Participants were 30 never-medicated patients with schizophrenia and nonschizophrenia psychosis who underwent functional magnetic resonance imaging (fMRI) during an acute psychotic episode and 28 comparison participants. The patient participants were part of a larger study and were recruited because they reported experiencing some type of psychotic symptom and had not previously contacted psychiatric services. Rule-out criteria included 1) age >40 years or <14 years, 2) WAIS-R full-scale IQ <70, 3) non-English native language, 4) diagnosis of substance dependence or substance use disorder within 6 months of testing, 5) neurological disorders or family history of hereditary neurological disorder, or 6) pregnancy. This larger study group and performance measures outside the scanner on the expectancy AX task (see the next section) are described in detail elsewhere
(17). After a complete description of the study to the subjects, written informed consent was obtained.
All patients were followed longitudinally, and their diagnoses were confirmed 6 months after their index hospitalization in diagnostic case conferences that included a review of information from the patients’ chart and from the Structured Clinical Interview for DSM-III-R
(22) administered by trained research personnel. Forty-five patient participants were considered appropriate for the study and consented to be scanned in the current protocol (51% of consecutive participants in the larger study). There were no significant differences between scanned and unscanned participants in terms of demographic characteristics (gender, age, race, education, or parental education), out-of-scanner behavioral performance on the task of interest (expectancy AX task, described in the next section), or degree of psychotic psychopathology (including reality distortion, disorganization, and negative symptoms). Fifteen patient participants were eliminated from the final fMRI analysis for a number of reasons, including technical or equipment problems (N=9), a pattern of behavior that suggested they did not perform the task appropriately (N=4), movement of more than 3.75 mm (approximate 1 voxel) in any direction while being scanned (N=1), or premature withdrawal from the scanning session (N=1).
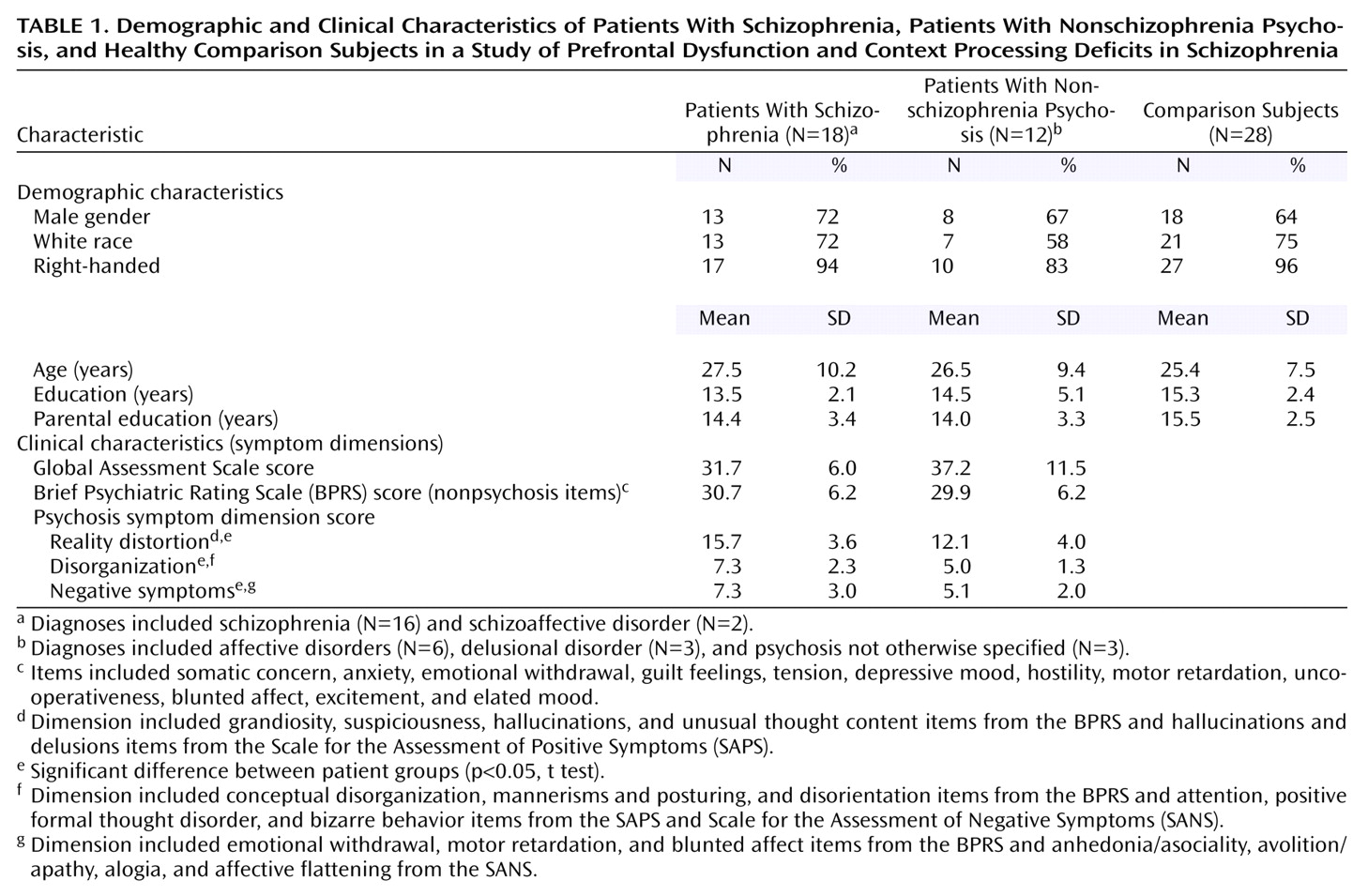
Table 1 summarizes the characteristics of the 18 patient participants who completed the study and had a diagnosis of schizophrenia (N=16) or schizoaffective disorder (N=2) at follow-up, hereafter referred to as the schizophrenia patients. There were also 12 participants who received a diagnosis of another psychotic disorder (six with psychotic affective disorder, three with delusional disorder, and three with psychosis not otherwise specified), hereafter referred to as the nonschizophrenia psychosis patients. A more homogeneous subgroup of nonschizophrenia psychosis patients was not used because 1) selection of a subgroup would have limited the power to detect group differences and 2) all patients shared psychotic symptoms and changes in functioning that led to psychiatric hospitalization. Ratings from the Global Assessment Scale, Brief Psychiatric Rating Scale
(23), Scale for the Assessment of Positive Symptoms
(24), and Scale for the Assessment of Negative Symptoms
(25) were used to measure symptom severity in terms of overall functioning and along three major dimensions of schizophrenia-related psychosis: reality distortion, disorganization, and negative symptoms
(17). As shown in
Table 1, the patient groups showed similar levels of dysfunction and nonpsychotic symptoms. However, the schizophrenia patients showed significantly more reality distortion (t=2.40, df=26, p=0.02) and disorganization (t=2.84, df=26, p=0.009) at index assessment, compared to the nonschizophrenia psychosis patients, and also showed more negative symptoms, although this difference did not reach significance (t=2.02, df=26, p=0.053).
Comparison participants were recruited from the community through advertisements in local newspapers and notices. In addition to the exclusion criteria described for the patients, exclusion criteria for the comparison participants included 1) having a history of axis I disorder
(26), 2) having a first-degree relative with a psychotic disorder, and 3) having been treated with any psychotropic medication within past 6 months. The three groups did not differ significantly in gender, age, race, education, parental education (a proxy measure of socioeconomic status), or handedness (
Table 1).