Clinical Trial: Pretreatment Patient Characteristics
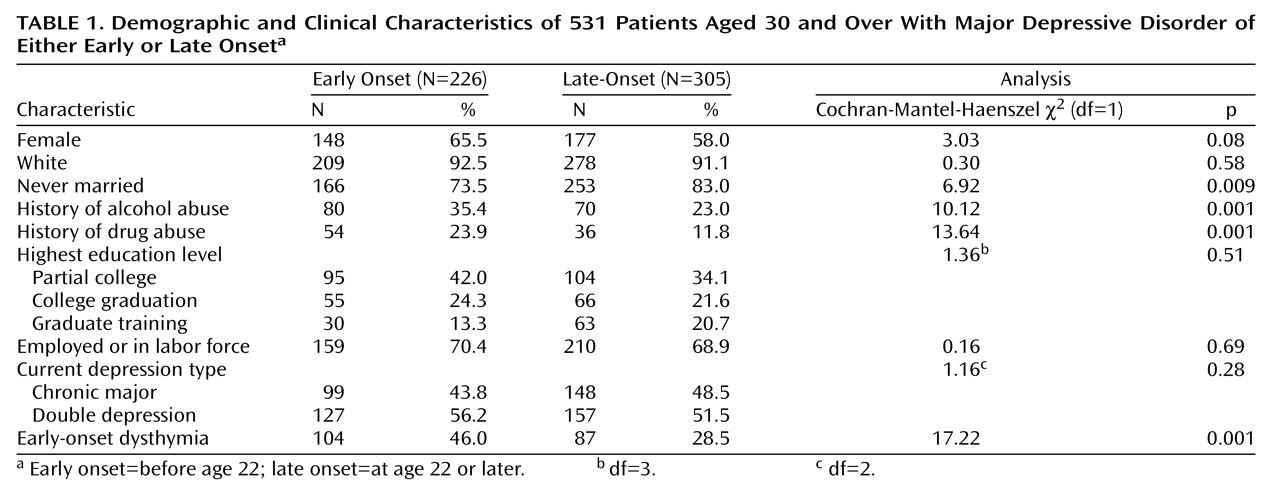
Of the 635 trial subjects, 531 were age 30 and over at baseline. Among this subgroup, the 226 patients (42.6%) with early-onset major depressive disorder differed in a number of important ways from the 305 patients (57.4%) with late-onset major depressive disorder. As shown in
Table 1, subjects with early onset of major depressive disorder were more likely to be female, to have never married, and to have had a history of alcohol or drug abuse. The early-onset patients were also significantly younger than those patients with late-onset major depressive disorder (mean=41.3 years [SD=7.6] versus 45.7 years [SD=8.4], respectively) (F=6.26, df=1, 529, p<0.001). There was no significant difference between early- and late-onset subjects in employment status, educational attainment, or current type of depression, and the two groups were similar in terms of baseline severity of depression as measured by their Hamilton depression scale scores (mean=24.8 [SD=5.3] and 24.8 [SD=5.6], respectively) (F=0.07, df=1, 529, p=0.95). Almost half (46.0%) of the patients with early-onset major depressive disorder also had a history of early-onset dysthymia, whereas early-onset dysthymia occurred in only 28.5% of the patients with late-onset major depressive disorder.
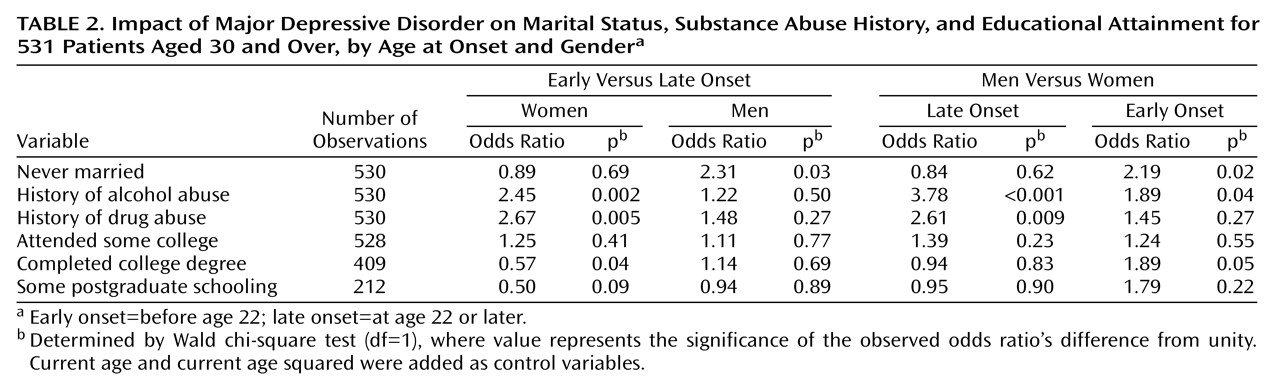
Levels of educational attainment, whether the patient ever married, and histories of alcohol or drug abuse depended in part on age. To account for possible age confounds, and to permit identification of gender-specific impacts, multivariate logistic regressions were performed. Results of these logistic regressions, expressed in the form of odds ratios, are given in
Table 2.
The impact of early-onset major depressive disorder on whether the patient had never married varied by gender. The likelihood of women with early-onset depression never having married was not significantly different from that of women whose onset was later. However, men with early-onset depression were more than twice as likely to have never married than were men whose depressive onset occurred later. While men and women with late-onset major depressive disorder did not differ from each other, men with early-onset depression were more than twice as likely to have never married than were women with early-onset depression. For men, the impact of early-onset major depressive disorder was most apparent on this simple index of intimate relationships.
Impacts of early-onset major depressive disorder on substance abuse also varied by gender. Women with early-onset major depressive disorder were much more likely than those with late-onset depression to have a history of alcohol or drug abuse. Age at onset did not significantly affect the risk of having a history of alcohol or drug abuse for men. The propensity for men to have a history of alcohol or drug abuse was generally larger than that for women. However, although men with late-onset major depressive disorder had an almost fourfold greater risk of alcohol abuse history than women with late-onset depression, the male-female relative risk dropped by about half when both genders had early-onset major depressive disorder.
Although the likelihood of having attended college was unaffected by age at onset, for those who attended college, early-onset major depressive disorder negatively affected the probability of graduating, particularly for women. Women with early-onset major depressive disorder were about half as likely to obtain a college degree as their older-onset counterparts. Further, within the early-onset group, men were almost twice as likely as women to graduate. This large negative impact of early-onset major depressive disorder for women appeared to continue beyond college into graduate studies, as women with early-onset major depressive disorder were half as likely as those with late-onset depression to seek postgraduate training. For men, however, the likelihood of attempting a postgraduate degree was unaffected by age at onset.
In terms of the six domains of psychological functioning measured at baseline by the Short-Form Health Survey, subjects with early- and late-onset major depressive disorder scored significantly lower than the “normal” population in each of the domains (results not shown, one-tailed ANOVA, df=1, 529, all F>20 and p<0.001). Between the early- and late-onset patients, scores were significantly different only for the domains of physical functioning (two-tailed ANOVA, F=6.60, df=1, 529, p=0.01) and work/daily activities—physical (two-tailed ANOVA, F=4.93, df=1, 529, p=0.03), with the late-onset patients having scores on both that indicated greater impairment. Further details are available upon request from the corresponding author (L.M.K.).
Clinical Trial: Treatment Response
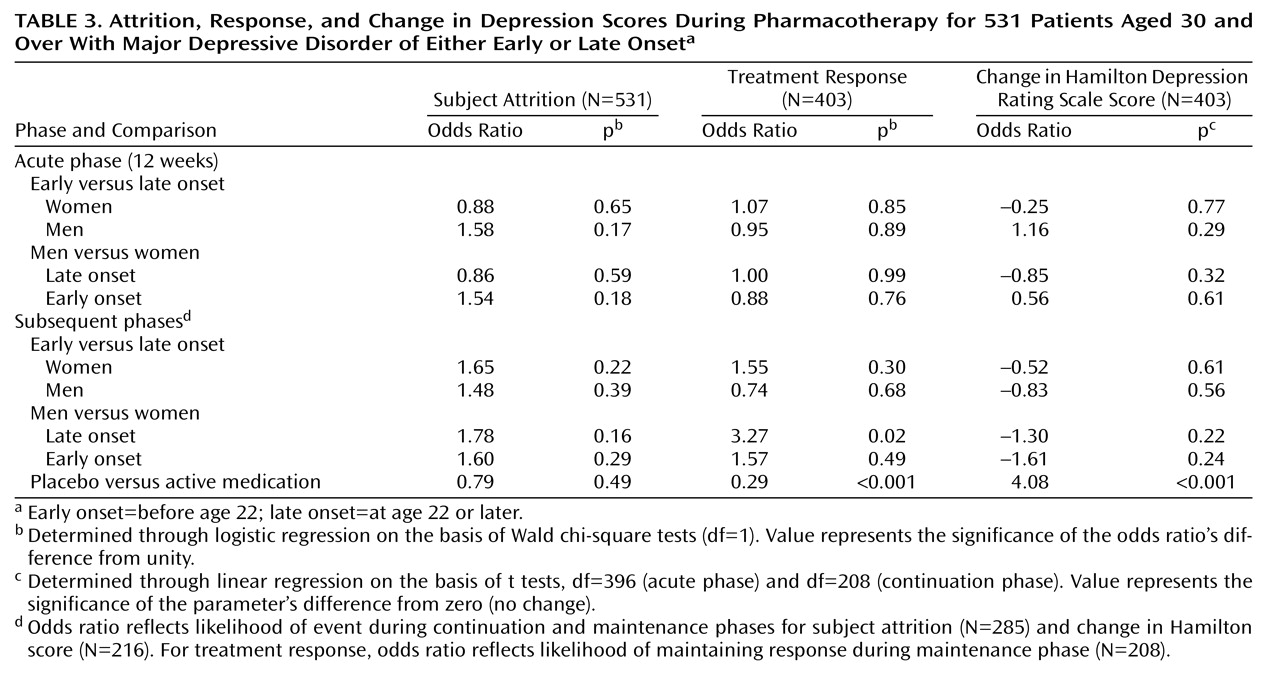
Symptomatic treatment responsiveness was independent of age at onset, both in terms of subject attrition during phases of the trial and treatment responsiveness for those who completed a trial phase (
Table 3). The likelihood of dropping out during the acute phase, or of dropping out during the continuation or maintenance phase, was not significantly affected by age of major depressive disorder onset or gender; no odds ratio significantly differed from unity. For patients who completed the acute phase, the probability of achieving a satisfactory acute-phase therapeutic response was independent of age at onset. Among the acute-phase responders, age of major depressive disorder onset did not affect the likelihood of maintaining the therapeutic response during the maintenance phase of the trial, although among the subjects with late-onset major depressive disorder, the likelihood was significantly greater for men than for women. The likelihood of patients randomly assigned to receive placebo maintaining a therapeutic response during this trial phase was only one-quarter that of patients randomly assigned to receive sertraline.
Least squares regression estimates, where the dependent variable is the change in Hamilton depression scale score since the beginning of that trial phase (negative implies improvement), and with beginning-phase Hamilton depression scale score as an additional regressor, indicate that the amount of change in Hamilton depression scale score was unaffected by gender or age of major depressive disorder onset. However, during the maintenance phase, being randomly assigned to receive placebo in place of sertraline resulted in a mean 4-point worsening in score on the Hamilton depression scale.
The Short-Form Health Survey results (not shown) suggest that therapeutic responders returned to levels of psychosocial functioning generally comparable to community norms, regardless of major depressive disorder age at onset. In four of the six domains (general health, pain, work/daily activities—physical, and interpersonal functioning), therapeutic responders after the 12-week acute phase were insignificantly different from normal community populations (one-tailed ANOVA, df=1, 529, all F≤1.17 and p≥0.14). In the physical functioning domain, late-onset subjects had slightly but significantly lower scores than the community subjects (one-tailed ANOVA, df=1, 529, F=6.40, p=0.006). In the work/daily activities—emotional domain, both early and late-onset subjects had slightly but significantly lower scores than the community subjects (one-tailed ANOVA, df=1, 529, F=3.25 and F=3.23, p=0.04 for both). In each of the six domains, however, the mean scores of the early- and late-onset patients were not significantly different from each other (two-tailed ANOVA, df=1, 529, all F≤2.96 and p≥0.09). Further details are available upon request from the corresponding author.
Education and Earnings Impacts of Lost Human Capital
The impact of early-onset depression on future earnings arise in our framework because of associated reductions in educational attainment. Trial data indicated that for men, early-onset major depressive disorder did not affect subsequent educational attainment. For women, however, the likelihood of completing a college degree for those attending college was only 57% as high for those with early- versus late-onset major depressive disorder, and for college degree recipients, the odds for pursuing postgraduate training were only 50% as high.
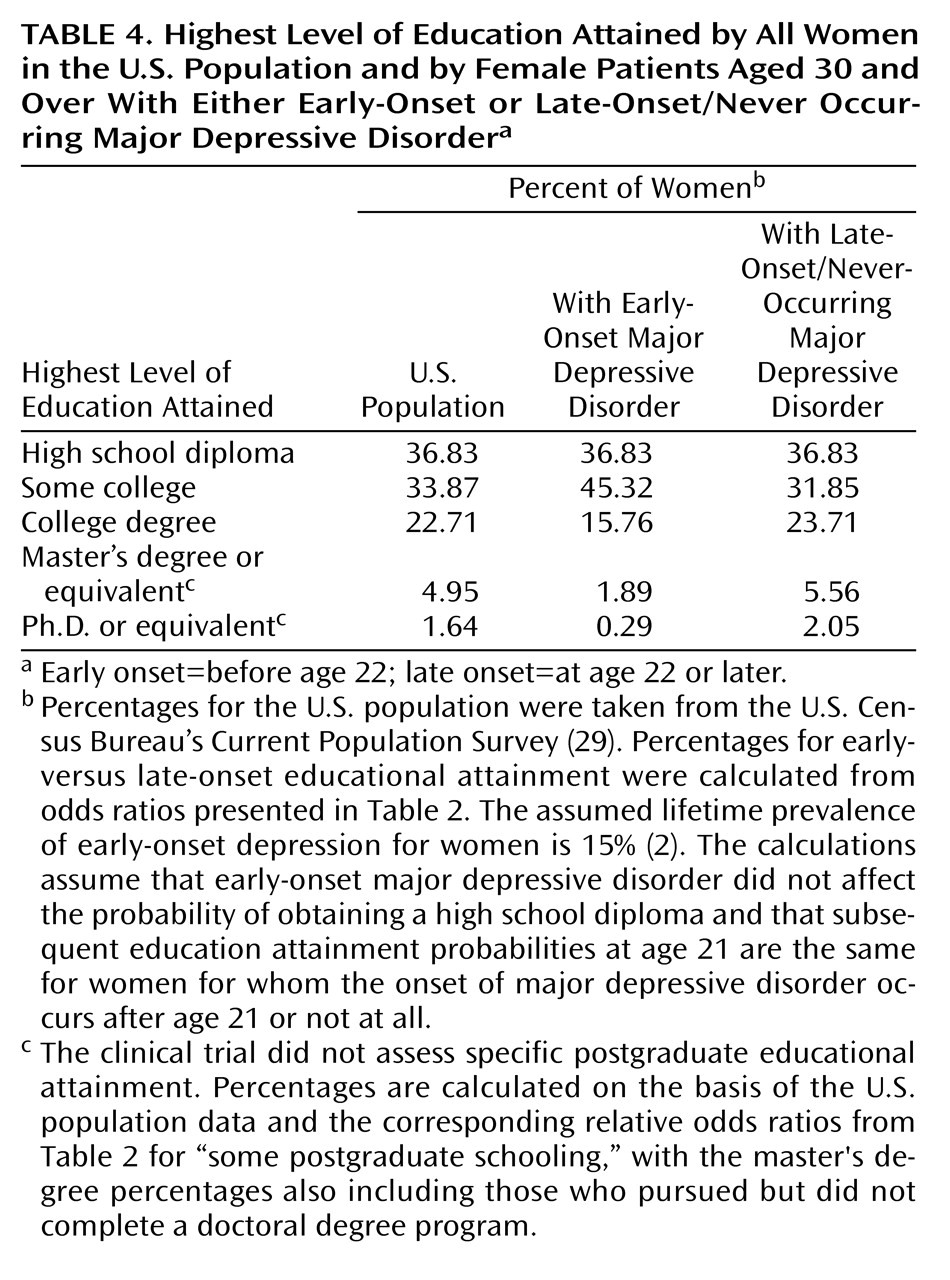
As seen in the final two columns of
Table 4, in relation to the female U.S. population in 1995, early-onset major depressive disorder resulted in considerable reductions in highest educational attainment, i.e., in lost human capital. More women with early- than late-onset major depressive disorder attended college but did not complete a college degree program, which resulted in a smaller proportion of early-onset women having a college degree as their highest level of educational attainment.
To assess the earnings impact of reductions in human capital accumulation associated with early-onset major depressive disorder for women, we related 1995 earnings of U.S. women ages 19–70 to levels of educational attainment. Although not shown here, consistent with other labor market studies
(30), we found that annual earnings are greater and peak at older ages with successive increases in educational attainment.
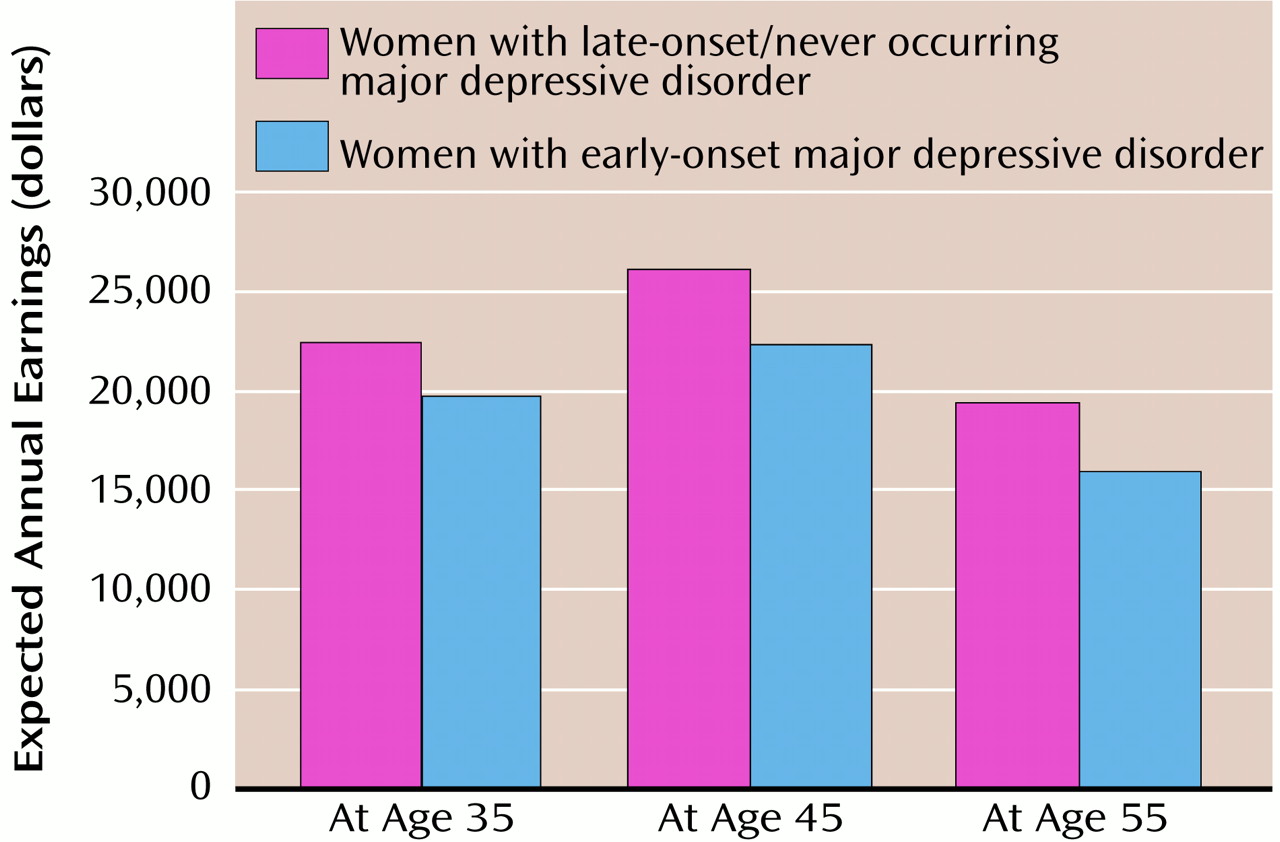
When these age at onset, educational attainment, and income data are combined, they reveal significant declines in expected future annual earnings for women experiencing early-onset versus late-onset/never-occurring major depressive disorder. As shown in
Figure 1, expected annual earnings at age 35 for two women 21 years of age in 1995 would be $22,461 for the woman with late-onset/never-occurring major depressive disorder but only $19,795 ($2,666, or 11.9% less) for the woman with early-onset major depressive disorder. At age 45, the expected annual earnings gap widens to $26,071 versus $22,341 ($3,730, or 14.3% less), respectively, and at age 55 expected annual earnings are $19,415 versus $15,937 ($3,478, or 17.9% less). We emphasize that these are annual decrements. Were they to be summed over a lifetime in the workforce, these decrements would be more substantial. Thus, early-onset major depressive disorder has considerable consequences for the expected earnings of women.