Anxiety disorders were described as early as the fourth century B.C. in the writings of Hippocrates
(1), but their importance was not fully appreciated until less than 30 years ago. For complex historical reasons the first specialists in psychiatry, the alienists of the early nineteenth century, were mainly concerned with the description and classification of psychotic disorders. As a result, the development of the field of anxiety disorders (as well as the domains of somatization and conversion disorders) was left to specialists in internal medicine and neurology such as da Silva, Briquet, Beard, Charcot, and Freud
(2). The interest of mainstream psychiatry in anxiety disorders would remain limited throughout the first half of the twentieth century because of the prevailing belief that neurotic disorders were benign conditions with nonorganic causes and that their treatment should necessarily be based on some form of psychotherapy
(3).
The realization that anxiety disorders could be successfully treated by pharmacological means
(4), the development of reliable diagnostic criteria
(5), and the advent of modern psychiatric nosology set the stage for a critical reappraisal of the magnitude of the problem of anxiety disorders. Using the DSM-III criteria, the National Institute of Mental Health (NIMH) Epidemiologic Catchment Area (ECA) study showed that anxiety disorders had the highest overall prevalence rate among the mental disorders, with a 6-month rate of 8.9% and a lifetime rate of 14.6%
(1), and affected 26.9 million individuals in the United States at some point in their lives. The costs associated with anxiety disorders in 1990 were a staggering $46.6 billion, accounting for 31.5% of total expenditures in that year for mental health
(6).
Quality of Life: The Concept
It is often said that the cost of human suffering cannot be measured. This truism may no longer be accurate. Many aspects of human suffering (or its absence) can be reliably measured. One of the approaches to this difficult yet invaluable task makes use of the concept of “quality of life.” This concept, developed in the social sciences, was first applied in medical practice to determine if available cancer treatments could not only increase the survival time of patients but also improve their sense of well-being
(7). The concept of quality of life was later applied to compare several antihypertensive medications in terms of functioning, well-being, and life satisfaction
(8).
According to Patrick and Erickson
(9), life has two dimensions: quantity and quality. Quantity of life is expressed in terms of “hard” biomedical data, such as mortality rates or life expectancy. Quality of life refers to complex aspects of life that cannot be expressed by using only quantifiable indicators; it describes an ultimately subjective evaluation of life in general. It encompasses, though, not only the subjective sense of well-being but also objective indicators such as health status and external life situations
(10). Data about quality of life can be used to estimate the impact of different diseases on functioning and well-being, to compare outcomes between different treatment modalities (such as medication and surgery), and, as in the examples mentioned, to differentiate between two therapies with marginal differences in mortality and/or morbidity
(11).
No single definition of quality of life is universally accepted
(12). There is, however, a degree of consensus regarding the minimal requirements for an operational definition of quality of life for employment in health status assessment and research. First, most experts agree that the scope of the concept of quality of life should be centered on the individual’s subjective perception of the quality of his or her own life. This consensus stems from the findings of several sociological studies that have demonstrated that objective conditions of life such as education and income are only marginally related to the subjective experience of a higher quality of life
(13,
14). Second, most authors agree that given the difficulties in assessing the relative impact of the complex experiences that ultimately determine one’s perception of quality of life, quality of life is better approached as a multidimensional construct, covering a certain number of conventionally defined domains
(15). Finally, it is recommended that we avoid the vagaries of abstract and philosophical concepts and concentrate on aspects of personal experience that are related to health and health care (health-related quality of life)
(16).
An example of a subjective multidimensional definition of health-related quality of life was proposed by Patrick and Erickson
(17): “the value assigned to the duration of life as modified by the social opportunities, perceptions, functional states, and impairments that are influenced by disease, injuries, treatments, or policies” (p. 6). Aaronson et al.
(18) suggested that the assessment of quality of life should comprise at least the following four domains: 1) physical functional status, 2) disease- and treatment-related physical symptoms, 3) psychological functioning, and 4) social functioning. Additional domains that are of particular relevance to specific demographic, cultural, or clinical populations (such as sexual function, body image, or sleep) may sometimes need to be included in the assessment to increase the breadth of coverage
(19).
Approaches to Studying Quality of Life in Individuals With Anxiety Disorders
Data regarding quality of life in mental disorders in general, and in anxiety disorders in particular, derive from two types of sources. The first source is represented by epidemiological studies such as the ECA and the National Comorbidity Survey. Although these studies were not specifically designed to study the association between quality of life and mental disorders in the community, they provide a number of indicators from which quality of life can be inferred. These indicators include a subjective assessment of physical and emotional health, psychosocial functioning, and financial dependency
(1,
20,
21).
Clinical studies made by using specifically designed instruments represent the second major source of data concerning quality of life. These instruments may be generic (i.e., attempting to measure multiple important aspects of quality of life) or specific (i.e., focusing on aspects of health status that are specific to the area of primary interest). The latter may be specific to a disease (e.g., panic disorder), to a population (e.g., elderly patients), to a function (e.g., sleep), or to a problem (e.g., pain)
(22). The main advantage of generic measures is that they permit comparisons across conditions and populations. In contrast, specific measures are intended to detect small, meaningful changes in specific conditions to which generic measures may be insensitive.
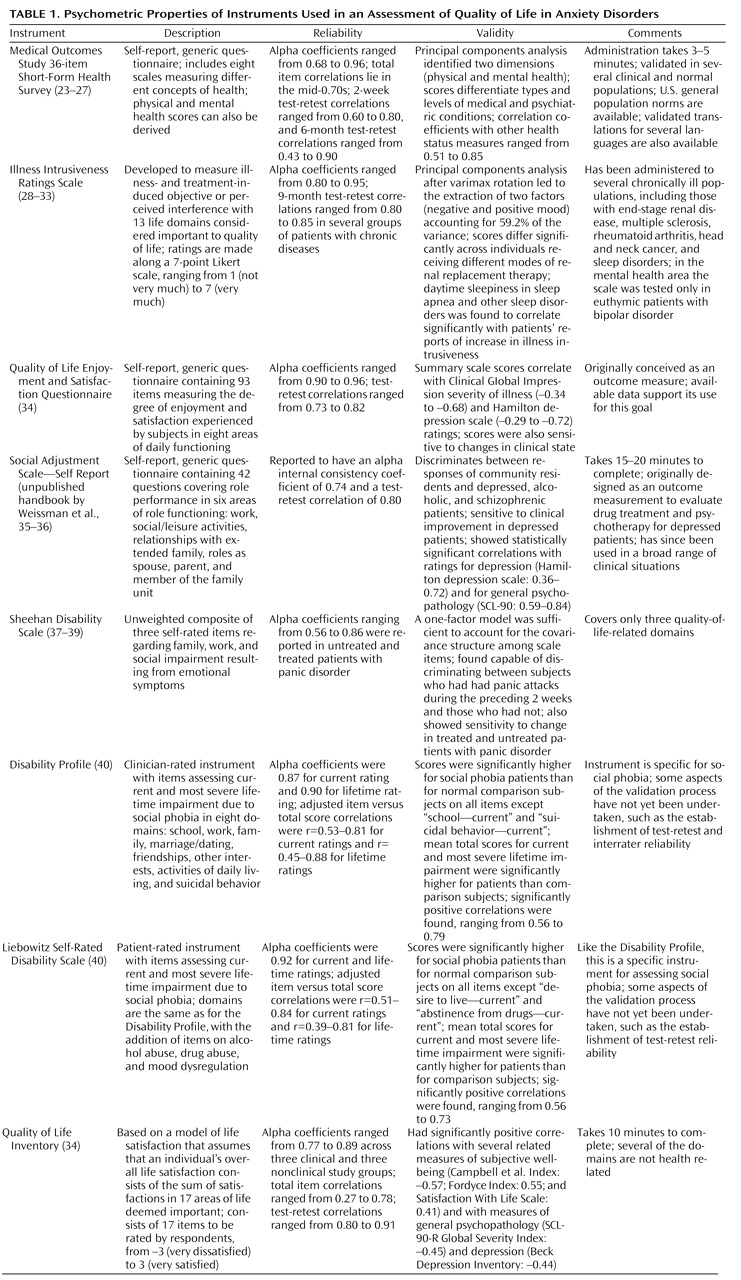
Although quality-of-life data can be collected in interviews or through patient diaries, most studies now employ self-report questionnaires, the most cost-effective method for obtaining patient-related information
(19). For this report, a review of epidemiological and clinical studies that have investigated quality of life (broadly conceptualized) in patients with panic disorder, social phobia, posttraumatic stress disorder (PTSD), generalized anxiety disorder, and obsessive-compulsive disorder (OCD) was conducted by searching MEDLINE and PsycLIT from Jan. 1984 to Oct. 1999. The key words employed were “quality of life,” “impairment,” and “disability.” With few exceptions (to be discussed later), only clinical studies utilizing self-report instruments based on subjective, multidimensional concepts of health-related quality of life that were properly validated were considered. (
Table 1 briefly summarizes the psychometric properties of these instruments.)
Quality of Life in Individuals With Social Phobia
Although social phobia is not a newly recognized disorder
(65), the magnitude of the problem was not fully appreciated until the late 1980s, leading to social phobia being termed a “neglected anxiety disorder”
(66). Even mental health specialists may have felt at first that this disorder, then just recently included in the DSM-III, represented an undue extension of the medical model into the domain of a naturally occurring phenomenon—shyness. Also, the first clinical studies comparing patients with social phobia and panic disorder reported that patients with social phobia tended to be men with higher educational, intellectual, social, and occupational status
(67–
69), suggesting that social phobia was a relatively benign condition. It was not until the ECA findings were reported
(70) that a different profile emerged, showing social phobia to be a common disorder associated with significant disability and impairment.
Studies in Epidemiologic Samples
Although the ECA study did not include direct measures of quality of life, many of the areas surveyed by the ECA are relevant to this issue. For example, the rate of financial dependency among subjects with uncomplicated social phobia (22.3%) was found to be significantly elevated compared with that of normal subjects
(70).
The National Comorbidity Survey
(20) reinforced the perception of social phobia as a major source of disability and suffering. It found a much higher lifetime prevalence for social phobia (13.3%) than the ECA. It showed that social phobia is negatively related to education and income and is significantly elevated among never-married individuals, students, persons who are neither working nor studying, and those who live with their parents. Approximately half of the persons with social phobia reported at least one outcome indicative of severity at some time in their lives (either significant role impairment, professional help seeking, or use of medication more than once); social phobia was also associated with low social support
(71).
Subthreshold Social Phobia
Some studies suggest that the negative impact of social phobia on quality of life may be felt beyond the strict set of diagnostic criteria in DSM-III/DSM-III-R. Davidson and colleagues
(72) examined the Duke University site’s ECA data to compare individuals with social phobia, subthreshold social phobia (i.e., phobic avoidance of public speaking and/or meeting strangers or eating in public not associated with significant functional interference), and nonphobic, healthy comparison subjects. Compared with nonphobic normal subjects, persons with noncomorbid subthreshold social phobia were more likely to be female and unmarried and to report less income and fewer years of education. Persons with uncomplicated subthreshold social phobia were also more likely to report poor grades and lack of a close friend—a measure of perceived social support. Davidson and colleagues
(72) concluded that subthreshold social phobia, in terms of impairment, closely resembles social phobia diagnosed according to the DSM-III criteria, which is similar to Klerman and colleagues’ conclusions
(44) with respect to infrequent panic attacks.
Some studies have investigated the possibility that the subtypes of social phobia may affect quality of life in different ways or degrees. Kessler and colleagues
(73) used National Comorbidity Survey data to compare social phobia characterized by pure speaking fears and by other social fears. Overall, social phobia characterized by pure speaking fears was found to be less persistent, less impairing, and less highly comorbid than social phobia characterized by more generalized social fears. Thus, although even subthreshold social phobia may be associated with a reduced quality of life
(72), these findings suggest that the most pervasive functional impairment and reduced quality of life is seen in persons who suffer from generalized social phobia
(74).
Studies in Clinical Samples
Schneier and colleagues
(40) examined the nature of impairment of functioning in 32 outpatients with social phobia by comparing their scores on two new rating scales—the Disability Profile and the Liebowitz Self-Rated Disability Scale—with those of 14 normal comparison subjects. The Disability Profile is a clinician-rated instrument with items assessing current (i.e., over the last 2 weeks) and most severe lifetime impairment due to emotional problems in eight domains. The Liebowitz Self-Rated Disability Scale is a patient-rated instrument with 11 items assessing current and most severe lifetime impairment due to emotional problems. More than half of all patients with social phobia reported at least moderate impairment at some time in their lives due to social anxiety and avoidance in areas of education, employment, family relationships, marriage or romantic relationships, friendships or social network, and other interests. A substantial minority reported at least moderate impairment in the areas of activities of daily living (such as shopping and personal care) and suicidal behavior or desire to live. On the Liebowitz scale, more than half of all patients reported at least moderate impairment in self-regulation of alcohol use at some time in their lives due to social phobia. Patients with social phobia were rated more impaired than normal comparison subjects on nearly all items on both measures. These findings on the Liebowitz Self-Rated Disability Scale must be considered preliminary, pending further validation of this instrument.
Wittchen and Beloch
(75) measured quality of life and other indices of impairment in a group of 65 subjects with social phobia (with no significant comorbidity) and compared the results with those from a comparison group of individuals with herpes infection. The instruments employed included the Short-Form Health Survey and the Liebowitz Self-Rated Disability Scale. Compared to the matched comparison group, the group with social phobia had significantly lower scores (i.e., worse function) on most of the Short-Form Health Survey scales. Pronounced reductions in self-rated quality of life were found among the patients with social phobia in the domains of role limitation due to emotional problems, social functioning, general mental health, and vitality. Standardized summed scores for the mental health components of the Short-Form Health Survey showed that 23.1% of all subjects with social phobia were severely impaired and 24.6% were significantly impaired compared to only 4.5% of the comparison subjects. The Liebowitz Self-Rated Disability Scale showed that social phobia affected most areas of life but in particular education, career, and romantic relations.
Impact of Treatment on Quality of Life in Patients With Social Phobia
In a 12-week, double-blind, randomized, placebo-controlled trial, Stein et al.
(76) had patients with social phobia (91.3% with the generalized subtype of the disorder) treated with fluvoxamine, an SSRI. At the study’s endpoint, patients taking fluvoxamine (N=34) showed a significantly greater improvement in scores on the work functioning and family life and home functioning items of the Sheehan Disability Scale compared to placebo-treated patients (N=34).
Safren and colleagues
(77) studied quality of life in a group of treatment-seeking persons with social phobia who underwent cognitive behavioral therapy for anxiety disorders in a university clinic. Subjects with comorbidities were not excluded. The instrument employed to measure quality of life was the Quality of Life Inventory
(78), a 17-item scale that assesses a person’s satisfaction in a particular area of life that he or she deems important (such as health, relationships, and work). Patients with social phobia judged their overall quality of life as lower than that of a normative reference group. Quality of life was inversely associated with various measures of severity of social phobia (especially social interaction anxiety), functional impairment, and depression. Subjects with generalized social phobia had significantly lower scores on the Quality of Life Inventory than those with nongeneralized social phobia. Patients showed significant improvement in scores on the Quality of Life Inventory after completion of cognitive behavioral group therapy for social phobia. However, their posttreatment scores on the Quality of Life Inventory remained lower than those of the normative group.
These studies suggest that there may be merit to the continued inclusion of quality-of-life outcome measures in treatment studies of social phobia, although changes may turn out to be more subtle (and perhaps more difficult to measure) than those seen in panic disorder.
Quality of Life in Individuals With OCD
Until 1980 obsessive-compulsive disorder was thought to be rare. The ECA study, however, found lifetime prevalences ranging from 1.94% to 3.29%
(89), although a more recent study places the current prevalence rate in a somewhat lower range
(90). Despite its well-known morbidity, few studies have attempted to measure the impact of OCD on quality of life.
Koran and colleagues
(91) studied quality of life in 60 unmedicated patients with moderate-to-severe OCD using the Short-Form Health Survey and compared their scores with published norms for the general U.S. population and with patients with either depression or diabetes. Patients with OCD had higher median scores on all domains of physical health for quality of life (physical functioning, role limitation due to physical problems, and bodily pain) than patients with diabetes and depression and scored near the general population norm. In contrast, in all the domains of mental health (social functioning, role limitation due to emotional problems, and mental health), the OCD patients’ average scores were well below those of the general population. The diabetic patients’ median scores were similar to those of the depressed patients. The severity of OCD was negatively correlated with scores on social functioning (i.e., the more severe the disorder, the lower the scores). This single study, which remains to be replicated, portrayed OCD as a disorder with a marked negative impact on quality of life.
Quality of Life in Individuals With Generalized Anxiety Disorder
Probably none of the categories of anxiety disorder established in DSM-III has been more difficult to ratify than generalized anxiety disorder. After two waves of substantial revisions in the diagnostic criteria and almost 20 years of continuous research, the uncertainties concerning the nature, boundaries, and clinical implications of this nosologic entity remain as strong as ever. As Roy-Byrne and Katon
(92) pointed out, “there continues to be considerable debate about whether generalized anxiety disorder is a freestanding primary disorder, a prodromal or residual phase of other disorders, a personality trait, or a comorbid condition that modifies the course, treatment response, and outcome of other diseases” (p. 34). There is increasing recognition that comorbidity is a fundamental feature in the nature and course of generalized anxiety disorder. Judd and colleagues
(93) found that 80% of individuals with lifetime generalized anxiety disorder also had a comorbid mood disorder during their lifetime. This finding suggests that the ideal goal of studying “pure,” noncomorbid generalized anxiety disorder may be unattainable.
The ECA study used the DSM-III criteria for generalized anxiety disorder, which emphasize its status as a residual category, and found a reported lifetime prevalence of 4.1% to 6.6%
(94). A total of 58% to 65% of the subjects who had generalized anxiety disorder also had at least one other DSM-III disorder. Persons with generalized anxiety disorder were more often unmarried or divorced. A significantly higher proportion of persons with generalized anxiety disorder than without had received disability benefits during their lifetimes. Even when employed, individuals with generalized anxiety disorder showed indirect evidence of impairment: a significantly higher proportion of them had annual incomes of less than $10,000 (1980 dollars).
The National Comorbidity Survey
(95) used the DSM-III-R criteria for generalized anxiety disorder; these emphasize the presence of excessive and/or unrealistic worry, somatic symptoms, and a duration of at least 6 months. The hierarchical exclusion rules of the DSM-III, which preclude the diagnosis of generalized anxiety disorder if a patient meets the criteria for any other mental disorder, were replaced by a less restrictive rule that required only that the diagnosis of generalized anxiety disorder could not be assigned if it occurred during the course of a mood or psychotic disorder. Generalized anxiety disorder was found to be a relatively rare current disorder (current prevalence of 1.6%) but a more frequent lifetime disorder, affecting 5.1% of the U.S. population aged 15–54 years. The vast majority of persons with generalized anxiety disorder also had at least one other disorder (current morbidity, 66.3%; lifetime morbidity, 90.4%). The most frequent comorbid disorders were affective disorder and panic disorder. “Pure” lifetime generalized anxiety disorder was found to be rare, with a lifetime prevalence of 0.5%. Wittchen and colleagues
(95) found that comorbidity was associated with a significantly greater likelihood of interference with daily activities (51.2% in comorbid generalized anxiety disorder; 28.1% in “pure” generalized anxiety disorder) and made it more difficult to assess the role played by noncomorbid generalized anxiety disorder.
Massion and colleagues
(96) examined the effects of generalized anxiety disorder and panic disorder on the quality of life of a group of patients from the Harvard/Brown Anxiety Disorders Research Program using questions derived from the National Comorbidity Survey. Both groups showed impairment in role functioning and social life as well as low overall life satisfaction. Generalized anxiety disorder was associated with a reduction in overall emotional health. However, the finding that the vast majority of the patients with generalized anxiety disorder had at least one other anxiety disorder led the authors to affirm that “generalized anxiety disorder virtually never occurs in isolation” and made it difficult to assess the role played by noncomorbid generalized anxiety disorder. In summary, these limited data suggest that, although relatively rare, noncomorbid generalized anxiety disorder can be found in a substantial minority of individuals and is associated with important impairment in its own right.
Quality-of-Life Studies of Patients With Anxiety Disorders: Limitations and Prospects
Quality-of-life assessment has been instrumental in exposing the extent and seriousness of anxiety disorders. As summarized previously, both epidemiological and clinical studies clearly delineate the extensive reduction in quality of life associated with anxiety disorders and hint at possible differences between anxiety disorders. Significant degrees of impairment can also be found in individuals with subthreshold forms of anxiety disorders, particularly panic disorder. Preliminary evidence suggests that panic disorder and PTSD may exert a heavier toll on quality of life than other anxiety disorders. Effective pharmacological or psychotherapeutic treatments have been shown to improve the quality of life in patients with panic disorder and social phobia but have yet to be demonstrated for other anxiety disorders.
Several validated generic and specific instruments have been shown to adequately measure quality of life in patients with anxiety disorders, raising the issue of how to select the most adequate instrument for a given purpose. It has been suggested that future studies addressing quality of life should employ a combination of generic and specific instruments to maximize both sensitivity and generalizability
(100). The Short-Form Health Survey is the most extensively tested generic measure and would constitute the natural candidate for an all-purpose instrument. The choice of the accompanying specific instrument should be determined by the specific goals of the study. An alternative approach would be the modular system proposed by Aaronson et al.
(18): the Short-Form Health Survey would constitute the “generic core” to which one or several additional “specific” modules with 10–15 questions could be added. These modules would focus on domains of quality of life that are not captured by the Short-Form Health Survey but that are likely to be affected by the presence of anxiety disorders (such as sleep in PTSD) or by the treatment itself (such as the sexual function of patients medicated with SSRIs). A modular instrument, the Hepatitis Quality of Life Questionnaire
(101), has been recently validated for the assessment of quality of life in patients with chronic hepatitis C; similar measures could be developed for anxiety disorders.
Progress in the field of the assessment of quality of life in anxiety disorders has not been homogeneous. Certain areas of knowledge are in need of further scientific investigation. First, although some disorders such as panic disorder have been reasonably well studied, others such as PTSD have been largely neglected. Second, there are disagreements between epidemiological and clinical findings in some areas that need to be clarified. The causes of this disagreement are open to debate and will require further study
(102). Third, to our knowledge, only a handful of studies have attempted to compare the impact of different anxiety disorders on quality of life. Fourth, the original goal for which the concept of quality of life was first adopted in clinical research was to compare outcomes between different treatment modalities. However, we found only 11 studies—eight in panic disorder, two in social phobia, and a small pilot study on PTSD—that attempted to assess the impact of treatment on the quality of life in patients with anxiety disorders. This is surprising considering that unlike other areas of medical research, mental health has few physiological variables to employ as outcome measures and would likely benefit from an approach that has proved successful in oncology and cardiology. It is likely that therapies that are equivalent in terms of the reduction of symptoms may be qualitatively or quantitatively dissimilar with respect to effects on quality of life. Knowledge of these differences may lead to a more informed choice of treatment modality for a particular disorder and, perhaps, for individual patients. In this area, much additional research is needed.
Despite the growing number of studies undertaken during the past 15 years, the investigation of quality of life in individuals with anxiety disorders is still in its infancy. Nevertheless, the studies conducted to date almost uniformly portray a picture of anxiety disorders as illnesses that markedly compromise quality-of-life and psychosocial functioning in several functional domains. It is hoped that these findings will translate into a more accurate public (and health care policy) view of anxiety disorders as serious mental disorders worthy of further research and appropriate health care expenditures. Finally, outcome studies that incorporate quality-of-life indices will further inform us as to the efficacy of existing and new treatments to lessen the burden of illness attributable to these disorders.