Obsessive-compulsive disorder (OCD) is characterized by recurrent, persistent, and intrusive thoughts or images that cause anxiety or distress (obsessions) and repetitive behaviors or mental acts aimed at reducing this distress or anxiety (compulsions). Patients recognize that these obsessions and compulsions are unreasonable and products of their own mind. Once considered rare, recent epidemiological data suggest prevalence rates of OCD from 1.5% to 3%
(1,
2). In general, OCD symptoms can best be managed with selective serotonin reuptake inhibitors (SSRIs) or behavioral therapy. The selective response of OCD patients to SSRIs has led to the hypothesis that changes in the central serotonergic systems may be the mechanism by which these compounds exert their effect
(3). Direct evidence that serotonergic perturbations are implicated in the neurobiology of OCD, however, is sparse. Serotonergic pharmacological challenges and CSF metabolite studies have yielded data that are too inconsistent—or too open to different interpretations—to serve as a valid basis for dissecting the neurobiology of OCD
(3–
5). Growing evidence that atypical antipsychotics, such as risperidone and quetiapine, may augment the response to SSRIs in patients with refractory OCD and those with comorbid tics, as well as studies showing an exacerbation of symptoms after administration of a dopamine agonist, would seem to point to an increase in dopaminergic system activity in OCD
(6,
7). The role of dopamine in stereotypic behaviors in animal models and the preclinical evidence of important interactions between serotonergic and dopaminergic systems further strengthen the putative role of dopamine in OCD
(8,
9). Studies examining the concentration of the dopamine metabolite homovanillic acid and the dopaminergic regulation of the hypothalamo-pituitary-adrenal axis lend further support to a possible role of dopamine in the pathophysiology of OCD
(10,
11). Neuroimaging studies have been very influential in shaping neurobiological models of OCD. Converging data have implicated a network of brain regions, including the orbitofrontal cortex, striatum, and thalamus, in the pathophysiology of OCD. Most regions of the putatively involved network in OCD are densely innervated by serotonergic or dopaminergic neurons
(12). However, despite the advent of several ligands for dopaminergic and serotonergic binding sites suitable for positron emission tomography (PET) or single photon emission computed tomography (SPECT), the functional anatomy of these neurotransmitter systems in OCD has scarcely been investigated. A commonly used ligand is 123-I-labeled 2-β-carbomethoxy-3-β-(4-iodophenyl)-tropane ([
123I]β-CIT), a SPECT ligand enabling both serotonin (5-HT) and dopamine transporter visualization in the brain. [
123I]β-CIT has already been used extensively to investigate several psychiatric and neuropsychiatric disorders
(13). Binding of [
123I]β-CIT in the striatal region has been shown to reflect mainly binding to dopamine transporter. Binding to 5-HT transporter occurs predominantly in the thalamus, midbrain, and pons, but the binding in these regions might also reflect densities of other monoamine transporters to an unknown proportion
(14,
15). Differences in [
123I]β-CIT binding characteristics for dopamine and 5-HT transporters also make temporal separation of the transporter occupancy possible
(16,
17). Because of these characteristics, both dopamine and 5-HT transporter densities can be visualized in the same subject after a single administration of the ligand. The present study sought to examine possible differences in [
123I]β-CIT binding patterns between patients with OCD and healthy comparison subjects pairwise matched by age, sex, and handedness. In order to further reduce the number of potential confounders, only OCD patients who were psychotropic naive and had no comorbid diagnoses or history of any other major psychopathology were included. We hypothesized that as a result of a putative increase in dopaminergic system activity in OCD, the binding patterns of [
123I]β-CIT in OCD would reflect higher dopamine transporter density.
Results
Of the 375 patients with OCD as their primary diagnosis referred to our specialized unit from 1997 to 2001, 104 had never received treatment with an SSRI
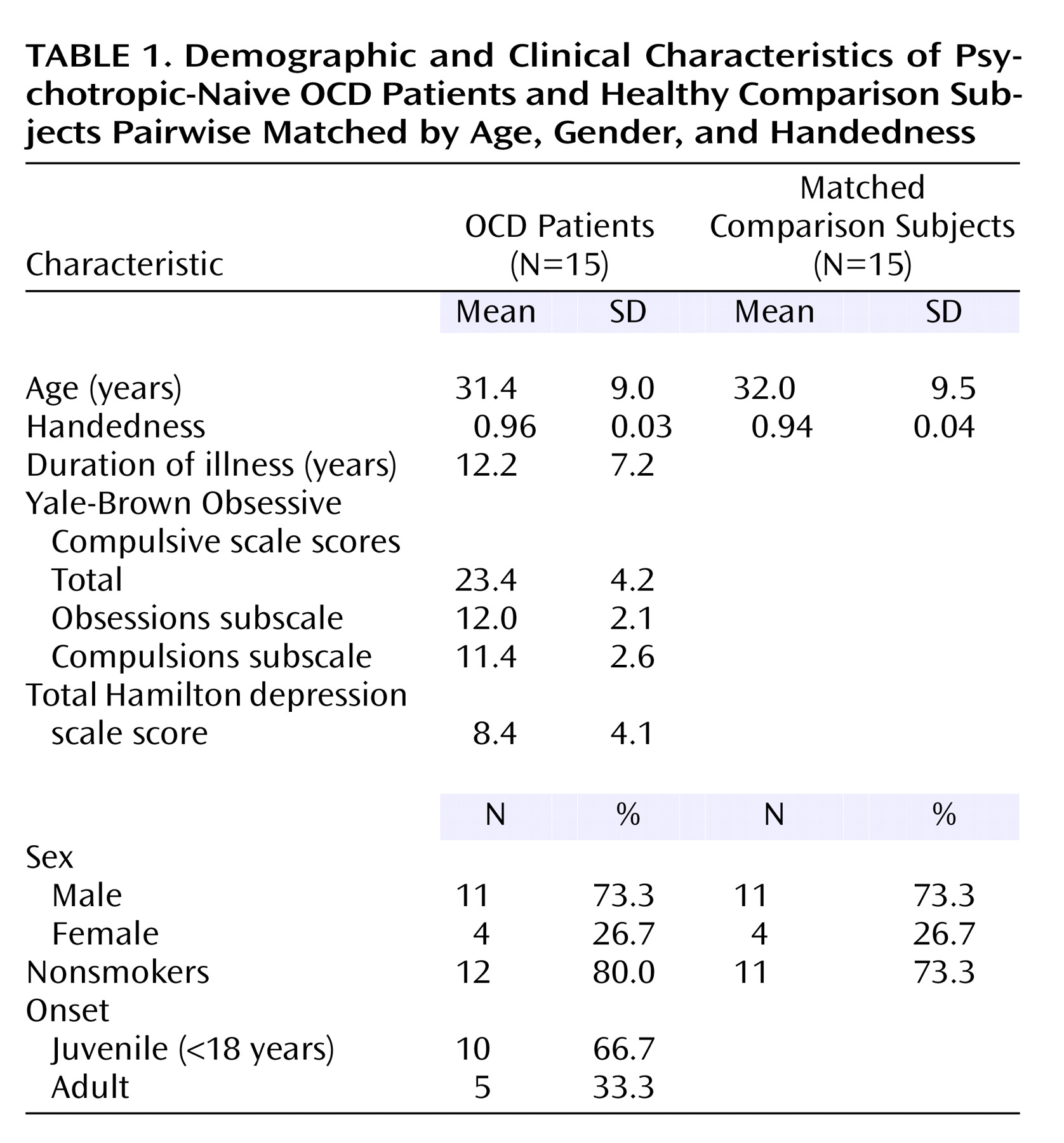
(29). Unfamiliarity with OCD treatment guidelines as well as several patient-related factors may underlie this lack of adequate treatment. Fifty patients were psychotropic naive. Eighteen psychotropic-naive patients fulfilled the inclusion criteria and finally 15 patients participated. Healthy subjects were mainly recruited from the existing database. Six potential comparison subjects refused participation. All subjects completed the study. Patients and comparison subjects were perfectly matched for gender and did not differ significantly in age and handedness. Demographic and clinical characteristics are shown in
Table 1. Almost all subjects were nonsmokers. Symptoms of the patient group were heterogeneous: five patients had predominantly obsessions of contamination and compulsions of washing, six had obsessions of doubt and compulsions of checking, two had predominantly aggressive obsessions and compulsions of counting, and two had mixed symptoms. Most patients had a juvenile onset (before the age of 18) of OCD. Although most patients had some aspects of depressive symptoms, as reflected in the average Hamilton depression scale score, none fulfilled criteria for a depressive episode or dysthymia or any other comorbid disorder at screening. Four patients had a prior single DSM-IV depressive episode not otherwise specified (two with dysthymic and two with more depressive features). One patient had a history of two DSM-IV depressive episodes not otherwise specified, one with dysthymic and one with more depressive features. One patient had received a form of supportive psychotherapy for his depressive symptoms.
Six patients had never received any form of treatment for their OCD. Six others had received a form of supportive or psychoanalytic therapy. Three patients had received a form of cognitive behavior therapy for a short period of time and without any noticeable effect. In these patients the cognitive behavior therapy was stopped at least 18 months before scanning.
In one patient the first SPECT scan (at 4 hours after injection) could not be reliably coregistered to the MRI because of motion artifacts, so the final analysis for the binding in the 5-HT transporter-rich regions involved 14 patients and 14 pairwise-matched healthy subjects. The intraclass correlation coefficients for the intrarater and interrater reliability of the volume of interest procedure were between 0.89 and 0.98 (mean=0.94, SD=0.04) and between 0.86 and 0.99 (mean=0.95, SD=0.05), respectively.
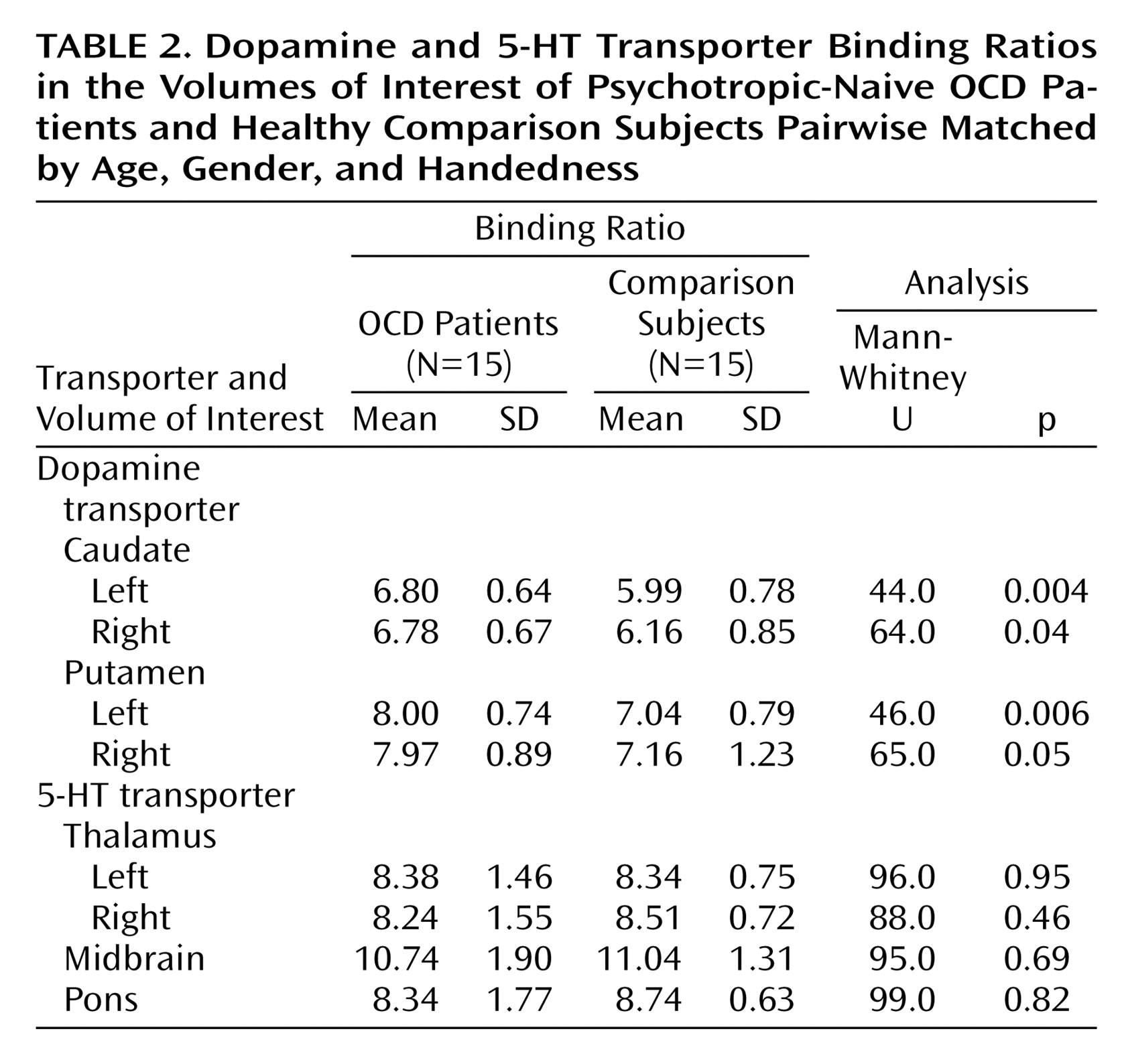
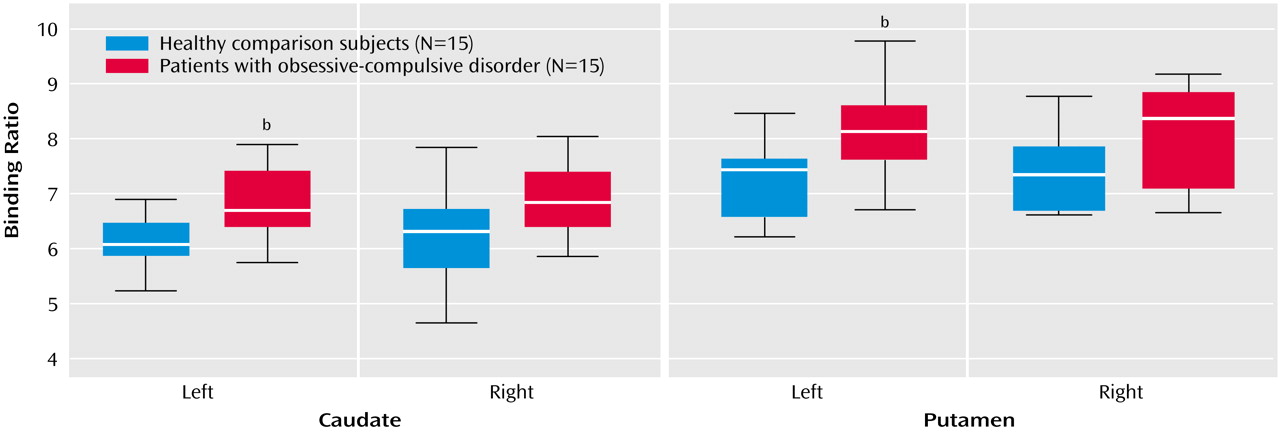
Mann-Whitney U tests revealed a significantly higher average binding ratio to the dopamine transporter in the left caudate and in the left putamen of patients with OCD relative to the matched healthy subjects (
Figure 1,
Table 2). There were no significant differences in average binding ratios to dopamine transporter in the right caudate and right putamen. Patients with juvenile onset and patients with adult onset had similar average binding ratios to dopamine transporter. There were also no significant differences in average binding ratios between the different subtypes of OCD. Hemispheric within-group comparisons for patients and healthy subjects revealed no significant asymmetry effects. No significant correlations were found between binding ratios to dopamine transporter and duration of illness or scores on the Yale-Brown Obsessive Compulsive Scale (total or subscales).
No significant differences in binding patterns were found between patients with OCD and healthy subjects in the 5-HT transporter-rich regions, i.e., the left and right thalamus, midbrain, and pons (
Table 2). Hemispheric within-group comparisons revealed no asymmetry effects. No significant correlations were found for binding ratios in the thalamus, midbrain, and pons with duration of illness or scores on the Yale-Brown Obsessive Compulsive Scale (total or subscales).
Discussion
We found significantly higher [123I]β-CIT binding ratios, an index of dopamine transporter density, in the left basal ganglia of psychotropic-naive OCD patients with no comorbid diagnoses relative to healthy comparison subjects pairwise matched by age, sex, and handedness. No abnormalities in binding ratios to the 5-HT transporter-rich regions in the midbrain, thalamus, or pons were found.
To the best of our knowledge, this is the first study examining central 5-HT and dopamine transporter densities in a carefully selected group of psychotropic-naive patients with OCD. Of interest is that in a recent [
123I]β-CIT SPECT study of Tourette’s syndrome, a disorder that is purported to have also basal ganglia abnormalities, no abnormalities in 5-HT or dopamine transporter densities were found in the basal ganglia, midbrain, or thalamus
(30). Results obtained from functional neuroimaging studies of OCD that used other methodologies most consistently show abnormalities in the right caudate and right orbitofrontal cortex that normalize after treatment
(31). Although this seems suggestive of some form of lateralized functional abnormality in OCD, this is not postulated in the prevailing neurobiological model of OCD.
We did not find hemispheric asymmetries in dopamine or 5-HT transporter binding ratios in any of the bilateral brain structures of OCD patients or healthy comparison subjects. The results of previous studies examining hemispheric asymmetry of dopamine transporter density in healthy subjects and neuropsychiatric conditions are inconsistent with these findings. Differences in radioactive ligands, neuroimaging techniques, and the number of subjects may account for these discrepancies. In a small PET study examining dopamine transporter density in patients with schizophrenia and healthy comparison subjects that used a radiolabeled form of 2-beta-carbomethoxy-3-beta-(-4-fluorophenyl)tropane ([
18F]-CFT), hemispheric asymmetry was only found in the caudate of healthy comparison subjects
(26). In contrast, a SPECT study with a radiolabeled cocaine analog (99Tc TRODAT) did not reveal hemispheric asymmetry in binding ratios to the dopamine transporter in the caudate and putamen of healthy volunteers
(32). However, in a very large [
123I]β-CIT SPECT study that examined age-related decline in dopamine transporter density in 126 healthy subjects, higher binding ratios in the left caudate and putamen were found
(27). Although standard templates were used instead of volumes of interest defined on coregistered MRIs, these findings suggest that our study group may have been too small to detect hemispheric asymmetries within groups.
The data from our present study in psychotropic-naive patients clearly suggest a dopamine transporter role in the pathophysiology of OCD. Theoretically, the higher dopamine transporter density in the left basal ganglia of psychotropic-naive OCD patients, as measured by the [
123I]β-CIT binding ratios, may be either due to a primary abnormality at the level of the transporter or secondary to other abnormalities. Higher transporter density may result from a higher homeostatic tone of the dopaminergic system, with lower densities of D
1 and D
2 receptors
(33,
34). The possible role of higher dopaminergic activity in the left basal ganglia in the pathophysiology of OCD still needs to be elucidated. Both dopamine (through D
1 and D
2 receptors) and serotonin (e.g., through 5-HT
2 receptors) are known to have a modulatory influence on the activity of excitatory (i.e., glutamate) and inhibitory (i.e., GABA) neurotransmitters in the basal ganglia and their cortico-thalamo-limbic connections. Furthermore, both the serotonergic and dopaminergic systems are known to modulate each other’s activity in parts of the fronto-thalamo-basal ganglia circuitry supposedly involved in OCD
(35–
37). Data on the exact nature of these interactions are still inconclusive. Finally, on the basis of the results of the present study, it is not possible to dissect whether dopaminergic abnormalities are causal or epiphenomenal to OCD.
Our study has several strong points. Patients and healthy subjects were pairwise matched, and the patient group consisted of a population with no comorbidity (including tics) that had never been exposed to psychotropic drugs or, for the most part, psychotherapy. Furthermore, SPECT data were analyzed by using coregistered MRI, allowing for more precise determination of the volumes of interest.
There are also some possible limitations to this study. The patient group was heterogeneous for OCD symptoms, reducing the chance of finding abnormalities related to a particular subtype of OCD
(38). We did not match female subjects for the stage of menstrual cycle, but the stage of menstrual cycle was noted at time of scanning. Four female patients were scanned in the first 2 weeks of their menstrual cycle, the remaining four (two patients and two healthy subjects) in the last 2 weeks. Although we included several important parts of the putative disturbed fronto-thalamo-cortical circuitry in OCD in our volumes of interest, other areas could not be investigated in this study. Considering the dispersion of the data, the power of our study may have been too small to detect a bilateral increase in dopamine binding potential in the basal ganglia. Such a bilateral increase in dopamine binding potential could theoretically result from differences in the frequency of the dopamine transporter SLC6A3 genotype, associated with dopamine transporter availability in previous studies
(39).
We found no abnormalities in binding ratios for the 5-HT transporter-rich regions of psychotropic-naive patients with OCD. However, [
123I]β-CIT binding in these regions probably also reflects availability of other monoamine transporters to an unknown proportion. The time point for visualization may have further limited the possibility of finding abnormalities at the level of the 5-HT transporter, as was illustrated in the study by Willeit et al.
(40) in seasonal affective disorder. In the latter study the 5-HT transporter was visualized at 4 hours and 24 hours after injection of the ligand, when a pseudoequilibrium state is reached. Differences were found only in the SPECT acquisitions 24 hours after the injection. In the present study, a 5-HT transporter inhibitor was administered after the first scan in order to displace [
123I]β-CIT from the 5-HT transporter. Hence, the 5-HT transporter could not be visualized 24 hours after injection.
Finally, it should be mentioned that although SPECT is easier to use, has a higher safety index, and is less expensive than PET, it has also relative disadvantages like the poorer anatomical resolution and the use of semiquantitative techniques.
Notwithstanding the possible limitations, our data clearly indicate a role for dopamine in the pathophysiology of OCD. This finding needs to be replicated and should be further explored in studies examining the effect of pharmacotherapy and psychotherapy on both serotonergic and dopaminergic transporter densities in OCD and in studies further dissecting the possible involvement of neurotransmitter systems in this disorder.