Lack of consensus as to the heterogeneity of depression is reflected in the evolving diagnostic categories of depressive disorders. Criteria for existing diagnostic categories differ depending on the particular version, and new categories such as minor depressive disorder have been included. For example, the minimal number of symptom groups required for a diagnosis of major depressive disorder changed from DSM-III to DSM-III-R, and distress or impairment caused by symptoms is a new requirement in DSM-IV. There is also a growing interest in subthreshold depression, a classification that requires fewer symptoms than major depressive disorder for diagnosis. The differentiation of dysthymic disorder from major depressive disorder is still an area of intense research
(1). The concept of “double depression,” which captures individuals with both major depressive and dysthymic episodes in specific temporal fashion, poses the question as to whether this classification is a comorbid condition or a separate entity
(2).
Studies on the validity of different depressive disorders have shown inconclusive results. Attempts to distinguish different diagnostic categories have been made by examining symptoms, course, or risk factors. A study by Wells et al.
(3) showed that initial depression severity and level of functional status accounted for more of the variance in outcomes than did type of depressive disorder. A comparison of symptoms among cases of major depressive disorder and dysthymic disorder revealed that symptom presentation did not distinguish clearly between the diagnostic groups
(4). The findings by Romanoski et al.
(5), which were based on the 1981 psychiatric assessments of the Baltimore Epidemiologic Catchment Area (ECA) sample, suggested that risk factors differed between the subjects with major depressive disorder and those with nonmajor depression. However, the diagnosis of nonmajor depression comprised several potentially heterogeneous disorders.
Studies have been conducted to examine the diagnostic validity of the distinction between dysthymia and major depressive disorder
(1,
2,
6), two disorders with a very high rate of comorbidity
(7). The condition of an index episode of major depressive disorder continuous with a preexisting dysthymia and without an intervening period of euthymia of at least 8 weeks has been coded “double depression”
(2). The poor prognoses for double depressive disorders and dysthymic disorders have been recognized
(2), but there is little conclusive evidence that dysthymia is a separate disease entity from major depressive disorder
(6). In addition, evidence from the Medical Outcomes Study
(3) suggests that the outcome for minor depression may be even worse than that for major depressive disorder.
The heterogeneity of minor depression and its separate role from major depressive disorder also have drawn increasing research attention. Family studies suggest that there is a higher risk of minor depression among relatives of probands with major depressive disorder
(8). Epidemiologic evidence suggests that major depressive disorder is more often an exacerbation of a chronic mood disturbance with roots in longstanding vulnerability factors, while in later life minor depression is more often a reaction to commonly experienced stresses
(9). Some researchers have suggested that minor depression is a heterogeneous disorder because some cases of minor depression progress into major depressive disorder while others do not
(10,
11).
This study uses a prospective and population-based sample to assess the discriminant validity and utility of four subcategories of depression: major depressive disorder, depressive syndrome, dysthymia, and comorbid depression (operationally defined here as meeting criteria for both major depressive disorder and dysthymia). The heterogeneity of these depression categories can be probed from three perspectives: symptoms, natural course, and risk factors.
RESULTS
Sample Characteristics
Individuals who met criteria for each of the three depression categories (major depressive disorder, dysthymia, and depressive syndrome) were identified first, which resulted in the following lifetime prevalence rates: major depressive disorder: 9.8% (95% confidence interval [CI]=8.2%–11.4%); depressive syndrome: 16.0% (95% CI=14.2%–17.8%); dysthymia: 7.3% (95% CI=6.1%–8.5%). For the purpose of examination among different categories, individuals were assigned to one of four mutually exclusive lifetime categories: major depressive disorder (5.4%, N=100), depressive syndrome (12.0%, N=223), dysthymia (3.7%, N=68), and comorbid depression (major depressive disorder and dysthymia; 2.8%, N=53).
Subject Transition Between Depression Diagnostic Categories
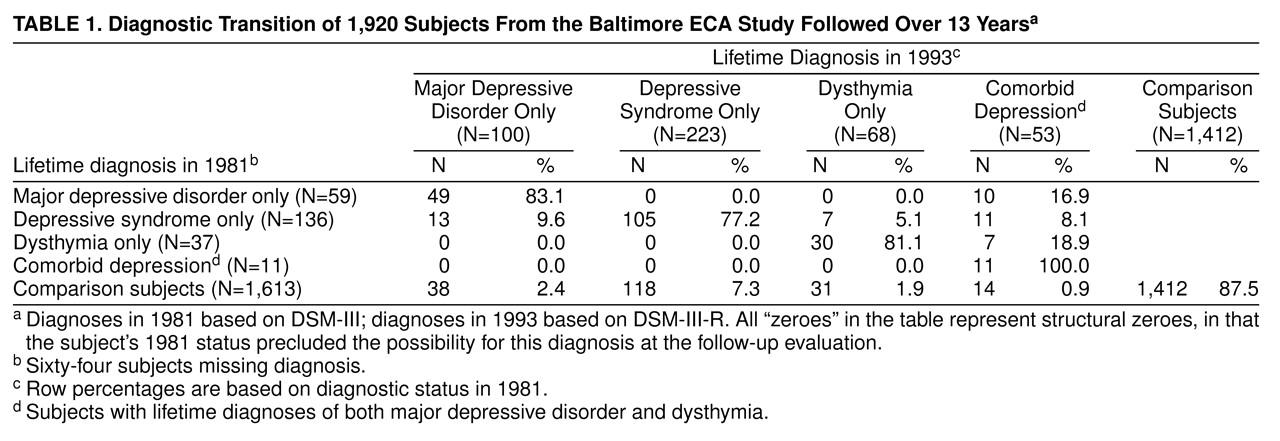
We examined the change of lifetime diagnostic status by cross-tabulating lifetime diagnoses assessed in the wave 1 (1981) interview and lifetime diagnoses summarized from assessments in three waves (1981, 1982, 1993–1996). As seen in
table 1, about 17% of the 59 subjects with major depressive disorder in 1981 developed comorbid dysthymia during the follow-up. About 10% of the 136 subjects with depressive syndrome in 1981 developed major depressive disorder; 5% developed dysthymia; and 8% developed comorbid major depressive disorder and dysthymia. About 19% of the 37 dysthymia subjects in 1981 developed comorbid major depressive disorder.
Symptom Heterogeneity
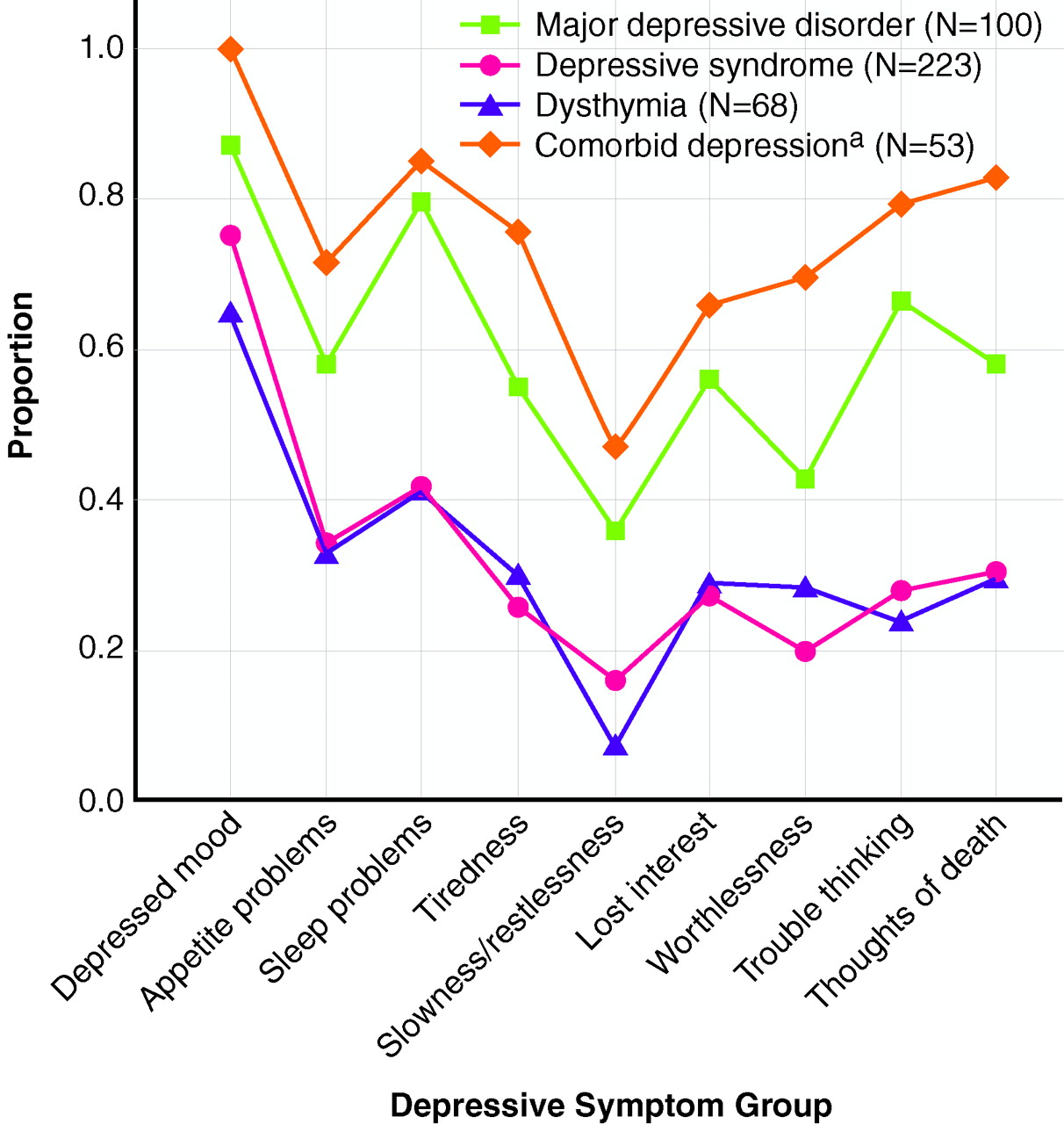
The proportions of individuals in each of the four categories reporting depressive symptoms during their worst episodes are compared visually in
figure 1 and statistically by using polychotomous regression models with homogeneity z tests. Proportions of subjects with depressive syndrome were lower than those of subjects with major depressive disorder for all nine symptom groups. The odds ratio of reporting each symptom group in the major depressive disorder category was significantly higher than it was for the depressive syndrome category (e.g., from the polychotomous regression model for depressed mood, homogeneity z=2.4, N=1,856, p=0.02). For all symptom groups except “feeling worthless,” subjects with dysthymia were significantly less likely than subjects with major depressive disorder to report experiencing the symptoms. Subjects with comorbid depression had significantly higher proportions reporting symptoms of feeling tired, feeling worthless, and suicidal thought/behavior than those with major depressive disorder. To summarize, the associations between each category and the symptom profiles were parallel but significantly differed in the strength of associations (comorbid depression greater than major depressive disorder greater than dysthymia and depressive syndrome), with a few exceptions in the comparison of the major depressive disorder and the comorbid depression categories.
Course Heterogeneity
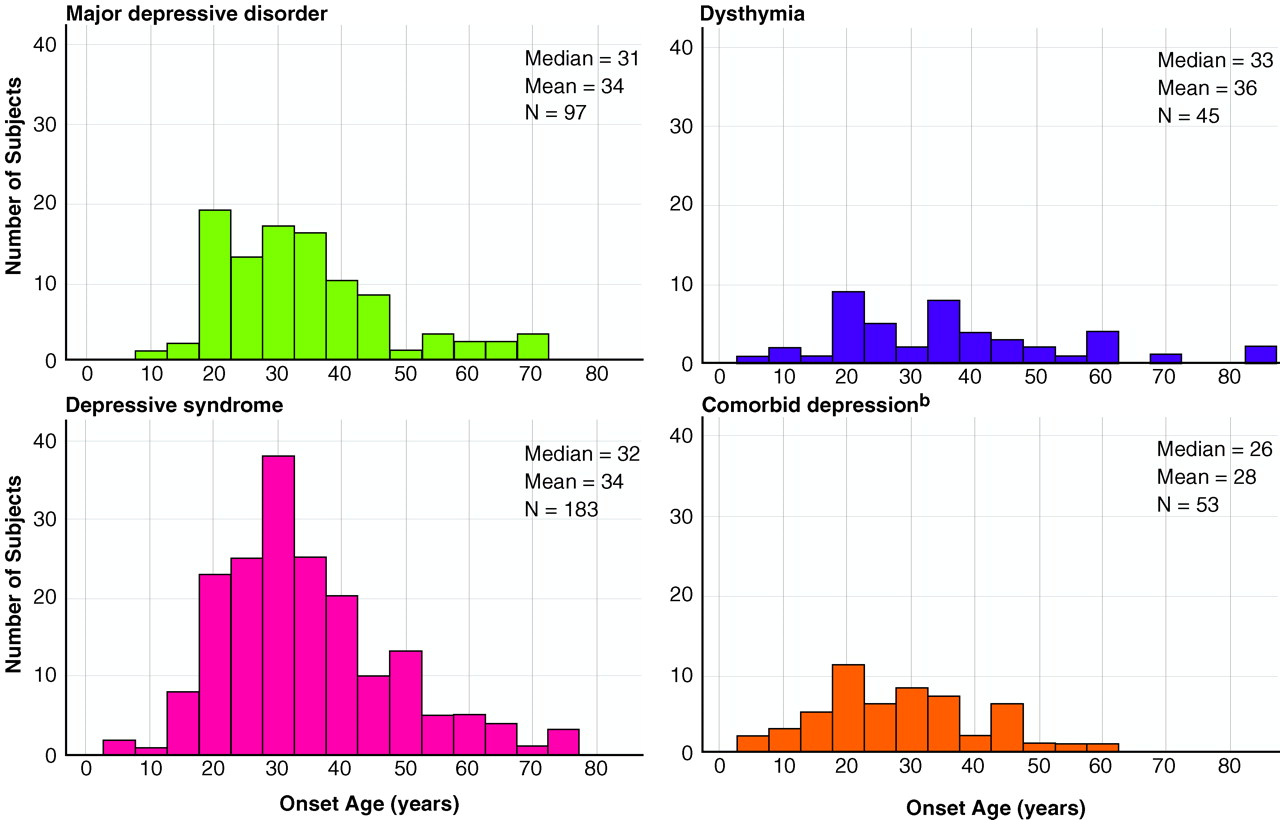
We compared the means of three continuous course variables (age at onset of first depressive episode, length of prodrome, number of depressive episodes) among the four depression diagnostic categories (
figure 2 shows the distributions of age at first depressive episode). The age-at-onset distributions were similar for the major depressive disorder and depressive syndrome categories. There was more variation in the onset distribution for the dysthymia category, and the age at onset was earlier for the comorbid depression category. Statistical tests for an overall difference across the four depressive categories suggested significant differences in age at onset (Kruskal-Wallis χ
2=8.84, df=3, p=0.03) and number of episodes (Kruskal-Wallis χ
2=13.2, df=3, p=0.004), but not in length of prodrome. Next, examination of six paired comparisons by means of Mann-Whitney tests revealed that the comorbid depression category had an earlier onset than the other three categories (versus depressive syndrome: U=3,584, N=236, p=0.004; versus major depressive disorder: U=1,971.5, N=150, p=0.02; versus dysthymia: U=899, N=98, p=0.04). If we used the Bonferroni method to adjust for multiple comparisons by multiplying the above p values by six, only the difference between the comorbid depression and the depressive syndrome categories remained significant.
Next, examination of six paired comparisons again by means of Mann-Whitney tests showed that subjects in the comorbid depression category experienced more episodes than those with major depressive disorder and those with depressive syndrome (versus major depressive disorder: U=1,916, N=148, p=0.03; versus depressive syndrome: U=2,711.5, N=213, p<0.001). If we used the Bonferroni method to adjust for multiple comparisons by multiplying the above p values by six, only the difference between the comorbid depression and the depressive syndrome categories remained significant.
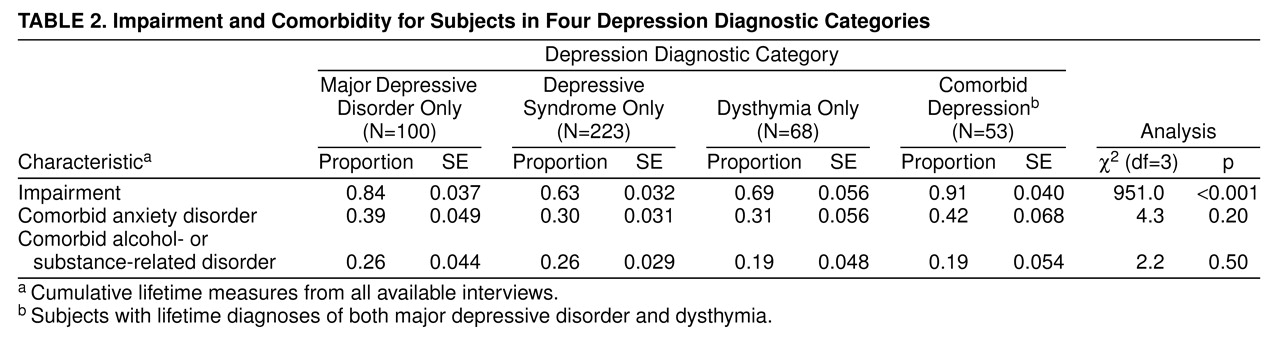
The proportion of subjects reporting dichotomous course variables (impairment, comorbid anxiety disorder, or comorbid alcohol- or substance-related disorder) are compared in
table 2. The chi-square test that compared all four categories suggested an overall difference in the proportion reporting impairment but not in subjects with co-occurring conditions. Subjects in the comorbid depression category reported the highest rate of depression-related impairment (91%), whereas those in the depressive syndrome category reported the lowest rate (63%). Examination of six paired comparisons by means of z tests showed that the impairment rate was higher in the major depressive disorder and comorbid depression categories but lower in the depressive syndrome and dysthymia categories (major depressive disorder versus depressive syndrome: z=4.30, N=323, p<0.00006; major depressive disorder versus dysthymia: z=2.22, N=168, p=0.03; comorbid depression versus depressive syndrome: z=5.36, N=276, p<0.00006; comorbid depression versus dysthymia: z=3.12, N=121, p=0.002). If we used the Bonferroni method to adjust for multiple comparisons by multiplying the above p values by six, all differences except that between the major depressive disorder and the dysthymia categories remained significant.
Risk Factor Heterogeneity Among Four Categories
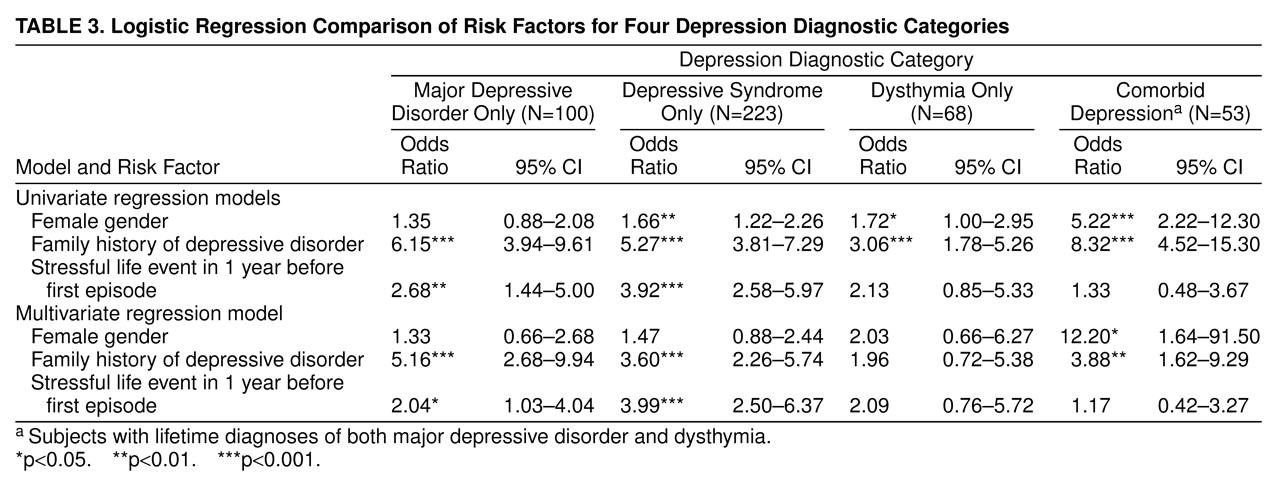
Results of logistic regressions that compared each of the four depression categories and the reference group are summarized in
table 3. In the univariate regression model, subjects with depressive syndrome, dysthymia, and comorbid depression—but not major depressive disorder—had a significantly higher likelihood of being female; the odds ratio for female gender was much higher in the comorbid depression category than it was in the other three categories. The homogeneity z test of odds ratios between the major depressive disorder and comorbid depression categories indicated that the association between female gender and comorbid depression was significantly stronger than that of female gender and major depressive disorder (z=–2.8, N=1,856, p=0.005). Family history was associated with all four diagnostic categories, but the odds ratio for the dysthymia subjects was lower than those of the other three groups. The homogeneity z test of odds ratios between the major depressive disorder and dysthymia categories indicated that the association between family history and major depressive disorder was significantly stronger than that of family history and dysthymia (z=2.6, N=1,594, p=0.009). Stressful life events had a significantly higher likelihood of occurring with major depressive disorder and depressive syndrome but not with dysthymia or comorbid depression.
In the multivariate regression model, the odds ratio for female gender was significant only for the comorbid depression category. The odds ratio for family history of depressive disorder was significantly associated with all categories except dysthymia. Stressful life events were a significant predictor for major depressive disorder and depressive syndrome but not for dysthymia or comorbid depression. A homogeneity z test comparison of odds ratios between the major depressive disorder and the comorbid depression categories indicated a significantly stronger association between female gender and comorbid depression than between female gender and major depressive disorder (z=–2.02, N=1,160, p=0.04).
Both major depressive disorder and depressive syndrome were associated with family history of depression and stressful life events before onset. Yet, for the subjects with major depressive disorder, family history was a stronger risk factor than a stressful life event; for depressive syndrome, a stressful life event was a stronger risk factor than family history. For subjects with comorbid depression, family history was a prominent risk factor in addition to female gender. Dysthymia was the only category not significantly associated with any of the examined risk factors. There were no significant interactions between the examined risk factors in any of the four categories.
DISCUSSION
There was a substantial degree of transition among these depression diagnostic categories over time. Symptoms of a substantial proportion of subjects with dysthymia have only intensified with time. The course of some individuals with depressive syndrome or major depressive disorder has become more chronic. The transition from depressive syndrome to major depression is consistent with what has been reported earlier by Broadhead and colleagues
(24). There have been some discrepancies in subject reports of psychopathology in multiple waves of assessments
(15), so we took information from three waves to establish the lifetime diagnoses in wave 3.
The profiles of depressive symptoms were parallel among the four depression diagnostic categories. Proportionally more subjects with comorbid depression or major depressive disorder reported all depression symptom groups than did those with dysthymia or depressive syndrome. The depressive episode was more severe in subjects with comorbid depression than for those with major depressive disorder, especially when reporting symptoms that may be considered more severe in nature, such as suicidality and worthlessness. Individuals with dysthymia presented symptom profiles similar to those with depressive syndrome.
The four depression diagnostic categories were similar in course characteristics except that the earlier onset for comorbid depression might explain its more severe and recurrent nature and the higher proportion of subjects reporting impairment. Our finding of earlier onset for subjects with comorbid depression is consistent with the study by Sorenson et al.
(25). The high rates of impairment associated with all four categories including depressive syndrome are consistent with existing evidence. Wells et al.
(3) reported that depressive symptoms in the absence of disorder are associated with limitations in six dimensions of patient well-being and functioning (physical functioning, role functioning, social functioning, number of bed days, current health, and being free of pain) when compared with patients with no chronic conditions in a general medical outpatient sample. Judd et al.
(26) found significantly more subjects with depressive symptoms reported high levels of household strain, social irritability, and financial strain as well as limitations in physical or job functioning, restricted activity days, bed days, and poor health status than did subjects without disorder. The lifetime prevalence of major depressive disorder is 5.4%, and in our study 84% of the subjects with major depressive disorder reported impairment. However, the lifetime prevalence of depressive syndrome is 12%, and in our study 63% of the depressive symptom subjects reported impairment. Therefore, we found that more people are impaired by minor depression than by major depressive disorder. This has also been found in prior studies (3, 26). The combination of a higher prevalence and associated impairment of subthreshold or subsyndromal depressive symptoms emphasizes its clinical and public health importance. It has also been demonstrated that individuals with minor depression were associated with 51% more disability days in the community than persons with major depression
(24).
We used the course characteristic onset age for first depressive episode for a standardized comparison of the four depression categories. In this study, the median onset age for subjects with dysthymia was 25 years, while the median onset age for depressive episode was 33 years. Contrary to conclusions based on clinical samples
(25), only a little more than half of the subjects reporting the presence of depressive episode had more than one episode in their lifetime.
Risk factor profiles differed from category to category, and there were linkages between specific risk factors and certain symptom or course characteristics. The association with family history of depressive disorder in episodic forms of depression (major depressive disorder, depressive syndrome, comorbid depression) was strong regardless of symptom severity. The association with stressful life events was stronger for the mild episodic form of depression (depressive syndrome) than it was for major depressive disorder. There was a prominent association between female gender and a more chronic course or more severe symptoms (the comorbid depression category). We used the “stressful life events before the onset of the first depressive episode” as a standardized comparison across disorder categories, in spite of the fact that for the comorbid depression category there are potentially two different onsets. The possibility that different roles might be played by the same risk factor such as stress before the first episodes of different types (depressive versus dysthymic) remain to be investigated.
Not very much is known about the risk factors for depressive syndrome. The existing evidence shows that family history of major depressive disorders and certain type of stressful life events were associated with minor depression
(9), and the association with female gender is still unclear
(10). Our evidence suggests that family history and prior stressful life events, but not female gender, are significant risk factors for depressive syndrome.
The finding that female gender is not a significant risk factor for major depressive disorder has not been reported in earlier studies. We also examined the risk factor profiles for three inclusive categories (all subjects with major depressive disorder, all subjects with depressive syndrome, all subjects with dysthymia), since the four examined categories were mutually exclusive, and the “major depressive disorder” only group did not include those who met criteria for both major depressive disorder and dysthymia. The odds ratio, after adjusting for family history and stressful life events, for female gender among all subjects with major depressive disorder relative to comparison subjects was 3.4 (95% CI=1.5–7.8). In other words, when all major depressive individuals are considered as a group, female gender is more prominent than it is in the group with major depressive disorder only. It is possible that the diagnostic switch between the first and final interviews is captured in the longitudinal study and that the course has been different for female subjects, since more of them have become comorbid, thus changing their diagnostic category and removing them from the major depressive disorder category, while strengthening the association of gender as a risk factor within the comorbid group.
The DIS instrument does not generate the diagnoses of minor depression or double depression. The “depressive syndrome” we used in this study is similar to the category of minor depression
(18). According to current diagnostic concepts, the comorbid depression group of this study consisted of individuals with 1) double depression as defined by Keller and Lavori
(2), or 2) chronic major depressive disorder, or 3) nonconcurrent comorbidity of major depressive disorder and dysthymic disorder. Future research is needed to examine the differences among them. Yet the comorbid depression group represented individuals who were experiencing both an intense and prolonged depressive episode. A limitation of studying a large population sample is the validity of measurements. This study would have been stronger if there were more detailed measures on depression-related impairment. The associations between depressive disorders and the potential risk factors, including family history and stress, could be clarified in future studies with prospectively refined measures. In addition, although three examined risk factors in this study represented potential hormonal, social, genetic, familial, or environmental etiologies for depression, there are still many among the whole spectrum of hypothesized risk factors for depression that were not included.
Since the subthreshold entity, depressive syndrome, is associated with similar etiologic profiles to major depressive disorder and a substantial rate of impairment, we highlight the importance of depressive syndrome in genetic and clinical research. In contrast, the dysthymia category was similar to depressive syndrome regarding symptoms but not risk factor profiles. It did not show a strong relationship to any of the examined risk factors. Its value as a distinct nosologic entity appears to be questionable. The comorbid depression category (lifetime major depressive disorder and dysthymia) has a worse course and is associated with female gender and family history but not with stress. Thus, the evidence suggests a genetic homogeneity and an environmental heterogeneity among three different forms of depression: major depressive disorder, depressive syndrome, and a more severe form of major depressive disorder with chronic and unremitting course.