Repetitive behaviors are one of the three core diagnostic domains of autism. There is potential overlap between this behavioral domain and obsessive-compulsive disorder (OCD). Need for routine and order, accompanied by anxiety if those are disrupted, has been reported in patients in both diagnostic groups.
2 Several studies have attempted to better describe the nature of repetitive behaviors in autism. In one study, compulsions in the autistic group were more common than obsessions, and no patients had obsessions alone.
3 Patients with autism had significantly fewer obsessions involving aggression, sex, religion, symmetry, contamination, and somatic concerns, and fewer higher-order repetitive behaviors such as cleaning, checking, and counting, commonly reported in OCD.
3 In another study, children with a high repetitive-behavior domain score on the Autism Diagnostic Interview–Revised (ADI–R) were significantly more likely to have parents with OC traits or OCD than children with low scores on this domain.
4However, there have been few studies that have evaluated the factor structure of the repetitive-behavior domain in autism. Factor analysis is a powerful set of statistical methods that may be used to reduce the number of variables in this domain.
5 This would simplify the description of data, allow for stratification of individuals with autism for genetic studies and, perhaps, lead to treatments and interventions specific to factor subtypes. Most published studies have used the ADI–R for factor analysis of this domain in autism. In these studies, two factors have been identified: 1) repetitive sensory/motor behaviors; and 2) resistance to change/insistence on sameness.
6–9 Despite the impressive degree of agreement between these studies, there are certain disadvantages in using the ADI–R for the purpose of identifying distinct factors within the repetitive-behavior domain. First, there are only 11–13 items available for such an analysis, limiting the diversity of repetitive behaviors that can be assessed. Also, there are no questions in this instrument that specifically identify obsessions. Finally, this instrument is not an outcome measure and, as such, factor-analytic results cannot be translated into dimensional instruments that can be used as outcome measures in intervention studies. The latter shortcoming particularly limits the ADI–R's usefulness in this area.
Perhaps because of these limitations, other measures of repetitive behaviors are beginning to be factor analyzed in autism. In one study, the Maudsley Item Sheet was used, and the presence of two correlated factors was supported by confirmatory analysis: “cognitive rigidity” and “sensory motor.”
10 This study was again limited by the number of items available for factor analysis and the inclusion of participants with mental retardation, but not autism, in the sample. Moreover, this instrument is not widely used. Finally, there have been factor analyses of the Repetitive Behavior Scale–Revised (RBS–R).
11–13 This instrument is a parent measure and was designed to assess the various repetitive behaviors observed in individuals with autism spectrum disorders. Originally, six factors were identified: “ritualistic behavior,” “sameness behavior,” “stereotypic behavior,” “self-injurious behavior,” “compulsive behavior,” and “restricted interests.” In a follow-up replication study, the original ritualistic and sameness factors were combined.
12 Georgiades et al.,
13 in a recently published replication study in a Greek sample, suggested a two-factor solution with a “high-order” factor reflecting compulsions, rituals, insistence on sameness, and restricted behaviors, and a “low-order” factor reflecting stereotyped movements and self-injurious behaviors. These studies were limited by difficulties in sample characterization (large population samples were used, and, as such, the diagnosis was not confirmed by the authors).
The Y-BOCS is a clinician-rated instrument designed to measure severity of disease in patients with OCD. It allows the clinician to incorporate all data available, including caregiver and clinician observations, into the ratings. Factor analysis of this checklist has been attempted in OCD but not in autism. Also, factor analysis of this instrument may be of particular importance in the design of intervention studies, since this has been the instrument of choice (along with various modifications) as an outcome measure in medication trials targeting repetitive behaviors in autism.
14–17 The goal of this study was to attempt such an analysis in an effort to reduce the number of variables and identify distinct components that may inform genetic and intervention studies.
RESULTS
Sample Description
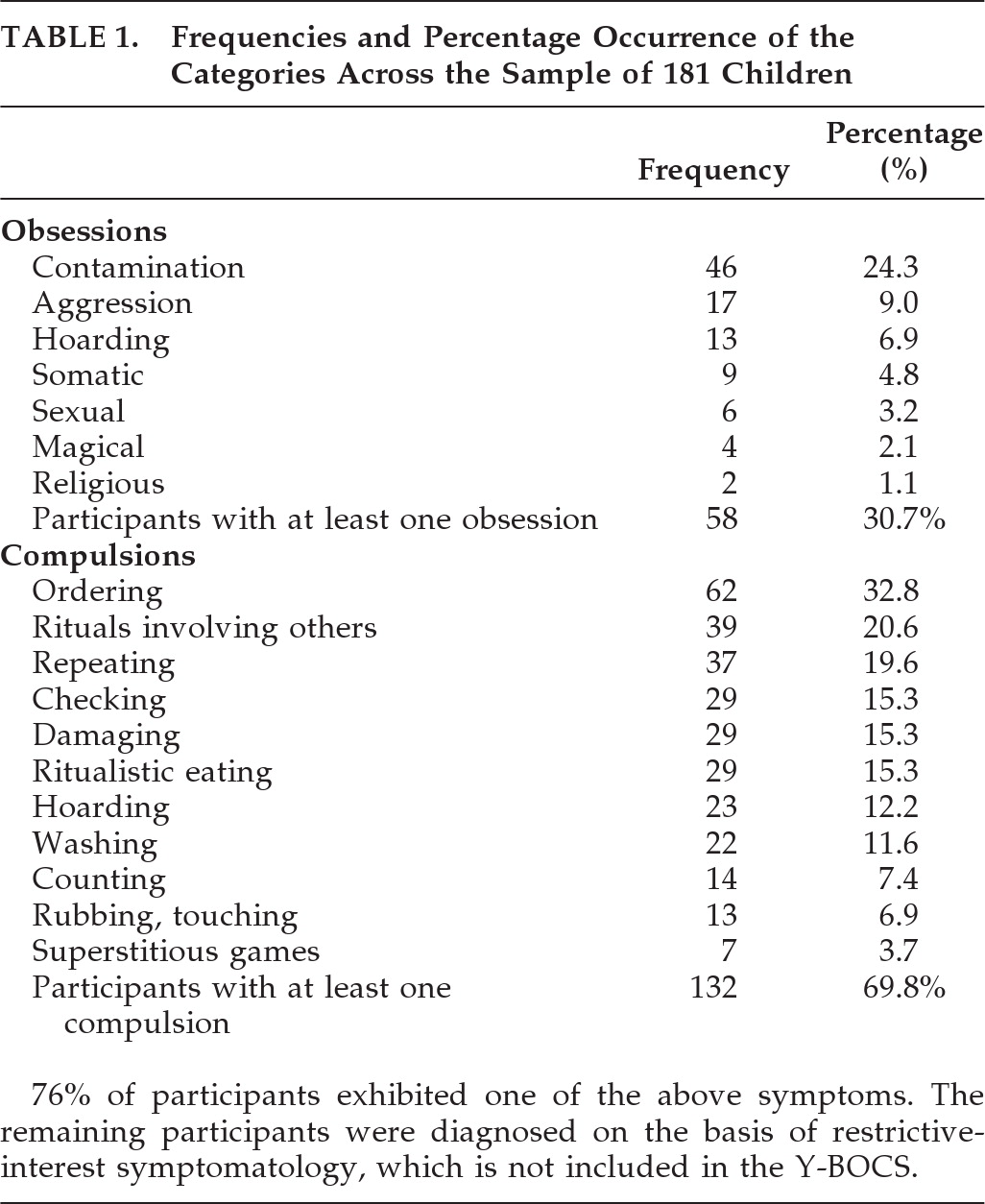
A sample group of 181 participants from 109 families provided data for these analyses. The age range was 2–18 years (mean: 8 [SD: 5]); 83% were male. The majority of the sample (68%) was highly verbal, with daily functional use of spontaneous, echoed, or stereotyped language involving phrases of three words or more that include a verb and are comprehensible to other people; 14.5% had at least five words that were used on a regular basis, although they had no functional use of three-word phrases; 17.5% of participants were completely non-verbal or used fewer than five words. Lastly, the Y-BOCS scores ranged from 0 to 37 (mean: 13.4 [SD: 8]). The lifetime frequencies (current or past occurrence) of the 18 symptoms included in these analyses are presented in
Table 1.
Factor Analysis
We evaluated a variety of possible structural models that were derived from both theoretical considerations and empirical observation. Initially, we hypothesized that a correlated two-factor model consisting of an obsession factor (OBS) and a compulsive-like factor would provide a good representation of the structure. However, this model did not fit the data well. We proceeded with a principal-axis factor analysis, followed by both varimax (orthogonal) and promax (oblique) rotations (in order to be consistent with previous factor-analytic approaches to the Y-BOCS).
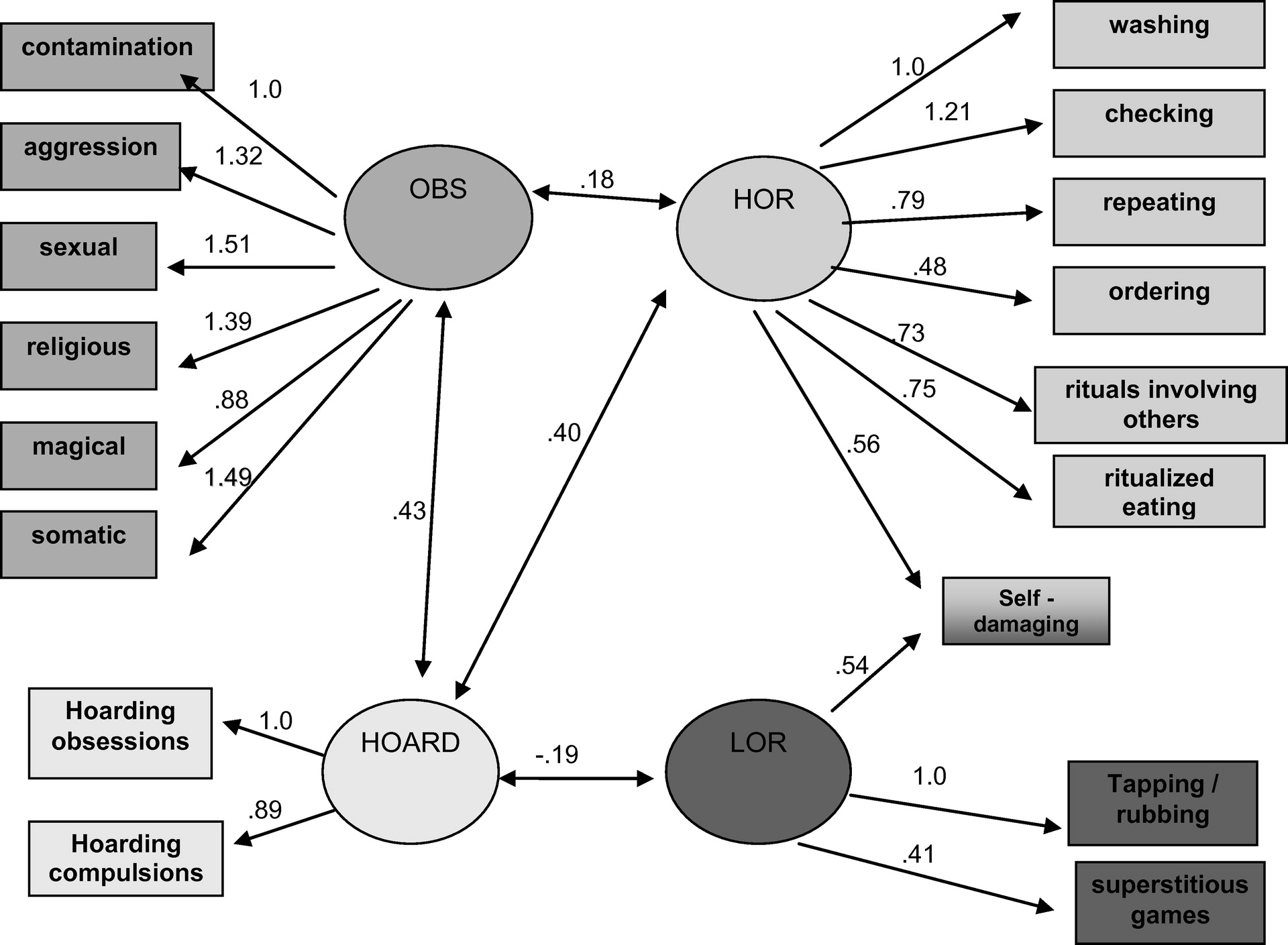
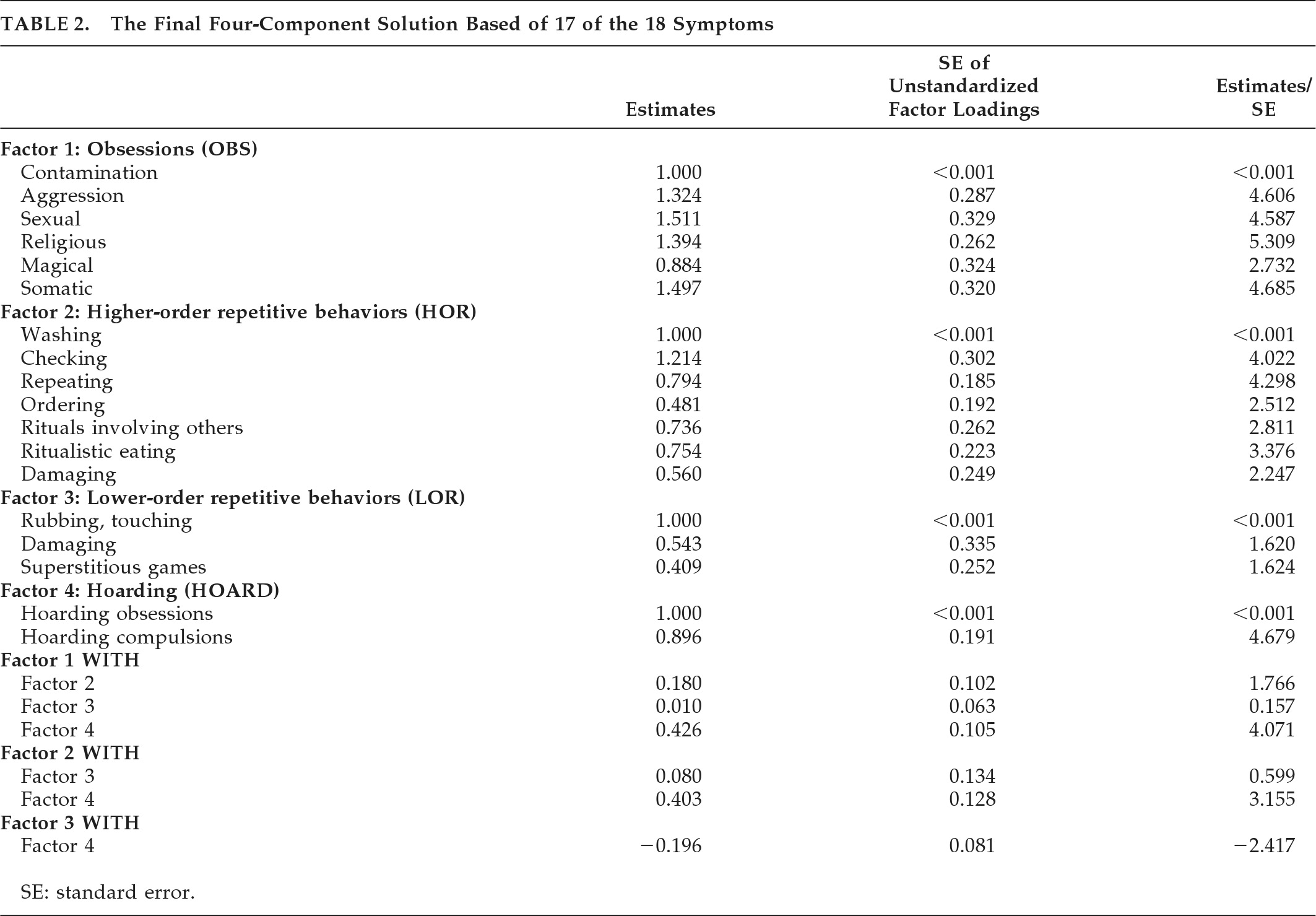
5,21–24 A third factor was suggested that included damaging behaviors, superstitious games, and tapping/touching. We then hypothesized a three-factor solution that consisted of an obsession factor (OBS), a higher-order repetitive behavior factor (HOR), and a lower-order repetitive behavior factor (LOR). Still, this solution did not fit the data well, with a significant chi-square and a RMSEA of 0.086. Generally, models are considered to fit well if the RMSEA is roughly 0.05 or less. Inspection of the parameter estimates and fit statistics suggested several modifications that might improve the model. The major modification suggested by these exploratory analyses was to combine hoarding obsessions and hoarding compulsions together on a separate hoarding (HOARD) factor. The resulting correlated four-factor model showed a better and marginally-acceptable fit to the data. However, the chi-square test remained significant. A second modification suggested cross-loading the Damaging Compulsions item on both the HOR and the LOR factors. We thus allowed this symptom to be associated with both Compulsion factors in the correlated four-factor model. Finally, the Compulsion symptom of counting generally did not relate to any of the four factors, so we eliminated it from the symptoms we were modeling. This resulted in a four-correlated-factor model of the structure of the 17 remaining symptoms that provided an acceptable fit to the data, as indicated by a nonsignificant chi-square test of model fit (χ
2[25]=37.01; p=0.0576; RMSEA=0.052). This model is shown in
Figure 1.
Figure 1 and
Table 2 show the loadings of the 17 variables on the four factors. All loadings are significantly different from 0 (two-tailed p<0.05) except the loadings on the LOR factor, which are marginally significant (two-tailed p<0.10). Although correlations among all factors were estimated, only the significant inter-factor correlations are shown. Thus, HOARD is related to all three of the other factors (two-tailed p<0.05), and OBS and HOR are marginally related (two-tailed p<0.10).
Description of the Sample Based on the Four Components
Ultimately, the usefulness of these structural analyses will be in the identification of types of patients who exhibit different patterns of repetitive-behavior symptomatology. The existence of such types may suggest different genetic bases for the disorder and also different treatment strategies. Thus, we looked for the identification of different groups of patients who could be characterized by specific types of symptoms.
Of the 181 participants, 83 had pure symptom patterns; that is, they exhibited behaviors that all fit within a single factor: 14 had only obsessions; 61 had only higher-order repetitive behaviors; 6 of these had only lower-order repetitive behaviors; and 2 were purely hoarders. It should be noted that the identification of pure symptom cases was complicated by our decision to include Self-Damaging on both the higher- and lower-order repetitive behaviors. Twenty-nine individuals exhibited damaging compulsion symptoms. One of these participants had only damaging symptoms and so was initially counted as a pure case on both HOR and LOR. Therefore, we did not include this individual in our count of pure cases. Of the remaining 28 participants with damaging compulsions, 7 had only other HOR, and so are counted as pure HOR cases. Two of these individuals had only other LORs, and so are counted as pure LOR cases. The remaining 19 individuals with self-damaging compulsions had a mixture of other symptoms, and so are not pure cases (i.e., they are mixed cases). The numbers reported above reflect these considerations.
There was no difference between the 83 pure and the 98 mixed cases on age (t=1.76, p=0.08), gender (χ2=0.614; NS), or level of language usage (χ2=0.208; NS). Among the 83 “pure” patients, we also did not find statistically significant differences among the four symptom classes on age (F[3,81]=0.172; NS), gender (χ2=2.52; NS), or level of language (Fisher's exact test, NS).
DISCUSSION
This study confirms that there is marked heterogeneity in the repetitive behaviors of autism. In our sample, we observed low frequencies of checking, ordering, counting compulsions, and self-damaging, similar to those reported by McDougle et al.
3 However, our sample demonstrated a higher frequency of washing and lower frequencies of repeating, hoarding, and touching. Also, 30% of participants reported having obsessions, and 17% reported only obsessions. This is unlike the above study where no participants were reported to have repetitive thoughts in the absence of compulsions. Given that the nature of repetitive behaviors may vary with IQ and age,
26 our differences with the previously-mentioned study may reflect significant differences in the IQ between the two samples.
Previous factor analyses of the Y-BOCS in populations with OCD have led to four different structures. Only the original study included a pure Obsession factor,
21 whereas the studies that followed disaggregated Obsessions and Compulsions,
5,22–24,27,28 with one exception.
29 In that study, Obsessions arose again as a pure factor, although this may include pleasurable repetitive thoughts, typically seen in autism. However, in our sample, the most frequently endorsed obsession was fear of contamination, which cannot be easily conceptualized as a pleasurable restricted interest.
The second factor identified (higher-order repetitive behaviors [HOR]) includes ordering, washing, repeating, checking, and ritualistic eating behaviors, as well as rituals involving others. All of these behaviors are higher-order, OCD-like repetitive behaviors. Again, one should be mindful that such behaviors in autism may not be egodystonic.
30,31The third factor (lower-order repetitive behaviors [LOR]) includes self-damaging behaviors, need to touch or rub, and games/superstitious behaviors, mostly lower-order repetitive behaviors. Such behaviors are not specific to autism and are seen in children with mental retardation (MR), other static encephalopathies,
32 frontal-degeneration syndromes,
33 and other neurological disorders, although severity and frequency are higher in autism than in MR.
11 As noted earlier, in this sample, self-damaging loaded almost equally on higher- and lower-order repetitive behaviors, which led us to allow this symptom domain to correlate with both the second and third factor. This may be of interest in this population and likely consistent with the authors' clinical impressions that, whereas some affected individuals may use self-injury to decrease anxiety, others self-damage to regulate arousal. As such, this symptom domain may need to be better described/delineated in the Y-BOCS checklist, if it is used in autism-spectrum populations.
The fourth factor (Hoarding [HOARD]) includes obsessions and compulsions related to hoarding. Hoarding is not a symptom-domain specific to autism and has been extensively studied in OCD. It seems to be characterized by a distinct biological profile, resistance to treatment with serotonin-reuptake inhibitors, and specific comorbidity profiles.
34 In our sample, hoarding also seems to be a separate dimension within the repetitive-behaviors domain.
Ultimately, the issue will be whether these different types of patients exhibit differential gene expression or differential response to treatment: 46% of the participants in our sample had only one “pure” type of symptom. This group can be potentially stratified for factor-type to explore genetic heterogeneity and intervention strategies for factor subtypes. From a phenomenological point of view, HOR may reflect mostly behaviors generated to decrease anxiety, whereas LOR includes repetitive behaviors possibly associated with regulating arousal. The evidence for efficacy for serotonin-reuptake inhibitors is mixed, with earlier studies showing a moderate effect,
16,35 but recent data showing no effect of citalopram on repetitive behaviors in autism.
17 Antipsychotics have also been shown to have some efficacy for the treatment of repetitive behaviors of autism,
37,38 and so have anticonvulsants.
37 Whether these medications are differentially affecting higher- versus lower-order behaviors remains to be seen.
This is the first factor analysis study of the Y-BOCS in any population that used estimates of tetrachoric correlations, rather than simple (and attenuated) Pearson correlations among dichotomous symptom categories as the basis of the analysis. We also used a confirmatory factor analysis strategy that allowed us to directly test the adequacy of the fit of our factor model to the data. Still there are limitations of this study. First, the original Y-BOCS checklist was used, as opposed to the more recently adapted form of this instrument for autism.
32 Furthermore, the checklist categories were used for the analysis. There are no data to verify the validity of these categories in autism, but we felt that, given that the original version of the Y-BOCS was used, an item-by-item analysis would show significant loadings on items labeled “other.” Given that we did not have detailed descriptions of such items, their inclusion would render the interpretation of the data more difficult. More importantly, the sample is heterogeneous in terms of age. We were not able to drop the preschoolers from the analysis, given power considerations, but do acknowledge that, given that repetitive behaviors seem to change with age, such an analysis will be of most importance in a follow-up larger cohort. Also, siblings were included in the study, again, given power concerns, but likely do not represent completely independent observations. Lastly, we had no information on IQ of the participants. We described the sample using the participants' level of language, instead. Future studies replicating our data may use the adapted-for-autism Yale-Brown Obsessive-Compulsive Scale (Y-BOCS) checklist, including all the items of the checklist in the factor analysis, and may consider using the Obsession subscale of the CY-BOCS (Children's Yale-Brown Obsessive-Compulsive Scale). Also, the Self-Damaging category may need to be further described to allow for clarification of symptoms/signs coded here.
We have identified a four-factor structure to describe the repetitive behaviors in autism. Replication of our results in a larger cohort is necessary, but this study represents another step in attempting to identify endophenotypes within the autism population. Such endophenotypes may be associated with distinct neurobiology and genomic architecture, and their identification may be valuable in identifying more effective treatment strategies for this symptom domain.
Acknowledgments
Previous presentation: Early analytic approaches to an overlapping dataset were presented at the Child Neurology Society Meeting, October 2005, and American College of Neuropsychopharmacology, December 2005.
This work was supported by the Seaver Foundation and NIMH Grant 1 U54 MH66673-0, and an unrestricted fund from Bloorview Research Institute during the data analysis and publication phase.
Disclosure of conflicts: Dr. Hollander has patent applications for oxytocin and memantine in autism. He also lists past consulting for Nastech and Neuropharm. Dr. Anagnostou lists past consulting for InteGragen and current, unpaid consulting with Neuropharm and Proximagen. The other authors have no disclosures.