Winter birth is a widely replicated risk factor for schizophrenia
(8). Some studies have found that winter-born patients had distinguishing clinical or demographic features, including paranoid subtype in men and a generally more benign course of illness
(9–
16). The clinical characteristics of winter-born patients suggested that patients with deficit schizophrenia
(17), who generally have a poor outcome
(18,
19), were likely not to have an excess of winter births. In two study groups that were not epidemiological samples, we noted an excess of summer births in patients with deficit schizophrenia, which was confirmed in epidemiological studies of incident cases of psychosis
(20,
21) and in two studies of case prevalence
(22,
23).
Method
Dumfries and Galloway is a geographically well-defined area in southwestern Scotland. It has a stable population of around 147,000, of whom 99.5% are Caucasian. Psychiatric services are provided through one government-sponsored agency, and there is little or no private health care.
All patients were identified who had come into contact with the psychiatric services of Dumfries and Galloway between the years 1979 and 1998 and who had been given a clinical diagnosis of schizophrenia; schizoaffective disorder; delusional disorder; mania; drug-induced psychotic disorder; or acute, transient, or unspecified psychotic disorder. ICD-9 was used to code diagnoses from 1979 to March 1996, when the clinical services began to use ICD-10. Patients were excluded if they did not reside in Dumfries and Galloway at the time of first clinical contact. The list of possible subjects was derived from two sources: 1) data for all inpatients, held centrally in Edinburgh by the Information and Statistical Division of the Scottish Office, and 2) locally held registers of outpatients, domiciliary visits, and “after hours” referrals. This study was approved by the Dumfries and Galloway Health Board Research Ethics Committee.
The Operational Checklist for Psychotic Disorders
(34) was completed by using case records, correspondence, and all medical, nursing, social work, and occupational therapy notes. The instrument is a symptom checklist with 90 items relating to mental status and psychiatric history. It has a glossary with scoring instructions for each item and was developed with case note review in mind.
Two raters (J.A. and G.M.) completed the Operational Checklist for Psychotic Disorders for each patient for the year after initial contact with psychiatric services. These summaries allowed comparison among patients on the basis of similar information, irrespective of year of contact. Case notes were examined in random order of date of contact, and raters were blind to the clinically coded diagnosis. There was good interrater reliability for the ICD diagnosis of schizophrenia
(33). The Operational Checklist for Psychotic Disorders was also used to generate DSM-IV and Research Diagnostic Criteria
(35) diagnoses by means of the associated computer algorithm OPCRIT, version 3.4
(34).
There were 464 patients with a first episode of psychosis during the study period. Patients with an OPCRIT-based DSM-IV diagnosis of schizophrenia, schizophreniform disorder, or psychosis not otherwise specified were included in the present analyses
(36). A total of 342 patients met these criteria: 113 with schizophrenia, 89 with schizophreniform disorder, and 140 with psychosis not otherwise specified.
We developed the Proxy for the Deficit Syndrome
(20–
23,
37–40) to identify patients with deficit schizophrenia in data sets in which the Schedule for the Deficit Syndrome
(17) was not applied. The proxy was initially developed for use with instruments such as the Brief Psychiatric Rating Scale and the Scale for the Assessment of Negative Symptoms, which quantify the severity of symptoms on 6- and 7-point scales. In contrast, the Operational Checklist for Psychotic Disorders records symptoms on 2- or 3-point scales, and many of the items that could be used with the Proxy for the Deficit Syndrome had little variance. Consequently, we used an algorithm based on the criteria for deficit schizophrenia
(17) to define the deficit and nondeficit groups. Patients were categorized as having deficit schizophrenia if they 1) had restricted and/or blunted affect (two separate items in the Operational Checklist for Psychotic Disorders) but 2) did not exhibit dysphoria (a separate item in the Operational Checklist for Psychotic Disorders)
(17,
37,
41). As in the studies in which the Proxy for the Deficit Syndrome was used, we tested the validity of assignments to the deficit and nondeficit groups by comparing their features to those of groups defined by using the Schedule for the Deficit Syndrome. In the validity testing, the deficit group did not differ significantly from the nondeficit group in age or in the severity of delusions, hallucinations, or formal thought disorder but had more severe negative symptoms, less severe dysphoria, poorer premorbid function, and a more insidious onset of the disorder
(18,
24,
38,
39). Another research group has used a similar approach to define a deficit group
(42).
This approach yielded 65 deficit patients (19%) and 277 (81%) nondeficit patients. The validity testing largely confirmed that these groups had clinical features that were similar to those diagnosed by using the Schedule for the Deficit Syndrome. The validity was further supported by the similarity between the prevalence in this deficit group and the prevalence estimate in another epidemiological study of first-episode schizophrenia
(43), in which structured interview data, rating scales filled out by the patient, and hospital records were reviewed to make the deficit or nondeficit categorizations.
To test the summer-birth hypothesis, we used logistic regression models with summer birth as the dependent variable. To make our results comparable to those of previous studies of summer birth and deficit schizophrenia
(20–
23), we used four definitions of summer: May to August, June to August, June-July, and July-August. Positive psychotic symptoms were used as covariates because psychotic symptoms are important sources of secondary negative symptoms and may contribute to miscategorizations. Earlier factor analysis studies of the symptoms of schizophrenia provided the basis for combining hallucinations and delusions as one variable and for considering disorganization as a separate variable
(44–
46). In the logistic regression procedures, the hallucination and delusion items in the Operational Checklist for Psychotic Disorders were recoded so that patients with a history of at least 1 month’s duration of either symptom were given a score of 2; those with a definite history of either symptom, but of a duration of less than 1 month, were given a score of 1; and those without a history of either symptom were given a score of 0. A single disorganization score was derived by using the same strategy for the items measuring positive formal thought disorder and incoherence. Age and gender were also included as independent variables. Six patients were excluded from the season-of-birth analysis: for two patients information on the month of birth was not available, and four patients were born in the Southern Hemisphere.
In previous studies
(20–
23), negative symptoms were not related to summer birth. We examined the relationship of summer birth to restricted affect (the negative symptom used to delineate the deficit and nondeficit groups) using four logistic regression procedures, with restricted affect in the place of deficit/nondeficit categorization as an independent variable. The other independent variables discussed earlier were also used.
We also tested the hypothesis that the relative frequency of summer births in the deficit group differed from that among all births in Dumfries and Galloway, using chi-square analysis and the four definitions of summer. Patients in the incidence study were born between 1891 and 1982 (the average year of birth was 1949). However, data on all births in Dumfries and Galloway by month were not available for the period before 1974. We compared summer births of the deficit group to those among all births in the area in 1974, using data from the General Register Office for Scotland in Edinburgh.
Because the data for all births were restricted to 1974, there was a possibility that any difference between deficit births and all births was due to a secular trend and did not reflect a consistent association between risk of deficit schizophrenia and summer birth. To assess this issue, we examined the pattern of deficit versus all births within each of two epochs, defined by a point in 1958 that approximately divided the deficit group in half, i.e., we made a median split of the deficit group based on year of birth and compared deficit births to all births within each of the two epochs.
Because the percentage of subjects with a diagnosis of psychosis not otherwise specified was relatively high, we also examined the association of summer birth and deficit schizophrenia after excluding the subjects with psychosis not otherwise specified.
Results
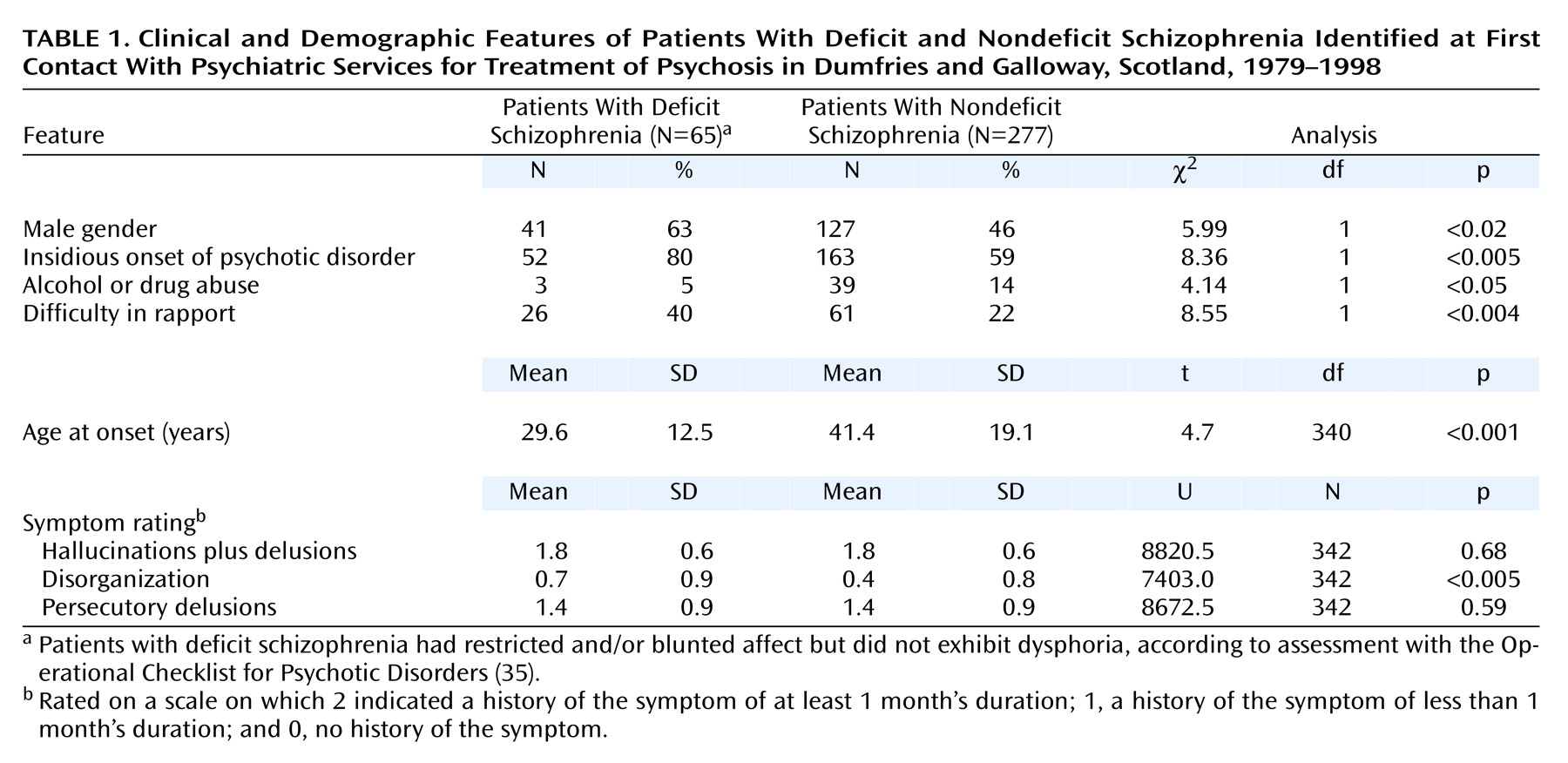
In general, the differences and similarities of the deficit and nondeficit groups were similar to those of such groups identified by using the Schedule for the Deficit Syndrome. By definition, the deficit group had significantly greater blunted affect and significantly less severe dysphoria than the nondeficit group; in addition, the two groups did not differ significantly relative to hallucinations plus delusions, and the deficit group had a significantly greater percentage of male subjects than the nondeficit group. As noted earlier, the prevalence of deficit schizophrenia was also similar to that in another epidemiological study of incident cases of psychosis
(43). Because the deficit group also had significantly more severe disorganization than the nondeficit group and was significantly younger (
Table 1), these two variables were used as covariates in the logistic regression procedures.
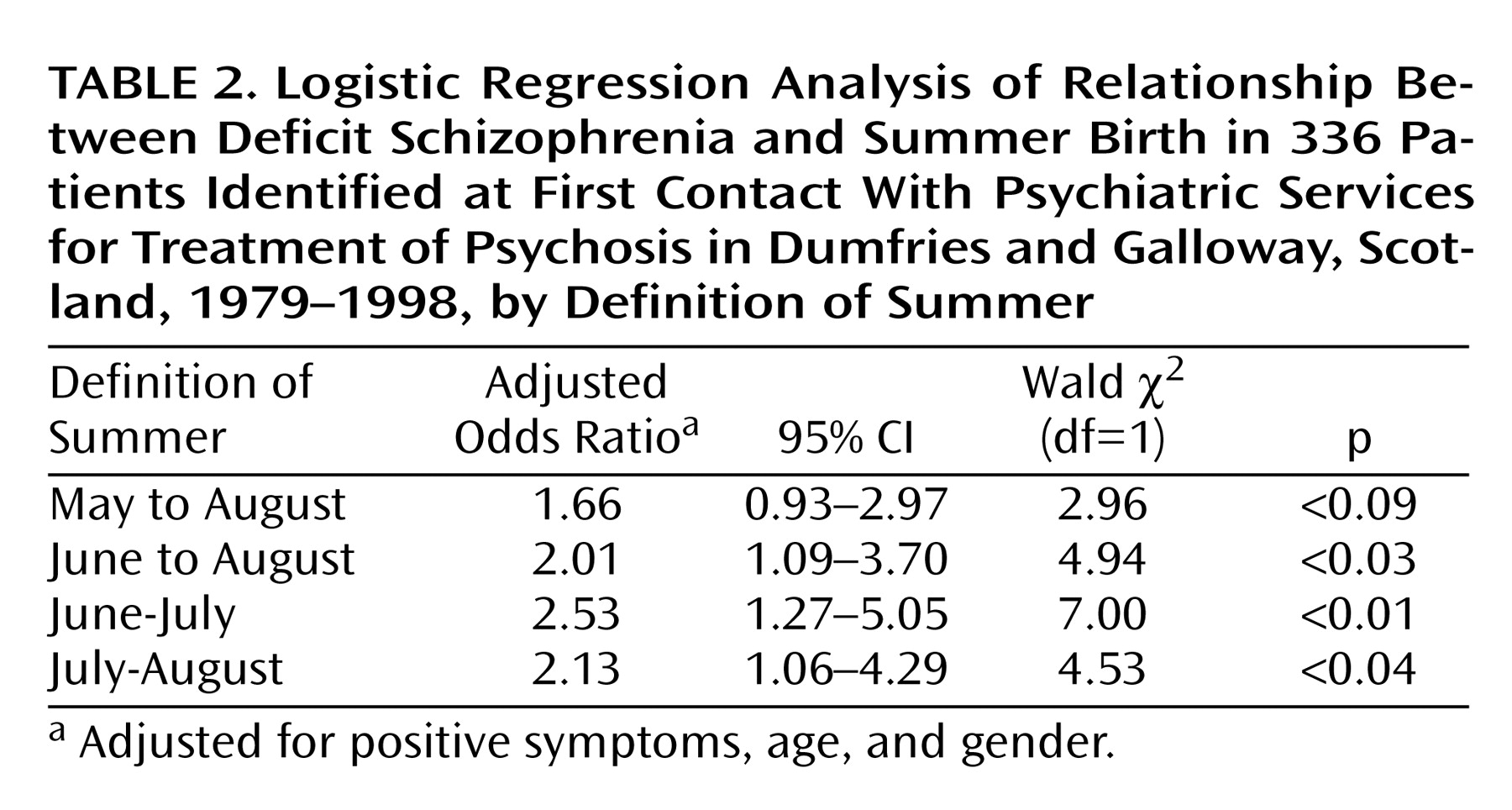
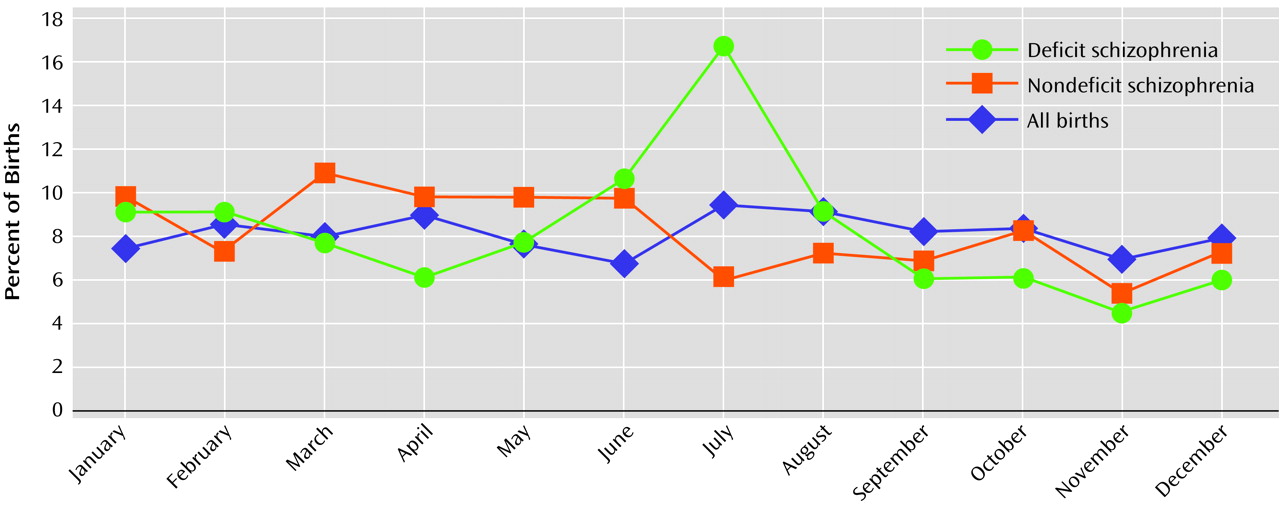
Figure 1 shows the percentages of births that occurred in each month in the deficit and nondeficit groups and among all births. In the multivariate logistic regression analyses, the deficit group had a significant association with birth in June to August, June-July, and July-August (
Table 2). More deficit than nondeficit patients were born from May to August, but this difference was not significant (
Table 2). No other variable was significantly associated with summer birth in any of the regression models. In contrast, the negative symptom that was used to define the deficit group (restricted affect) was significantly associated with just one definition of summer, June-July (data available on request from authors).
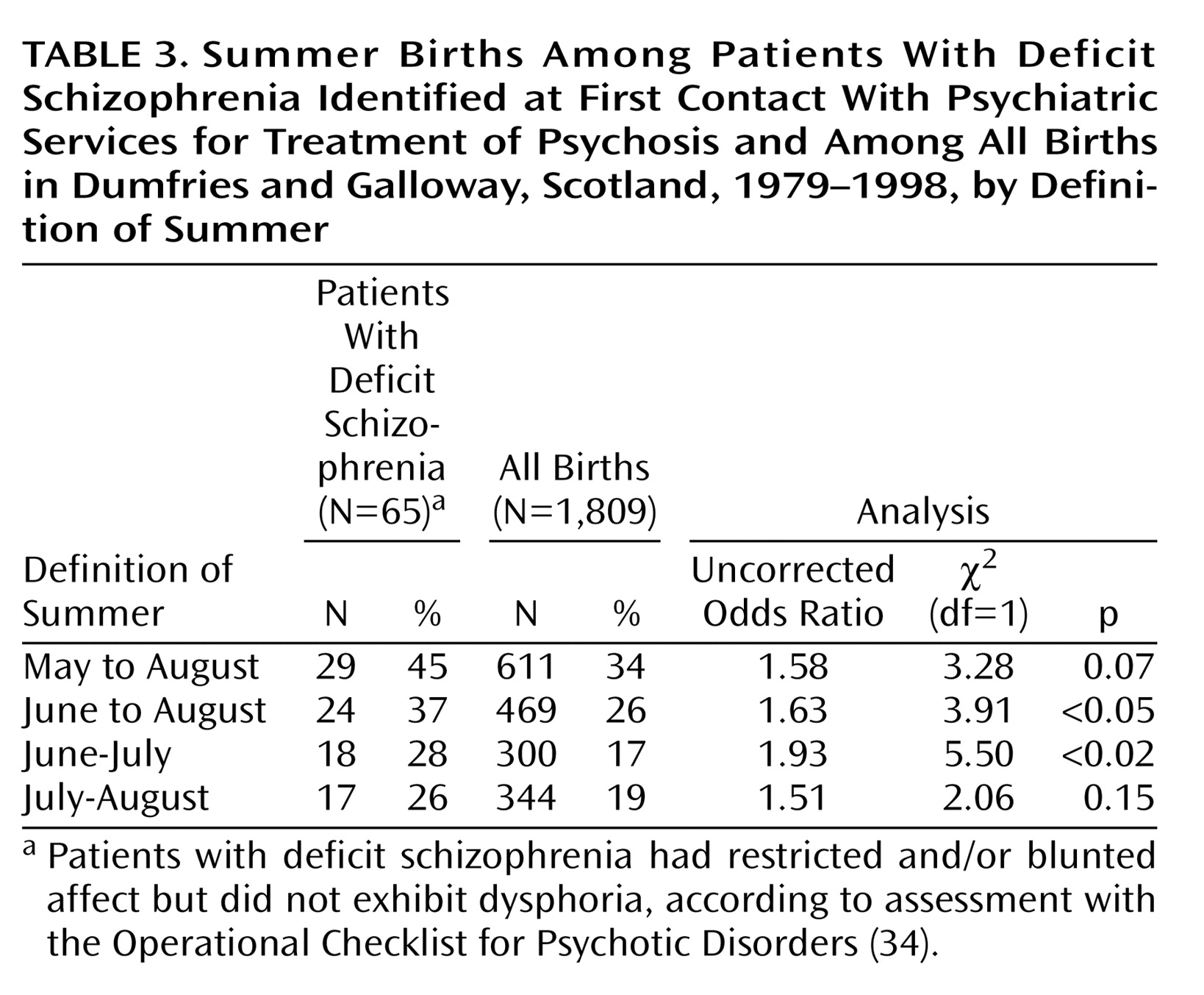
The deficit group also had a significantly higher percentage of births in June to August and June-July, compared to all births in Dumfries and Galloway (
Table 3). In the median split analysis, an excess of summer births was apparent in the deficit group, compared to all births, in each of the two epochs (data not shown).
When subjects with a diagnosis of psychosis not otherwise specified were excluded, an excess of summer births was still apparent in the deficit group (data not shown).
Discussion
In an epidemiological study of incident cases of psychosis in southwestern Scotland, we replicated the association of deficit schizophrenia with summer birth. This association was present within schizophrenia, i.e., in a comparison between deficit and nondeficit schizophrenia patients, after accounting for clinical and demographic features. In contrast, within schizophrenia, the negative symptom measure (as distinguished from the deficit categorization) had a weaker association with summer birth. The deficit schizophrenia group also had an excess of summer births in comparison to all births in the same region.
The validity of our results depends on the validity of the deficit and nondeficit categorizations. Although our current approach to distinguishing deficit and nondeficit groups was somewhat different from the approach we used previously, the characteristics of the two groups were similar to those of groups identified with the Schedule for the Deficit Syndrome and the Proxy for the Deficit Syndrome
(17–
32). The association with summer birth remained after accounting for the variance due to other potentially confounding clinical and demographic factors (including two variables for which the deficit group did not have the desired results in the validity testing). Any miscategorizations due to this method seem more likely to result in a failure to find an association than in a false positive association.
Because we restricted our analyses to patients in their first year of treatment, the subjects included a relatively high percentage of patients with psychosis not otherwise specified. We restricted the data analyses to the first year to approximate an incident case sample and to avoid bias due to survival in the sense of biased mortality and in the sense of survival as a case, i.e., chronic illness. In addition, when patients with a diagnosis of psychosis not otherwise specified were excluded, an excess of summer births was still apparent in the deficit group (data not shown). The lack of follow-up, with confirmation of diagnoses, is a limitation of our study, and it is possible that changes in diagnoses might have changed our findings. However, the multiple replications of the summer-birth effect
(20–
23,
47) suggest that this limitation did not create the association reported here.
Another limitation is that we did not have an ideal nonpatient comparison group, as the earliest year for which data on all births were available was 1974. In our first report on summer birth, there was also a suggestion of a difference between births in the deficit group and all births in the same region
(20). We have also found a significant difference between deficit births and all births in an epidemiological nonpatient comparison group in data from the Epidemiological Catchment Area study, which was conducted in five centers in the United States
(22), and in a study of incident cases of psychosis from Cantabria in northern Spain
(47). The consistency of the findings of the present study with those of other studies suggests that the shortcomings of the comparison groups have not resulted in a false positive association.
A measure of negative symptoms had a weaker association with summer birth than did the deficit versus nondeficit categorization. Negative symptoms were also not associated with summer births in previous studies
(20–
23). Negative symptoms and the deficit criteria define groups that overlap substantially but are not synonymous, and these two measures also have different correlates
(19,
27,
37). The ability to detect an association—or in the case of the positive psychotic symptoms, a failure to detect an association—is limited by the reliability of the variables of interest. However, the consistency of the studies of carefully validated deficit groups and summer birth, despite the use of a variety of scales, suggests that this issue did not distort our results.
Other studies have also suggested that season of birth is related to clinical characteristics. A review of the literature on season and schizophrenia
(9) concluded that, on average, winter-born schizophrenia patients have a relatively benign disease compared to those born at other times of the year. In two subsequent studies, winter birth was found to be associated with the paranoid subtype in men
(10,
11), which is a relatively benign form of illness. The deficit syndrome is associated with a relatively severe form of illness
(18,
19,
37); thus, our present results are consistent with the previous studies.
The replicated association between summer birth and deficit schizophrenia is not consistent with the interpretation that deficit/nondeficit differences are found because the deficit group is at the extreme end of a severity spectrum, i.e., that the deficit group has a more severe form of the same pathophysiology found in nondeficit schizophrenia. Deficit subjects do not have a more severe form of the winter-birth excess, which is associated with schizophrenia as a whole, but a different risk factor, i.e., summer birth. It is likely that the winter-birth effect is the one that has been noticed in previous studies of schizophrenia because the deficit versus nondeficit categorization has not been made and the prevalence of nondeficit schizophrenia is greater than that of deficit schizophrenia. Not only is the widely replicated winter-birth phenomenon probably restricted to the nondeficit group, but the effect size may be greater than previously thought.
The identification of a season-of-birth risk factor for separate subgroups of schizophrenia may have several implications. For instance, maternal exposure to certain viral infections, most often influenza, has been linked to the development of schizophrenia
(48–
50). As infection appears to increase the risk of schizophrenia only if it occurs during the second trimester, and such infections are generally more prevalent during the winter, subjects with schizophrenia as a result of exposure to such infections may have an excess of spring or summer births. In future studies of viral infections and risk of schizophrenia, it would be desirable to examine deficit and nondeficit groups separately. Other proposed explanations of seasonal variation of births, besides seasonal variation in infections, include decreased exposure to sunshine, seasonal variations of exposure to environmental toxins, and seasonal variations in nutrition
(51).
The apparent double dissociation between season of birth and deficit versus nondeficit categorization is consistent with the evidence that deficit and nondeficit schizophrenia have differences in pathophysiology
(52). Use of the deficit versus nondeficit categorization in future studies may provide additional insight in the search for nongenetic risk factors for schizophrenia.