Subjects
The average age of the 11 Lyme disease patients was 44.2 years (SD 12.4; range 19–63). The duration of symptoms was 59.5 months (SD 57.5; range 6–170), and the length of time since diagnosis was 18.9 months (SD 17.1; range 2–60). The duration of prior oral antibiotic treatment was 7.9 months (SD 7.3; range 0–19), and the duration of prior IV antibiotic treatment was 2.0 months (SD 1.1; range 1–4). The symptom history since the onset of Lyme disease included the following: memory loss (11/11), excessive fatigue (11/11), sleep disturbance (11/11), arthralgias (11/11), word-finding problems (10/11), headaches (9/11), radiculopathy (8/11), irritability and mood lability (8/11), recalled tick bite (5/11), physician diagnosed erythema migrans (4/11), and arthritis (4/11). Five of the 11 patients had had prior spinal taps, with 3 of the 5 revealing abnormal CSF results (2 ELISA positive for Borrelia burgdorferi and 1 with elevated protein). Eight of the 11 had had prior MRI scans, 4 of whom had abnormal results (one or more white matter hyperintensities).
Controls and patients had similar mean age, sex distribution, blood hemoglobin, pulse, and end-tidal pCO
2 concentration. The controls differed from patients only in their systolic blood pressure, with both groups in a normal range. (
Table 1). Exploratory correlational and covariance analyses were completed using the systolic blood pressure variable, but it was inconsistently related to blood flow measures and did not appear to exert any influence on group rCBF differences.
Regional Cerebral Blood Flow. Patients' and controls' mean flows for three rCBF parameters (ISI, fg, or k
2) did not differ significantly, but significant differences in mean flow for the wg ratio were observed (
Table 1). A higher wg suggests an imbalance between fast and slow clearing flows that requires further investigation. Detector-by-detector analyses were then carried out for each of the four rCBF parameters.
For the ISI measure, no effect was found for disease status alone (F[1,31] < .001, p=.999), which is consistent with the global CBF findings. However, a significant three-way interaction was found for disease status in hemisphere by detector site (F[15,465]=1.79, p=.033), indicating that patients and controls differed at specific detectors within an identifiable hemisphere. Analysis of individual normalized detector values (ISI parameter) revealed that patients and controls differed significantly at only two sites in the left hemisphere. Patients had lower relative CBF at one anterior, dorsolateral detector (F2: t[31]=2.11, p=.043), and higher relative CBF at the most posterior detector in the occipital lobe (O2: t[31]=−2.97, p=.006). This finding must be viewed with an awareness that, at an alpha level of .05, two of 32 detectors might differ by chance.
A similar omnibus analysis of the fg data produced no significant differences related to disease status in the overall MANOVA (for disease status: F[1,31] < .001, p=.999; for disease status by detector: F[15,465]=1.40, p=.141; for disease status by hemisphere: F[1,31]=.37, p=.550; for disease status by detector by hemisphere: F[15,465]=1.05, p=.403).
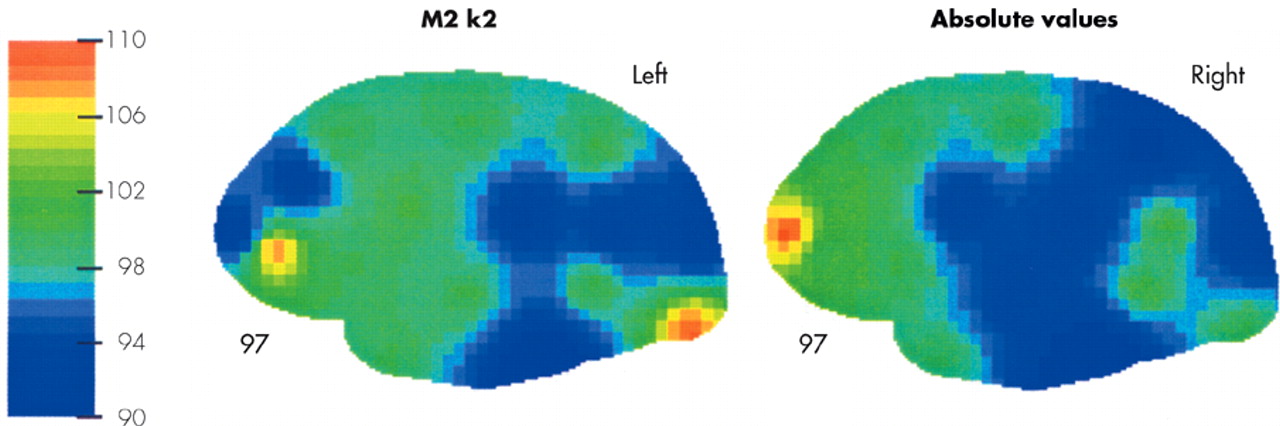
Analysis of the k2 data, on the other hand, produced a significant disease status by detector interaction (
F[15,465]=2.30,
p=.004), indicating that patients differed from controls at specific detector sites bilaterally. In the analysis of the individual detector sites, patients showed higher relative white matter CBF at a number of frontal detectors (F1 on the right:
t[31]=−2.17,
p=.038; F3 on the left:
t[31]=−2.41,
p=.022); and one occipital detector (O2 on the left:
t[31]=−2.43,
p=.021). They had consistently lower CBF at posterior temporal and parietal detectors (P4 on right:
t[31]=2.12,
p=.042 and T3 on the left:
t[31]=2.59,
p=.015). Overall, this measure of white matter CBF was consistently lower in posterior temporal and parietal regions on both sides of the patients' brain. If relative flows were averaged in these regions (T3, P1, P2, P3, P4), patients had lower flows both bilaterally (
t[31]=3.20,
p=.003) and on each side of the brain individually (right:
t[31]=2.20,
p=.035; left:
t[31]=4.15,
p < .001). Thus, in the patients' cortex there appear to be broad regions in which white matter CBF was reduced. Patient/control differences in k
2 are illustrated pictorially in
Figure 1.
The reduction in slow-clearing flow among the patients was confirmed in the analysis of the wg ratio at individual detector sites, where there was a main effect for disease status in the overall MANOVA (F[1,31]=5.08, p= .031). Significant patient/control differences (all t[31] > 2.04, p < .05) are found at 19 of the 32 detector sites (F1, F2, F3, F4, C1, C2, P1, P2, P3, P4 on right, F1, F3, C1, C2, T1, T3, P1, P2, P3 on left). All are in the direction of patients having a higher wg.
Flow deficits do not appear to be a reflection of the small white matter hyperintensities that were observed in some subjects on MRI, since a comparison of those with (
n=4) and without (
n=4) hyperintensities revealed no differences. Overall, higher wg in patients appears to reflect a reduction in slow-clearing flows, since there was no evidence of any elevation in fast-clearing flows at any detector site. Normalized values of k
2 appear higher in anterior regions, but this appears to be an artifact of the normalization procedure: when large areas of cortex are poorly perfused (e.g., posterior regions in patients), relative flow to other areas—as a percent of the total—will be elevated.
27Neuropsychological Findings
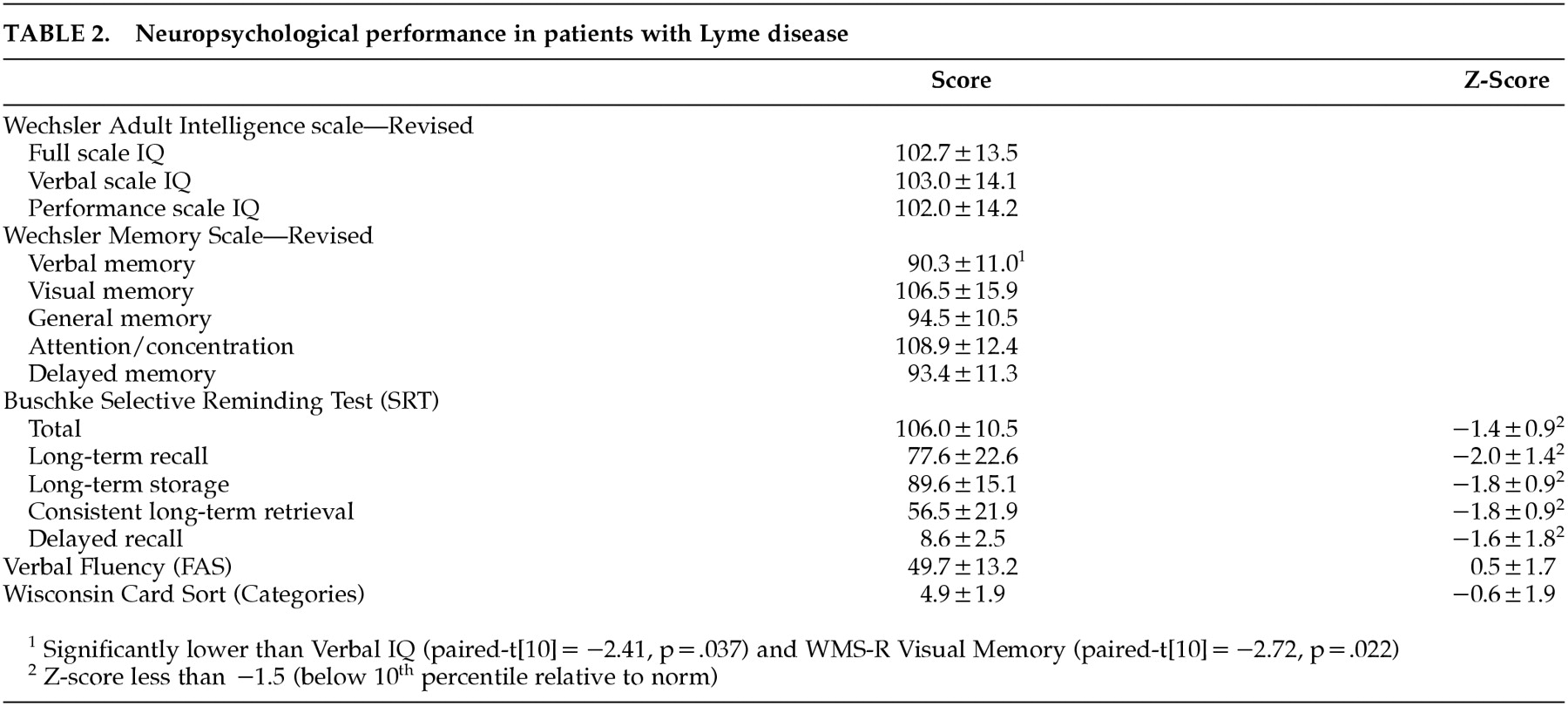
On the WAIS-R, the Lyme patients' IQs fell within a normal range and were generally consistent (
Table 2). Clinically significant reductions in verbal memory were noted, on both the WMS-R and the Buschke Selective Reminding Test. For the group as a whole, both Verbal Fluency and Wisconsin Card Sort performance were within normal limits.
On the Beck Depression Inventory, the mean of 16.4 (SD 12.8) placed the Lyme patients in the “mild depression” severity category. Although the majority of patients had scores consistent with either “none” or “mild” depression (7/11), two cases had borderline-moderate depression, and two had more severe depressive scores. On the Zung Anxiety Index, the mean of 55.6 (SD 11.3) was consistent with moderate anxiety for the group as a whole. Two patients had scores indicative of no anxiety, five had scores indicative of minimal to moderate anxiety, and four had scores consistent with marked to severe anxiety.
In the analysis of neuropsychological performance and rCBF, both the Buschke Total score and the Consistent Long Term Retrieval Score, were correlated with mean flow for k
2 (
r=.66,
p=.027 for Total;
r=.68,
p=.022 for CLTR). In other words, improved cognitive performance was associated with improved white matter flow. This flow measure was also correlated with the degree of reduction in WAIS-R Block Design relative to Vocabulary score (
r=.62,
p=.041). Correlations with the averaged bilateral posterior temporal/parietal flow were similar but did not reach significance. The reduction in WAIS-R Digit Symbol was, however, significantly correlated with this k
2 measure on the left side (
r=.63,
p=.037). Consistent associations were not observed with the wg measure. However, a trend-level negative association was noted between rCBF parameters and indices of premorbid intellectual functioning, and lower global flows were associated with higher estimates of premorbid intelligence (e.g., ISI mean flow and Verbal IQ,
r=−.58,
p=.062) and a tendency toward higher levels of education (
r=−.45,
p=.163). Both factors would attenuate the expression of neuropsychological deficits.
28 With a sample this small, there is inadequate power to statistically control for their effects on performance across an entire battery.
Tests scores that correlated with mean flow for k2 were not associated with either Beck or Zung scores, and neither the mean flow for k2 nor the average flow to temporal and parietal regions was correlated with the Beck or Zung scores. If the Beck and Zung scores are partialled out of the association between test scores and rCBF, significant correlations are essentially unchanged. With both Beck and Zung scores partialled out, the Buschke total score is correlated with k2 mean flow (rpartial=.68, p=.042); Block Design deviation from Vocabulary is correlated with k2 mean flow (rpartial=.70, p=.036); and Digit Symbol deviation from Vocabulary is correlated with left-sided temporal-parietal flow (rpartial=.67, p=.048). Depression and anxiety do not appear to mediate the association between test scores and flow measures.