Among the illicit stimulants, cocaine and the amphetamines are the most widely abused. While cocaine use has had a national distribution and an overall decrease since the early 1990s, the use of amphetamines, particularly methamphetamine, has been increasing and spreading eastward from its endemic centers in the western and southwestern parts of the United States.
1–3 The use and effects of methamphetamine command increasing attention from researchers and drug treatment professionals, as well as from drug enforcement officials and state and national legislators. Using the University of California's MELVYL MEDLINE database, a search for journal articles indexed under “methamphetamine” reveals a doubling of the number of articles from the year 1990 through the year 2000. One hundred six articles are indexed for 1990, whereas 212 articles are found for 2000. In contrast, the number of articles indexed under “cocaine” remained essentially constant over the same time period, at approximately 1,000 per year. From 1994 to 2000, the number of underground methamphetamine labs that were seized by the U.S. Drug Enforcement Agency (DEA) increased 590%, with 6,394 lab seizures reported.
4 Similarly, the amount of the drug seized by the DEA also increased, from 289 kg in 1996 to 3,163 kg in 2000.
4,5 Several acts of national legislation, such as the Comprehensive Methamphetamine Control Act of 1996 and the Methamphetamine and Club Drug Anti-Proliferation Act of 2000, have focused specifically on the growing problem of methamphetamine abuse. This article provides an overview of some of the relevant clinical and historical features of methamphetamine abuse, followed by a discussion of the drug's effect on different neurotransmitter systems. Particular attention is given to the issue of methamphetamine-induced neurotoxicity. Lastly, the effects of methamphetamine on cognition are also assessed, with particular reference to neurotoxic effects.
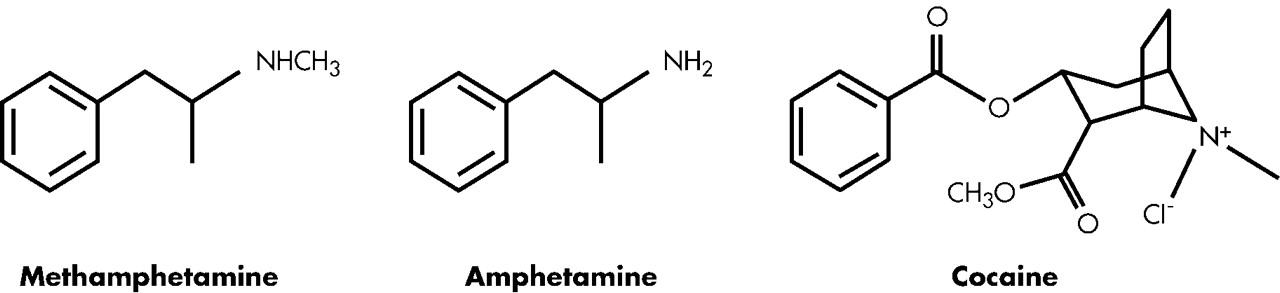
Unlike cocaine, methamphetamine is a synthetically derived drug, and its synthesis requires only rudimentary laboratory equipment (See
Figure 1). Until the enactment of recent legislation, the requisite reagents used to make methamphetamine could be purchased in drugstores, hardware stores, and chemical supply houses. According to the DEA, among the controlled substances manufactured underground in the United States, methamphetamine is the most prevalent, and it is one of the commonly abused controlled substances that can be made in the home.
6 For many years, methamphetamine has been manufactured in small “mom-and-pop” labs that can be readily concealed in a shed, storage garage, or large vehicle such as a minivan. Prior to the late 1980s, illicit manufacture of methamphetamine was the purview of white motorcycle gangs who used the chemical phenyl-2-propanone (P2P) to make the drug, which was legal at the time, as the major precursor. Federal controls were placed on P2P with the implementation of the Federal Chemical Diversion and Trafficking Act of 1988. Subsequently, underground chemists began using ephedrine and pseudoephedrine as the main precursors in methamphetamine synthesis. The use of ephedrine and pseudoephedrine is simpler and more efficient than the P2P-based process, as it produces a higher yield of the psychoactive D-isomer of the drug. Additionally, Mexican poly-drug trafficking organizations began manufacturing and distributing methamphetamine in the mid-1990s. These organizations created “superlabs” in Mexico and southern California that were capable of producing 10 pounds or more of high-purity methamphetamine in 1 to 2 days. The superlabs are in marked contrast to the more numerous and widely distributed mom-and-pop labs, which maintain a share of the U.S. market. Because of the varied manufacturing patterns, the purity of street methamphetamine can vary widely, even within a circumscribed geographic area.
3Methamphetamine is typically ingested (usually dissolved in a beverage, such as a soft drink or coffee), smoked (vaporized), snorted, or injected intravenously. The amount used at a single administration can vary more than tenfold, depending on individual tolerance, route of administration, and purity. Among chronic users, dosing patterns tend to be either administrations of low doses or cycles of high-dose bingeing that lasts for days, followed by a period of abstinence.
Amphetamines have a longer duration of action than cocaine (8–13 hours versus 1–3 hours) and may be more rapidly addicting.
7 Methamphetamine has higher lipid solubility than the unsubstituted amphetamine, and thus larger amounts of the drug rapidly and efficiently cross the blood-brain barrier. Approximately 45% of a methamphetamine dose is metabolized into amphetamine, and both drugs are primarily excreted renally.
8 In animal models the pharmacological effects of methamphetamine depend greatly upon the dose and pattern of administration. In rat models, for instance, different effects are seen with administration of a single dose, repeated administration of low doses at long intervals, repeated administration of high doses at short intervals, or high-dose runs superimposed on chronic low-dose administration.
9 In methamphetamine-naïve humans, low doses produce a sense of heightened alertness, attentiveness, and energy. Higher dose intoxication produces a sense of well-being, euphoria, and enhanced self-esteem that can approach hypomania and grandiosity. Initially, sexual activity and pleasure may be increased, although longer use is associated with impaired sexual functioning. Appetite is suppressed. Adverse effects include restlessness, insomnia, bruxism, and excessive weight loss. Suspiciousness may occur and can develop into a full paranoid psychosis that is indistinguishable from acute paranoid schizophrenia. The psychosis may extend beyond the period of acute intoxication, and some experts believe that it may recur or become chronic, despite abstinence from drug use.
10–12 A preoccupation with minutiae and details can arise, leading to compulsive repetitious behaviors. Skin picking is not uncommon and is, at times, accompanied by tactile hallucinations and delusions of parasitosis. Abrupt cessation of long-term use produces withdrawal, which can last for days and may be accompanied by dysphoria, irritability, and agitation.
13Effects on Neurotransmitter Systems
Acute administration of methamphetamine increases extracellular dopamine (DA) levels through the reverse transport of DA and by the displacement of DA from vesicular stores.
14,15 Methamphetamine also impacts serotonergic, noradrenergic, and glutamatergic systems through interactions with 5-HT transporters, monoamine transporters, and
N-methyl-D-aspartate (NMDA) receptors. Repeated administration of the drug to rodents or nonhuman primates decreases striatal concentrations of DA and DA metabolites in several brain regions.
16–18Dopamine
The neurotoxic effects of methamphetamine lead to alterations in levels of DA, with increased levels correlating with subsequent decreases in DA neurotransmission.
19 Conversely, DA receptor antagonists or synthesis inhibitors attenuate methamphetamine-induced neurotoxicity.
19,20 DA uptake inhibitors attenuate methamphetamine-induced deficits in DA neuronal activity, suggesting that the dopamine transporter (DAT) is critical to the mediation of neurotoxicity.
21–23 However, Yuan et al.
24 found that the depletion of DA with reserpine or alpha methyl paratyrosine (AMPT), with the process held at normal temperatures, did not protect against the neurotoxic effects of methamphetamine. Although the DAT may function in damage mechanisms, the role for endogenous DA seems less defined.
In a number of findings, damage has been observed in animals exposed to methamphetamine, particularly the degeneration of DA nerve terminals, with reductions in DAT activity, tyrosine hydroxylase activity, and vesicular monoamine transporter-2 (VMAT) protein levels.
21,23,25–27 Human imaging studies have shown reductions in DAT levels.
28–30 Alterations in both humans and animals occur within days of drug exposure and may persist for months or years.
18,28,31Serotonin
In addition to DA, other neurotransmitters are affected by methamphetamine use, including 5-HT and cholinergic systems. The mechanism of methamphetamine damage to 5-HT fibers is unknown, and the release of DA is believed to be an intermediate step in the cause of 5-HT degeneration.
32,33 Blocking DA synthesis prevents 5-HT degeneration.
34,35 The relationship between DA release and 5-HT fiber damage is complex and may involve other neurotransmitter systems.
36After exposure to methamphetamine, marked effects may take place in the serotonergic system. Zhou et al.
37 reported that, within hours of methamphetamine injection in monkeys, region-specific dose effects were observed, with the frontal cortex and hippocampus affected at lower amphetamine doses and the striatum and parietal cortices at higher doses. Targets of methamphetamine insult included 5-HT pathways (e.g., medial forebrain bundle, cingulum bundle, indusium griseum, fornix, and stria terminalis). In contrast, the temporal cortex, hypothalamus, and brainstem were relatively spared. Unlike studies on DA, few studies imaging the serotonin system have been performed in humans, and none have been conducted with methamphetamine using subjects.
38Other Neurotransmitters
The excitatory neurotransmitter glutamate may function in methamphetamine-induced neurotoxicity, with acute administrations of methamphetamine producing marked and prolonged increases in glutamate release.
39,40 NMDA glutamate-receptor antagonists decrease methamphetamine-induced DA overflow and prevent reduction in tyrosine hydroxylase activity.
41–43Studies have investigated how nitric oxide (NO) functions in methamphetamine-induced neurotoxicity. Abekawa et al.
44 examined the effect of NO synthesis inhibition on methamphetamine-induced dopaminergic and serotonergic neurotoxicity in rats. Their findings revealed that toxic doses of methamphetamine significantly decreased contents of DA, dihydroxyphenylacetic acid (DOPAC), and homovanillic acid (HVA) in the striatum; and contents of 5-HT were greatly reduced in the striatum, nucleus accumbens, and medial frontal cortex. However, coadministration with the NO synthase inhibitor, N-omega-nitro-L-arginine methyl ester (LNAME), lowered the methamphtetamine-induced decreases in the striatum in contents of DA, DOPAC, and HVA but did not alter the decreases of 5-HT in the nucleus accumbens, medial prefrontal cortex, or striatum. Therefore, it is conceivable that methamphetamine-induced dopaminergic neurotoxicity, but not serotonergic neurotoxicity, may be related to NO formation that is caused by the activation of postsynaptic DA receptor. Hence, DA, glutamate, and perhaps NO may all function in the neurotoxic effects of methamphetamine on the DA system.
Imaging Studies
Imaging techniques, such as proton magnetic resonance spectroscopy (MRS), have been used to assess the presence of neuronal damage in human subjects. A noninvasive magnetic resonance imaging (MRI) technique, MRS uses certain pulse sequences to yield chemical spectra that reflect relative concentrations of specific neurotransmitters, or their metabolites, in preselected brain volumes. Using proton MRS, one can obtain measures of N-acetylaspartate (NAA), choline (Cho), myoinositol (mI), and creatine (Cr) content. NAA is present in axons, dendrites, and the cell bodies of healthy neurons, and its levels are thought to be a measure of neuronal viability.
45 In a wide range of studies, abnormally low levels of NAA and abnormally high levels of mI (a glia marker) and Cho have been linked to neuronal damage.
46 Using MRS, Ernst et al.
46 reported uncharacteristically low NAA in the basal ganglia of methamphetamine-dependent subjects. They also observed an inverse correlation between the prefrontal white matter NAA values and years of use, with evidence of abnormally high Cho and mI in the frontal grey matter. In a subsequent MRS study of recently abstinent subjects, Nordahl et al.
47 found evidence of abnormally low normalized NAA (i.e., NAA/Cr) levels and higher normalized Cho (i.e., Cho/Cr) levels in the anterior cingulum (ACC), with no evidence of such findings in the primary visual cortex that served as the control region. Taylor et al.
48 also found evidence of low NAA in the anterior cingulum and a trend toward a low NAA value for the basal ganglia. These findings have been interpreted as consistent with neural damage to the frontostriatal regions. Using MRI analyses, Bartzokis et al.
49 reported no overall tissue loss in frontal gray and white matter. Postmortem confirmation and longitudinal within-subjects studies are necessary in order to confirm these results. Using positron emission tomography [F-18]-fluorodeoxyglucose (FDG PET) techniques, London et al.
50 and Volkow et al.
30 examined brain glucose metabolic changes in methamphetamine-dependent subjects.
Duration of Neurotoxicity
An emerging body of studies aims to establish the duration of methamphetamine damage on neuronal regions and processes. In this section, we review recent studies that were conducted on humans and monkeys and revealed findings pertinent to the continual long-term effects of methamphetamine use. In a study performed on monkeys to assess the persistence of methamphetamine exposure effects, Harvey et al.
51 used in vivo and postmortem techniques. Following a 1-month exposure to methamphetamine, postmortem characterization revealed extensive decreases in the immunoreactivity (IR) profiles of tyrosine hydroxylase, DAT, and VMAT-2. These decreases were observed in the striatum, medial forebrain bundle, and ventral midbrain dopamine (VMD). When assessed at 1.5 years by stereological methods, IR deficits were not associated with a loss of VMD cell number. At 1.5 years, IR profiles of methamphetamine-exposed monkeys, throughout the nigrostriatal dopamine system, appeared to be similar to those of controls, although some regional deficits persisted. The lack of VMD cell loss suggests that the magnitude and extent of dopaminergic deficits may represent transient impairment.
Recent studies conducted on humans suggest that permanent degeneration of the DA system does not occur, and normalization of dopaminergic deficits may take place over time. In their investigation of the postmortem brains of methamphetamine users, Wilson et al.
52 reported lower levels of the DA nerve terminal markers and the DA transporter in the nucleus accumbens, caudate, and putamen. They also suggested that lower levels of striatal DA transporter might explain the rationale for the dose escalation and dysphoria that are frequently found in methamphetamine abusers. They did not, however, find decreased levels of the enzyme 3,4-dihydroxyphenylalanine (DOPA) decarboxylase or VMAT, which is found in patients with Parkinson's disease who have permanent degeneration of their nigrostriatal DA system.
In a study that used positron emission tomography (PET) to measure DA transporter binding, Volkow et al.
53 found evidence of DAT normalization in a paired study of five subjects that were initially examined in early abstinence and then in late abstinence (1.5 to 2 years). These latter findings suggest that chronic exposure to methamphetamine does not necessarily cause permanent deficits or damage to the DA system in human users. In the presentation of her data, however, Dr. Volkow reported that the five subjects still had cognitive deficits following normalization of their DA transporter binding values.
In summary, findings for neuroanatomical, neurochemical, and imaging data support the conclusion that methamphetamine abuse causes damage to multiple transmitter systems that are distributed throughout the brain. Whether the ensuing damage is permanent or reversible over time has not yet been determined.
Cognitive Effects of Methamphetamine Abuse
Drugs that affect the monoaminergic system, such as amphetamine and cocaine, can alter both behavioral and cognitive processes in many ways. Although numerous studies have examined the effects of cocaine on cognition,
54–60 less is known about the long-term cognitive effects of methamphetamine use. As methamphetamine use has been shown to damage both DA and 5-HT systems, the cognitive effects may differ qualitatively from those resulting from cocaine use, which has a differential effect upon these systems.
61 Earlier studies reported that acute doses of methamphetamine administered to drug-naive subjects produced improvements in cognitive processing.
62–64 Studies using sleep-deprived individuals revealed that administration of amphetamines reduced reaction times and improved performance.
62 Other investigations have reported similar results in nonfatigued individuals.
65 Fleming et al.
66 observed that single doses of dextroamphetamine reduced reaction times on a continuous performance test but had no significant effect on other attentional measures. Additional studies reported improvements in verbal memory performance as a result of the administration of methamphetamine.
64 In contrast to the improvements cited above, some investigations found no cognitive improvements associated with amphetamine administration.
65,67More recent studies have shown that long-term methamphetamine use is associated with impaired performance on a number of cognitive tasks.
68–71 Volkow et al.
71 tested a group of methamphetamine-dependent subjects and found that they exhibited performance deficits in both verbal memory and motor function. Simon et al.
70 observed that the methamphetamine users in their study did not differ from controls on global Intelligence Quotient (IQ) measures, though they did perform significantly worse on tests of memory recall. The methamphetamine group in this same study had difficulty with tests that measured manipulation of information (i.e., Digit Span Task and Trail Making Part B), but had no problems on tasks that measured psychomotor speed separately (i.e., Trail Making Part A). The methamphetamine group also displayed deficits in abstract reasoning and task shifting strategies. In their study, Ornstein et al.
72 reported that methamphetamine-dependent subjects displayed specific deficits in shifting categories on a computerized task shifting experiment when compared with chronic heroin users and nonsubstance using control subjects.
Clinically, methamphetamine-dependent individuals appear distractible and exhibit difficulties in sustaining attention. Our lab has examined the attentional performance in a group of methamphetamine-dependent individuals, using a sensitive, computerized battery of selective attention tasks to better understand the nature and specific properties of their cognitive dysfunction.
69 A single-trial Stroop priming task; a task switching experiment, with response conflict trials; a spatial priming task; and a go-no-go task were all used in the assessment. When compared with controls, the methamphetamine-dependent individuals displayed more consistent patterns of difficulties in suppressing irrelevant task information. These deficits became apparent in both reaction time measures and accuracy rates. Although the methamphetamine-dependent individuals exhibited deficits in the explicit components of the tasks, they had preserved attentional priming, which is a noteworthy dissociation in attentional performance. Priming is an implicit component of cognitive processing that remains intact in some disorders, even when other cognitive abilities are impaired, such as in global amnesia. In disorders such as schizophrenia, however, priming does not remain undamaged.
73–74Dopaminergic Systems and Cognition
The dopaminergic system often exhibits modulatory effects on many cognitive functions, including memory, attention, task switching, and response inhibition.
74 Recent studies in humans and animals revealed that DA depletion in the mesostriatum can lead to both a slowing in reaction time and deficits in overall task performance.
75 Dopaminergic systems within the prefrontal cortex (PFC) are vital to the formation of attentional sets and switching behavior, with DA neurotoxic lesions of the PFC disrupting the establishment of attentional sets.
68,75,76 Deficits in task switching have been observed in patients with Parkinson's disease.
77–79 This suggests that, functioning in the mesostriatum, DA may also play a role in the creation of attentional sets.
80 As previously discussed, long-term methamphetamine use can impair the DA system in both humans and animals. Therefore, the logical assumption is that methamphetamine-induced damage to DA systems may contribute to some of the cognitive deficits observed in methamphetamine-dependent subjects.
Serotonergic Systems and Cognition
The depletion of central 5-HT in rats has been shown to increase the level of premature responding that is independent of the ability to detect and respond accurately to visually displayed targets.
81 Harrison et al.
81 proposed that 5-HT depletion in animals may increase impulsivity by altering 5-HT-DA interactions and, possibly, removing the inhibitory effects of 5-HT on DA neurotransmission. Others have suggested that lower 5-HT levels may actually enhance attentional focus under other conditions, although reduced serotonin levels may increase impulsive responses and errors of commission in some circumstances.
82,83 In an attentional search task that required the suppression of a distracting stimulus, Coull et al.
82 found that subjects on a tryptophan-depleted diet ignored the distractor more promptly than those in the placebo control group. Data from their study suggests that reduced serotonin levels may contribute more to impulsive patterns of responses rather than to deficits in selective attention. Reduced serotonin levels in humans have been linked to impaired long-term memory performance.
84,85 Memory performance in 27 tryptophan-depleted healthy subjects was assessed at immediate and delayed intervals, with specific memory impairments emerging in the delayed condition.
85 In contrast, no short-term memory, perceptual, or psychomotor deficits were observed.
Methamphetamine-dependent subjects show cognitive patterns that are similar to those of subjects who have been on tryptophan-depleted diets.
68 Rogers et al.
68 used a novel computerized decision making task in order to compare the decision making behavior of 1) chronic amphetamine abusers, 2) chronic opiate abusers, 3) patients with focal lesions of orbital frontal cortex or dorsolateral/medial prefrontal cortex, and 4) tryptophan-depleted normal volunteers. Chronic amphetamine abusers and patients with damage to the orbitofrontal cortex—but not other sectors of the PFC—showed suboptimal decisions and deliberated for significantly longer periods of time before making choices. Subjects with lower plasma tryptophan performed similarly to subjects with histories of amphetamine abuse. Such a discovery is salient, as studies conducted on animals have revealed reduced levels of 5-HT due to high-dose methamphetamine administration.
31 Limbic regions that are innervated by 5-HT projections are especially sensitive to the effects of repeated amphetamine administration in animal studies,
17,31 thus one mechanism for altered decision making associated with chronic amphetamine abuse in humans might be the altered serotonergic modulation of the ventral PFC and its interconnected structures. Increased impulsivity and impaired judgment that are associated with methamphetamine use may be linked to the depletion of both DA and 5-HT neurotransmitter systems.
Electrophysiological Studies
Disrupted attentional processing as a result of methamphetamine use has been detected using electrophysiological techniques in both animals
86 and humans.
87,88 Effects of repeated administration of methamphetamine in rats were examined using electrophysiological techniques to measure an attentional component (P3-like potential) of the event-related potential (ERP) while the animals were performing an active discrimination task. The rats were trained to press a bar after cessation of a target tone (1000 Hz) that lasted for 800 ms and to withhold an overt response to the standard tone (2000 Hz). Following a series of injections with saline or methamphetamine, ERPs were recorded in rats. In the rats that received methamphetamine, the amplitude of an attention-related ERP (the P-3 like potential) decreased without alterations in latency. These results are consistent with alteration in catecholaminergic neurotransmission that is induced by repeated methamphetamine administration. Human subjects were used in a study in which auditory ERPs were recorded for 15 methamphetamine-dependent individuals during a selective attention test.
87 Attention-related negative ERP components were reduced and latency was delayed when compared to normal controls, which suggests impairment in auditory information processing. Another experiment revealed abnormal electrophysiological activity in methamphetamine-dependent subjects who exhibited reduced P3a amplitude and delayed P3b latency, both markers of selective attention.
88 The authors suggested that these findings might be linked to the dysregulation of functioning that is related to impairment of the frontal cortex.
The prevalence of methamphetamine abuse has reached epidemic proportions throughout the United States. The review of relevant literature supports the assertion that cognitive impairments exhibited by methamphetamine-dependent individuals may be the result of the neurotoxic effects of multiple neurotransmitter systems that are distributed throughout the cortex. Deficits in attentional inhibition, increased impulsivity, and impaired task-switching strategies may all be consequences of collective damage to the DA and 5-HT systems. A convergence of evidence from behavioral studies in humans, animal research, and the field of neuroimaging is needed to further examine the neural basis of cognitive deficits in methamphetamine-dependent individuals. Increased knowledge of how neural regions and cognitive functions are affected by excessive methamphetamine use could benefit both pharmacological and therapeutic treatment interventions. Targeted and longitudinal research that uses neuroimaging techniques, along with sensitive measures of cognitive function, will have profound implications for the neuroscience of drug addiction, which could subsequently guide pharmacological and treatment interventions.
ACKNOWLEDGMENTS
This work was supported in part by a grant from the University of California Davis Department of Psychiatry, the NIDA grant DA10641, and the NIDA grant DA14359