Demographic Characteristics
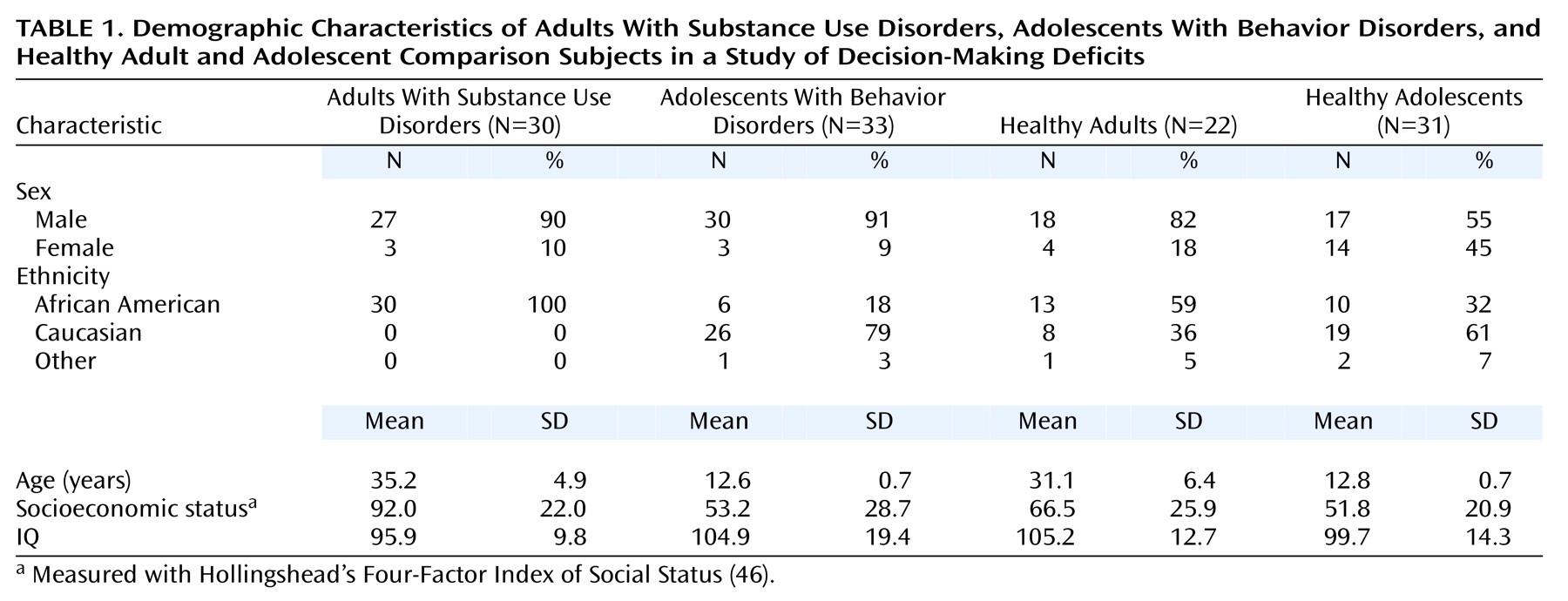
The study group comprised 52 adults (22 healthy comparison subjects and 30 adults with substance use disorders) and 64 adolescents (31 healthy comparison subjects and 33 adolescents with an externalizing behavior disorder) (
Table 1). Data from two adult comparison participants were removed from an analysis published previously
(9) because their Gambling Task scores indicated that they did not engage in the task.
Behavior disorders in adolescents consisted of ADHD without comorbidity (N=21), conduct disorder without comorbidity (N=5), and ADHD comorbid with a history of mood disorder without acute symptoms (N=7, four with unipolar depression, two with dysthymia, and one with adjustment disorder). An ANCOVA, with IQ as covariate, showed no significant differences in Gambling Task scores among the three groups of adolescents with behavior disorders. Thus, data for the three groups were analyzed together, to represent a single group of at-risk adolescents. About half of the subjects with behavior disorders (18 of 33) were treated with stimulants and were tested 48 hours after stimulant discontinuation. Performance on the decision-making task (net scores) and on the Wisconsin Card Sorting Task did not differ between the 18 adolescents who discontinued treatment and the 15 adolescents who were not treated with stimulants (net score, week 1: F=0.70, df=1, 30, p=0.41; net score, week 2: F=0.03, df=1, 30, p=0.86; Wisconsin Card Sorting Task: 0.01<F<0.74, df=1, 30, 0.40<p<0.93). Nine adolescents with behavior disorders were also receiving tricyclic antidepressants (N=2), bupropion (N=4), or sertraline (N=3). These medications were not discontinued because their longer half-lives would have required a longer discontinuation period. The performance scores of these nine adolescents did not differ significantly from that of the other 24 adolescents with behavior disorders (net score, week 1: F=0.02, df=1, 30, p=0.88; net score, week 2: F=1.72, df=1, 30, p=0.20; Wisconsin Card Sorting Task: 0.34<F<2.34, df=1, 30, 0.14<p<0.56).
Most adults with substance use disorders (28 of 30) used an average of 2.5 g/week (SD=0.7) of cocaine, more than half (19 of 30) used an average of 253 mg/week (SD=76) of heroin, and 29 used marijuana, alcohol, and/or nicotine weekly. The average duration of use was about 7 years for the cocaine and heroin users, and between 14 and 17 years for the users of marijuana, alcohol, and cigarettes. None of the comparison subjects had ever used cocaine or heroin or were currently smoking marijuana or nicotine cigarettes.
Data on the subjects’ age, sex, ethnicity, socioeconomic status, and IQ are listed in
Table 1. The healthy adolescents and the adolescents with behavior disorders were similar in age, whereas the healthy adults were younger than the adults with substance use disorders (t=2.56, df=50, p=0.01). Socioeconomic status was lower in the adults than in the adolescents (F=35.16, df=1, 113, p<0.0001) and lower in the adults with substance use disorders than in the healthy adults (t=3.81, df=50, p=0.0004). There was no significant difference in socioeconomic status between the healthy adolescents and the adolescents with behavior disorders. Finally, IQ was significantly higher in the healthy adults than in the adults with substance use disorder (t=–2.97, df=50, p=0.005) and significantly lower in the adults with substance use disorders than in the adolescents with behavior disorders (t=–2.36, df=48.4, p=0.02), but there was no significant difference in IQ between the healthy adolescents and the adolescents with behavior disorder or between the healthy adolescents and the healthy adults.