Instrument (GERRI).
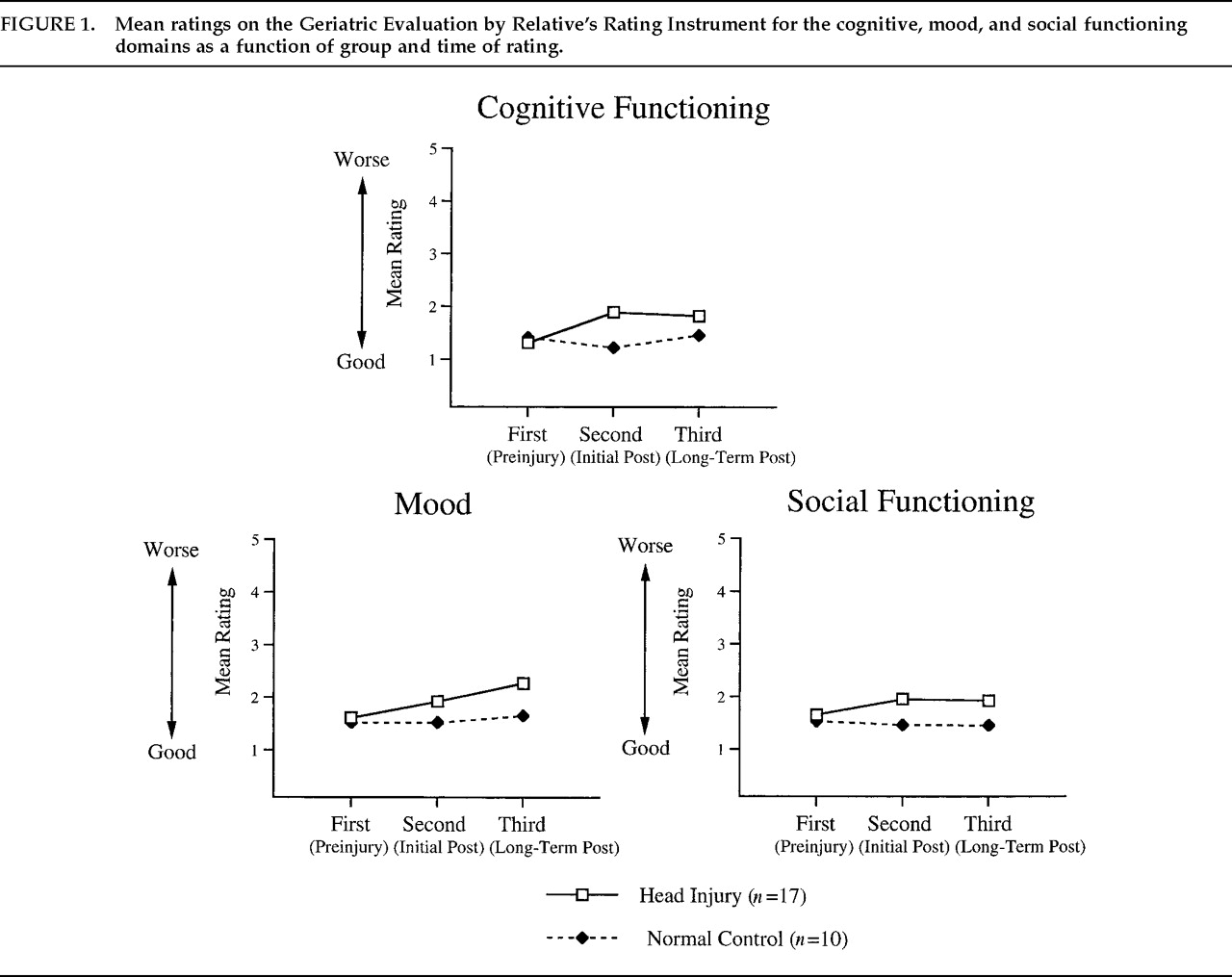
21 Compared with their preinjury status, patients were rated as exhibiting significant declines in cognition, mood, and social functioning. The most salient changes included decreased memory, comprehension, and concentration as well as increased restlessness and irritability. In the current study, long-term follow-up to 2 years postinjury is described. We hypothesized that compared with a demographically similar group of control subjects without head injuries, the patients with mild and moderate CHI would still show significant postinjury impairments in cognition, mood, and social functioning.
METHODS
Subjects
The sample included 17 CHI patients (mean age=69.9 yr, SD=11.5; mean education=11.7 yr, SD=3.8). They were prospectively recruited from acute care neurosurgery services of hospitals affiliated with Emory University School of Medicine in Atlanta and the University of Maryland School of Medicine in Baltimore. To be included in the study, patients had to have ratings made at three time periods (preinjury and two follow-up occasions). Five patients sustained mild head injuries, defined as Glasgow Coma Scale (GCS)
22 scores of 13–15 with loss of consciousness lasting less than 20 minutes and normal neurologic and neuroradiologic findings on computed tomography (CT) or magnetic resonance imaging. The remaining 12 patients sustained moderate injuries, classified as GCS scores of 9–12, or 13–15 if there was evidence on CT of focal neurologic deficits or brain lesions (contusions, hematomas). The primary mechanism of injury was motor vehicle accidents (
n=11), 5 patients were injured in falls, and 1 patient was a pedestrian injured in a street accident. All of the patients were functioning independently at the time of their accidents, and none resided in personal care or nursing homes.
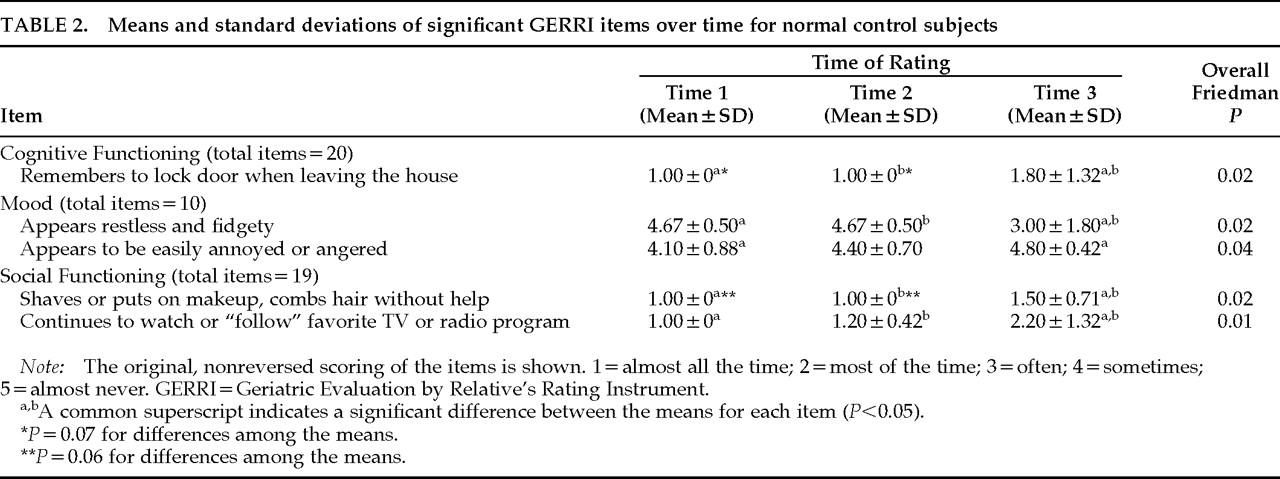
A comparison group of 10 community-residing control subjects (mean age=74.7 yr, SD=10.6; mean education=13.4 yr, SD=2.1) was recruited. There were no significant differences (P>0.05) between the patient and control groups in age, education, or distribution of gender.
Patients and control subjects did not have premorbid histories of drug or alcohol abuse, psychiatric disturbance, or neurologic illness including significant head injury. In addition, both the patients and the control subjects were free of preexisting dementia as assessed by family ratings on the Blessed Dementia Rating Scale,
23 a questionnaire that inquires about changes in cognition, personality, and activities of daily living within the past 6 months. The scores were within normal limits for both groups (range 0–3.5 for patients, 0–2 for control subjects). The procedures were explained to all subjects prior to their participation, and informed consent was obtained by using protocols approved by the Human Investigations Committees of the participating centers.
Instrument
The Geriatric Evaluation by Relative's Rating Instrument was developed by Schwartz
21 to measure cognitive and behavioral changes in community-residing outpatients in their fifth decade of life or older. The GERRI is completed by a significant other and contains 49 items, which are scaled from 1 (almost all the time) to 5 (almost never). In addition, a rating of 6 (does not apply) is given if the behavior is never performed (e.g., pays bills with checks). Specific items on the GERRI are combined to yield domains measuring cognition (20 items), mood (10 items), and social functioning (19 items). In a sample of patients with Alzheimer's disease, Schwartz
21 found that the GERRI had high interrater reliability and validity in discriminating patients with mild, moderate, and severe dementia.
Procedures
The GERRI was completed by a significant other on three different occasions. Initially, the significant other was asked to rate the patient's preinjury behaviors in terms of their frequency of occurrence. The average time from injury to the preinjury GERRI rating was 40 days (SD=35.1). The questionnaire was then mailed to the same informant an average of 123 days postinjury (SD=71.3) and later at an average of 390 days (SD=88.5) postinjury. The informant was asked on these two follow-up occasions to provide ratings based on the patient's current functioning. Of 22 patients who had a preinjury and an initial follow-up GERRI, 17 (77%) also had a GERRI available at the last postinjury occasion. None of the patients were in the hospital at the time of their follow-up ratings.
A significant other for each control subject completed the GERRI based on the subject's current functioning. The GERRI was then mailed to the significant other at two follow-up intervals. The number of days separating the first and second ratings (mean±SD: 70.8±69.7 for patients, 32.7±22.9 for control subjects) and second and third ratings (240.2±81.5 for patients, 215.7±52.8 for control subjects) was comparable between the two groups, P>0.05.
DISCUSSION
The results of this study indicate that older adults sustaining mild and moderate CHI show cognitive and behavioral changes, according to their significant others, that are similar to those seen in young adults following more severe head injury.
7,8,10,11,13 Most of these sequelae encompass cognitive difficulties that we have previously documented via significant others' reports in the initial 5 months of recovery as well as objective neuropsychological evaluations in this older group.
20,24 Changes in mood were also noted, including feelings of hopelessness and worthlessness. Other investigators
2,4–6,25 have observed that these alterations in young survivors lead to considerable family stress and disruption of relationships. Although subjective burden was not measured in the current study, it is likely that similar stresses are found in the significant others of these older patients and that these stresses, in turn, affect their perceptions of the patients' functioning on the three GERRI domains.
Analysis of the specific items on the GERRI revealed different patterns of temporal onset in the patient group for the domains of cognition, mood, and social functioning. Extension of our previous study using the GERRI
20 to a longer follow-up period indicated that some changes were not initially appreciated by significant others. Whereas many of the changes in cognition were rated as immediately noticeable after the injury, some of the mood and social functioning changes were not apparent until the last postinjury rating. In addition, feelings of hopelessness and worthlessness as well as lack of optimism about the future were rated as worsening from the initial to the longer postinjury follow-ups. This trend suggests that depression may have a delayed onset in this population, similar to findings in young survivors.
26,27 Alternatively, the relatives' own levels of depression may increase over time, and this in turn may affect their ratings of the patient's mood. Further distinction of these two possibilities would require independent and objective evaluation of the patients' and control subjects' moods and the way in which these correlate with the GERRI ratings. A finding via independent ratings that patients' moods worsened over time would underscore the importance of assessing depression at several points in recovery following CHI in order to detect associations that may not be immediately apparent. Studies in young CHI patients demonstrate that depression is associated with poor cognitive recovery, diminished social relationships, and reduced quality of life.
28–30 In our own work,
31 we have documented a high frequency of depression, approximately 30%, in older adults on the basis of a self-report inventory (Geriatric Depression Scale
32). In addition, higher scores on the Geriatric Depression Scale, indicative of greater depression, predict attentional and memory functioning an average of 7 and 13 months postinjury, but not at the initial 1-month assessment.
33The postinjury changes reported by the significant others of the CHI patients were actually quite mild when compared with estimates of the patients' preinjury status. Although there were clear alterations in functioning following the head injury, an inspection of the mean values indicated that significant others noted rather slight repercussions. Moreover, with the exception of the cognitive domain score, the patients were not rated as being significantly more impaired than the control subjects, even though there were significant changes over time in the overall scores of the patients. The lack of more pronounced changes could be related to our inclusion of patients with mild/moderate as opposed to severe injuries. As we noted above, most studies in young adults have focused on relatives' ratings of patients with severe CHI. In addition, our patients were carefully screened for preexisting major health problems, depression, and cognitive impairments, and thus they comprised a rather well-functioning group prior to their injuries. Finally, the GERRI ratings, as with any self-report measures, depend on the accuracy of the informants. In a sample of patients with head injuries or orthopedic injuries sustained 5 to 10 years previously, we found that relatives tended to underestimate the extent of the patients' current cognitive problems when compared with objective evaluation of these patients.
34 The significant others in the current study may likewise have minimized the extent of alterations in patient functioning.
On a methodological note, our findings highlight the importance of including a control group for comparison with a head-injured sample. Item analyses indicated that variations in functioning over time were also reported for the control subjects, although the specific GERRI items differed between the groups. In a study of subjective complaints after mild head injury, Dikmen et al.
35 found that control subjects without head injury reported a considerable number of physical and behavioral symptoms. These trends, also noted in other research, suggest that a failure to incorporate non–head-injured control subjects may provide an inaccurate assessment of initial outcome and recovery.
In summary, the results of this study reveal parallels between the types of neurobehavioral changes reported by significant others of older adults and the findings in outcome from more severe CHI in young persons. Although our sample is not representative of all older adults sustaining CHI, our findings do paint a more positive picture as opposed to the generally pessimistic portrayal in the literature.
36 Future studies should examine the impact of these alterations of older adults' capacity for independent functioning. In addition, assessment of the impact of these alterations on caregiver stress and burden should be investigated to identify possible supportive needs and interventions.