Research into the effectiveness of specialized, trauma-focused inpatient programs for adults abused as children is very limited, and the studies that have been published have had methodological limitations
(1). Findings from studies of combat veterans with chronic posttraumatic stress disorder (PTSD) may be seen as relevant, since abused adults are frequently diagnosed with chronic PTSD. Studies of specialized inpatient treatment of veterans with chronic PTSD, especially long-stay programs (>90 days), have suggested that this form of treatment is not an effective form of intervention
(2,
3). However, it has been recognized that generalizing from veterans to a population of primarily female abused adults is risky
(4).
The few studies that have investigated outcome for abused adults following specialized inpatient treatment suggest that abused adults may respond better than veterans and that, at least for some, it may be the treatment of choice
(5). An outcome study of women with histories of child abuse, after varying lengths of specialized inpatient trauma treatment, found substantial improvement at discharge; relapse in some symptom areas was reported at a 12-month follow-up evaluation, but the group tended to maintain treatment gains. A substantial minority, however, continued to show severe impairment at the follow-up assessment
(5). Another study reported that patients with dissociative identity disorder were markedly improved 2 years after a stay in a specialized inpatient program
(6). An earlier uncontrolled study in the same treatment setting as the study reported here found that abused adults showed reduced PTSD symptoms at discharge from the 6-week inpatient trauma program. Some decay of gains at a 3-month follow-up assessment were noted, but the study group returned to improved levels at 1 year
(7).
Results
Demographic Characteristics
The participants in the treatment group ranged from 18 to 66 years of age with a mean age of 40 years. Eighty-eight percent lived in Ontario, and 87% were born in Canada. Eight percent identified themselves as belonging to a minority group. Women made up 84% of the group, 58% were married or living with a partner, and 25% were separated, divorced, or widowed. Only 23% had secondary school or less education, with 47% being graduates of a college or university and 29% reporting that they had attended a college or university. Thirty-five percent reported that they had been employed prior to admission, but 44% were on sick leave, and the remainder were homemakers, students, or unemployed. Twenty-eight percent reported an annual family income of $30,000 or less, 27% were in the $31,000–$60,000 range, 21% were in the $61,000–$80,000 range, and 26% reported family income above $81,000 (all amounts expressed in Canadian dollars).
Clinical Characteristics
The category of lifetime traumatic events most often endorsed was “coerced sex before age 18 years” (76%). The mean number of event types experienced in which the participant felt at risk of serious injury or death was 4.6 (SD=0.24). Seventy-six percent of the treated group reported having been physically abused as a child (<16 years), 74% reported child sexual abuse, and 61% reported that they had experienced physical, sexual, and emotional abuse.
Seventy percent of the subjects reported that they had been hospitalized previously for psychological reasons, and 40% reported two or more prior hospitalizations. Thirty-eight percent of the participants assessed with the SCID-II did not meet criteria for any axis II disorder. Twenty-eight percent met criteria for one axis II disorder, and the remainder met criteria for two or more.
At 12 months postdischarge, the median number of visits to helping professionals (psychiatrists, psychologists, social workers, clergy, and social agencies) since discharge was 44, the mean was 45.3, and the number of visits ranged from six to 118.
Analysis of Treatment Group Over Time
Because the wait-list comparison groups were tested at fewer time points than the treatment group, a repeated-measures multivariate test including the three groups at all testing points was not possible. Repeated-measures multivariate analysis of variance (MANOVA) was performed on the scores from the treatment group on the three outcome measures at the five points in time. The analysis yielded a significant main effect for time (Pillai’s trace=0.633, F=5.173, df=12, 36, p<0.001), indicating that the within-subject differences on the three outcome measures across the time periods were significant (SCL-90 global severity index: F=5.701, df=4, 188, p<0.001; Modified PTSD Symptom Scale: F=8.665, df=4, 188, p<0.001; Traumatic Stress Institute Belief Scale: F=4.450, df=4, 188, p<0.001).
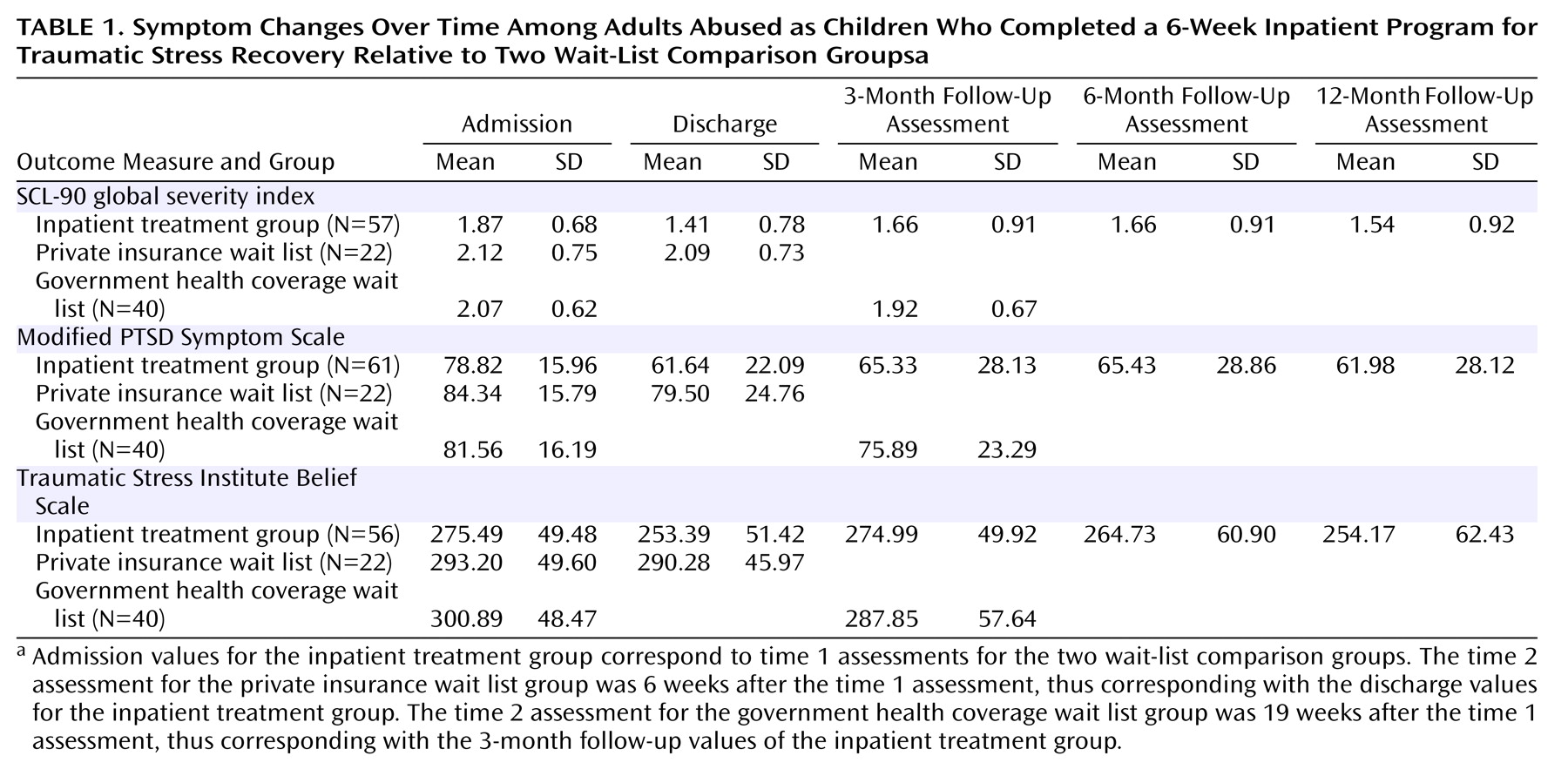
Repeated-measures univariate tests were conducted for each dependent variable separately to determine where the differences in means existed, given the overall multivariate significance. Univariate tests also reduced the amount of missing data compared with the multivariate test. The means and standard deviations from the univariate analyses are illustrated in
Table 1. On the SCL-90 global severity index, relative to admission, the mean was improved at discharge (mean difference=0.46 [p<0.001]) and at all follow-up points (3 months: mean difference=0.21 [p<0.04]; 6 months: mean difference=0.21 [p<0.03]; 12 months: mean difference=0.33 [p=0.001]). Similarly, on the Modified PTSD Symptom Scale, pairwise comparisons revealed that, relative to admission, the mean was improved at discharge (mean difference=17.18 [p<0.001]) and at all follow-up points (3 months: mean difference=13.49 [p<0.001]; 6 months: mean difference=13.39 [p<0.001]; 12 months: mean difference=16.84 [p<0.001]).
On the Traumatic Stress Institute Belief Scale, a different pattern was observed: relative to admission, the mean at discharge was improved (mean difference=22.10 [p=0.001]). However, at 3 months, the mean was not different from admission. At 6 months, it was marginally improved (mean difference=10.76 [p<0.10]), and at 12 months it was significantly better than at admission (mean difference=21.32 [p=0.008]).
Comparison of Treatment and Wait List Groups
The private insurance wait list group and the treatment group were equivalent on all demographic variables except main source of family income: 32% of this wait list group reported their own salary/wages, partner’s income, or investments as the main source of family income compared with 70% of the treatment group. No significant difference was found between the two groups in terms of annual family income. Repeated-measures MANOVA was performed to compare the treatment group (N=103) at admission and discharge with the private insurance wait list group (N=22) at time 1 and time 2 (6 weeks apart) on the three outcome measures. The interaction of group and time was significant (Pillai’s trace=0.074, df=3, 121, p<0.03). Univariate tests indicated that the group-by-time interaction was significant for all three outcome measures. Four covariates (gender, age, marital status, and annual family income) were entered into the same analysis, and the group-by-time interaction remained significant (Pillai’s trace=0.094, df=3, 110, p<0.02).
Univariate tests indicated that the group-by-time interaction was significant for all three outcome measures (SCL-90 global severity index: F=11.401, df=1, 112, p=0.001; Modified PTSD Symptom Scale: F=4.938, df=1, 112, p<0.03; Traumatic Stress Insititute Belief Scale: F=4.663, df=1, 112, p<0.04). These findings indicate that at discharge, the participants in the treatment group were significantly more improved than the private insurance wait list group at time 2.
The government health coverage wait list group and the treatment group were equivalent on all demographic variables except marital status and main source of family income: those in the treatment group were more likely to be married or living with a partner (59% versus 30%), and those in the treatment group were more likely to name salary/wages, partner’s income, or investments as the main source of family income (71% versus 35%). The treatment group was also more likely to have an annual family income over $30,000 than the government health coverage wait list group (71% versus 31%).
A repeated-measures MANOVA was performed to compare the treatment group (N=74) at admission and 3 months postdischarge with the government health coverage wait list group (N=40) at time 1 and time 2 (19 weeks apart) on the three outcome measures. The interaction for group and time was significant (Pillai’s trace=0.08, df=3, 110, p<0.03). Univariate tests indicated that the group-by-time interaction was significant for the Modified PTSD Symptom Scale but not for the other two outcome measures. When gender and age were entered as covariates, the results were similar (Pillai’s trace=0.075, df=3, 107, p<0.04). Marital status and annual family income were not significant covariates. These findings suggest that the treatment group at 3 months postdischarge and the government health coverage wait list group after 19 weeks were not significantly different.
Effects of Demographic and Clinical Variables on Treatment Group Outcome
Age, gender, marital status, source of income, annual family income, axis II comorbidity, and number of visits to helping professionals between discharge and the 12-month follow-up assessment were entered separately into the repeated-measures MANOVA assessing change over time for the treatment group to see if any of these variables interacted with the time factor.
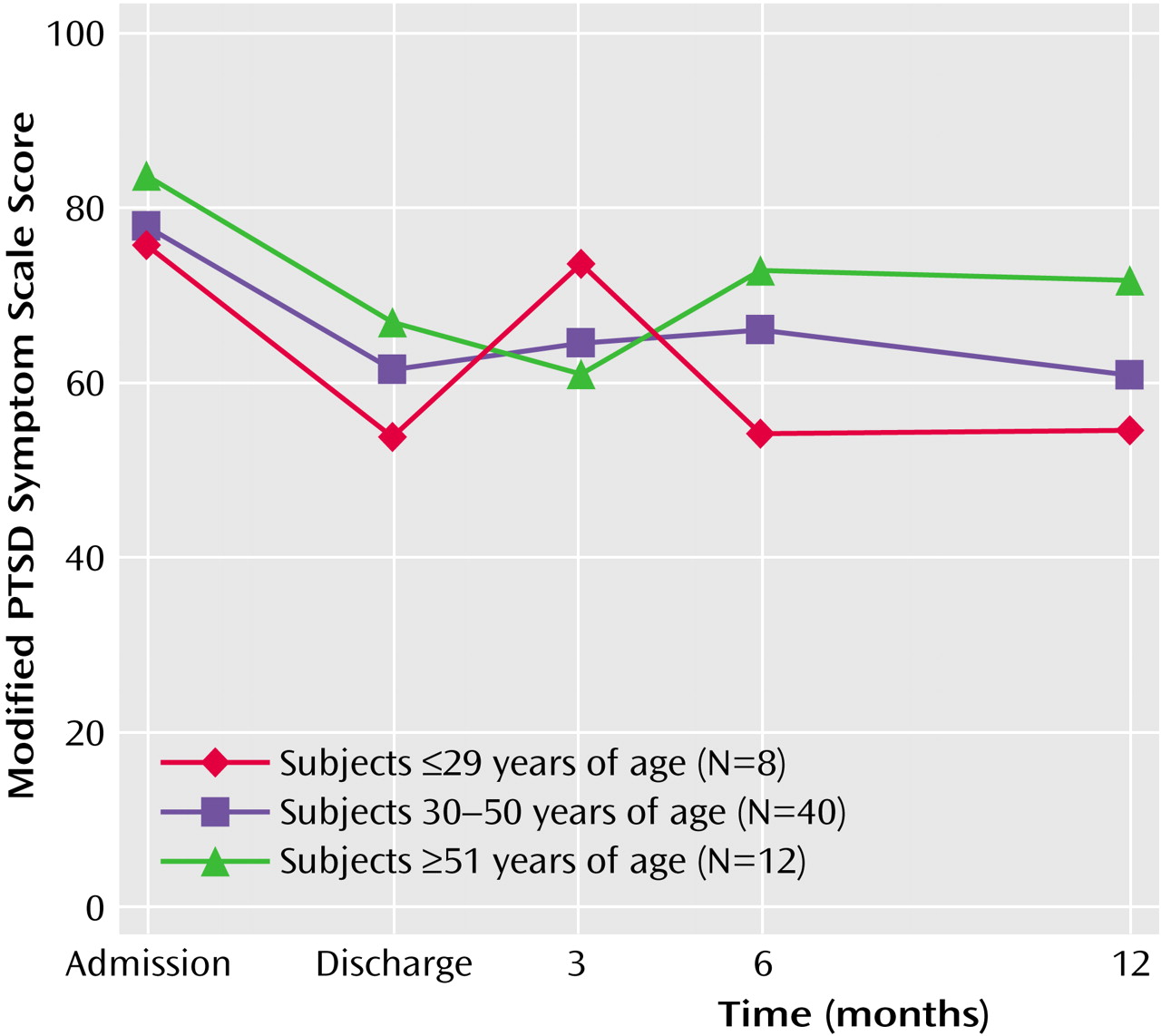
Figure 1 shows that age significantly interacted with score on the Modified PTSD Symptom Scale (F=4.03, df=2, 57, p<0.03). Participants 29 years or younger were more likely to report an abrupt increase in PTSD symptoms at 3 months than were older participants. The mean for participants over 50 years did not increase at 3 months at all, suggesting that older participants may experience the return home differently from younger participants.
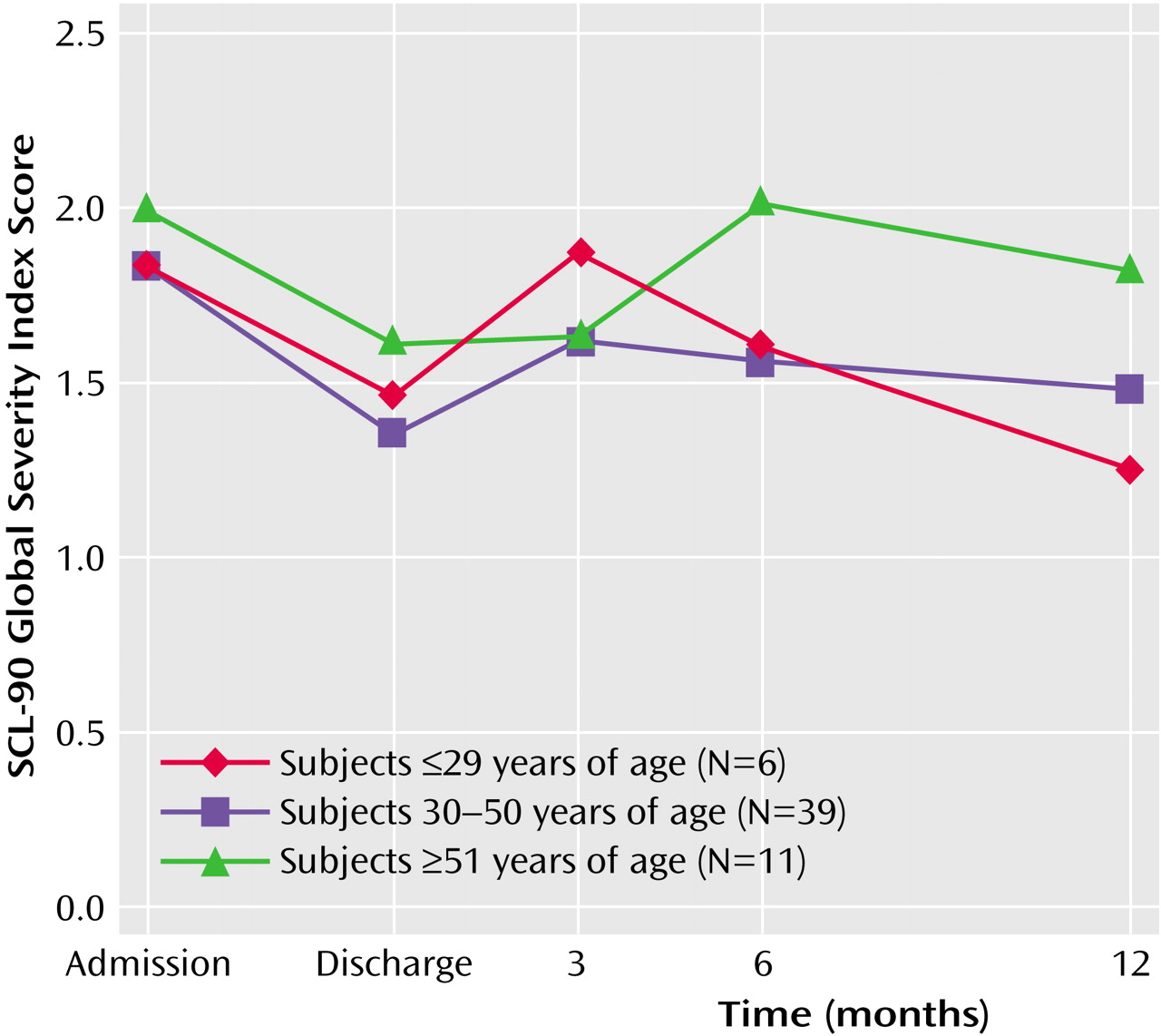
Figure 2 shows that age also interacted with score on the SCL-90 global severity index (F=3.46, df=2, 53, p<0.04). Although the oldest group had the highest mean global severity index score at admission, the mean at 3 months was as low for the older group as for those 30–50 years of age. However, the mean for the older group returned to admission levels at 6 months postdischarge and was only slightly improved at 12 months postdischarge, whereas the younger age cohorts showed more improvement.
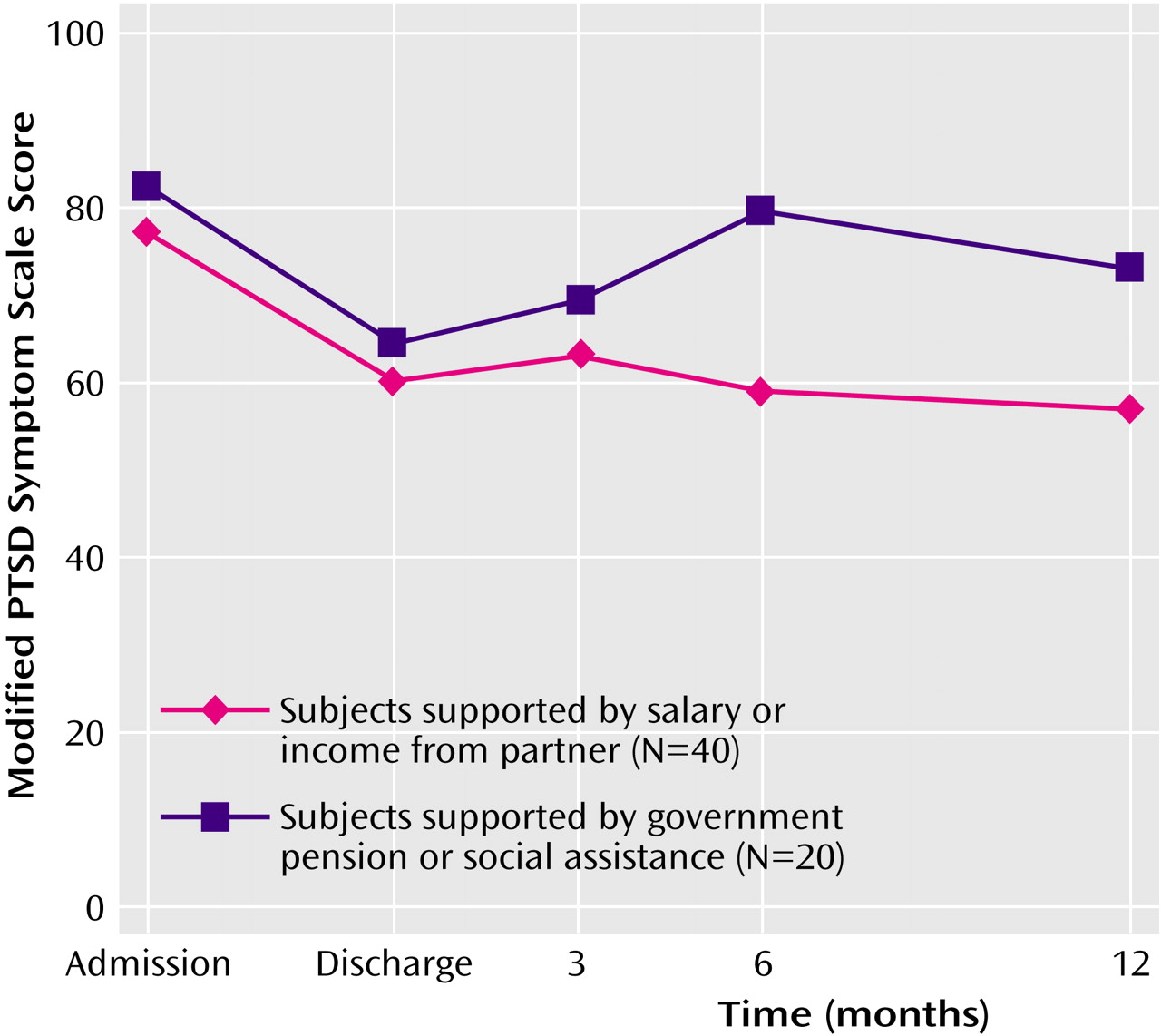
Source of income (personal salary/partner’s income/investments versus government pension/employment insurance/social assistance) significantly interacted with time for score on the Modified PTSD Symptom Scale (F=5.04, df=1, 58, p<0.03).
Figure 3 shows that the pattern of change was similar for the two groups between admission and the 3-month follow-up assessment, but at 6 months, those who were supported by government pension, employment insurance, or social assistance had returned to PTSD symptom levels close to those at admission. By 12 months postdischarge this group had improved slightly but still reported considerably more PTSD symptoms than those who received income from nongovernment sources.
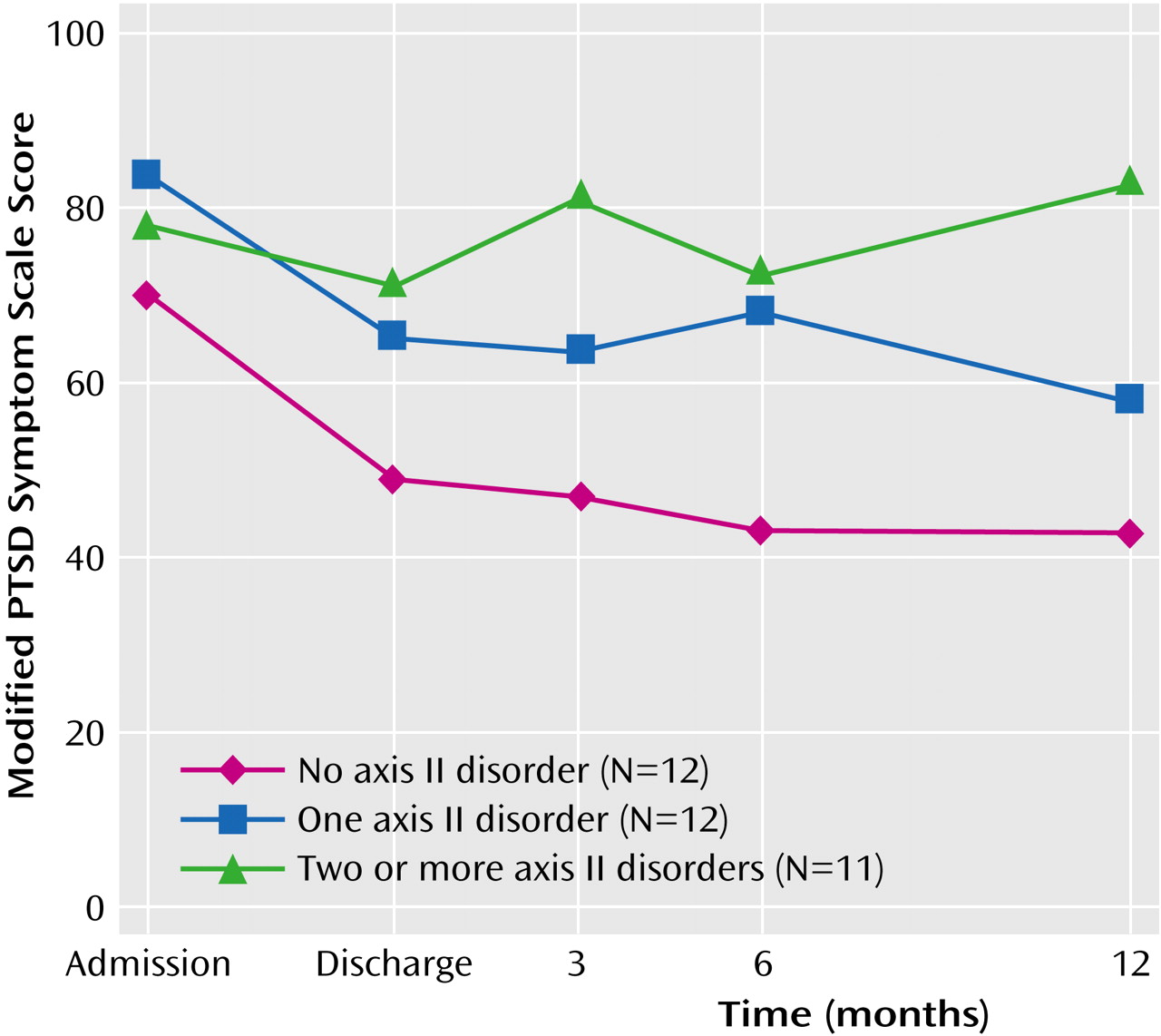
Annual family income significantly interacted with time for score on the Traumatic Stress Institute Belief Scale (F=4.01, df=2, 47, p<0.03), but the interaction did not appear to be clinically significant and is not illustrated here. The number of axis II disorders for which the participant met criteria also significantly interacted with time for score on the Modified PTSD Symptom Scale (F=4.325, df=1, 32, p<0.03).
Figure 4 shows that those who did not meet criteria for an axis II disorder tended to maintain treatment gains at 3 months, whereas those who met criteria for two or more axis II disorders tended to show an increase in PTSD symptoms at 3 months relative to discharge. Chi-square tests of the association between number of axis II disorders and age, source of income, and annual family income were not significant.
Gender, marital status, and number of visits to helping professionals postdischarge did not interact significantly with time on any of the outcome measures.
Participants’ Perceptions of What Was Helpful
From the interviews, the following themes regarding what participants said was helpful about the program were identified: 1) interaction with staff who were respectful of participants and knowledgeable about PTSD; 2) feeling believed and validated; 3) the opportunity to work through emotional issues in a safe environment; 4) the opportunity to learn self-help skills; and 5) recognizing that others had experienced abuse similar to their own. The most commonly reported negative experience was difficulty in returning to everyday life following discharge. A more complete description of the participants’ views of what was helpful and less helpful about the inpatient treatment can be found elsewhere
(19).
Improvement Measures
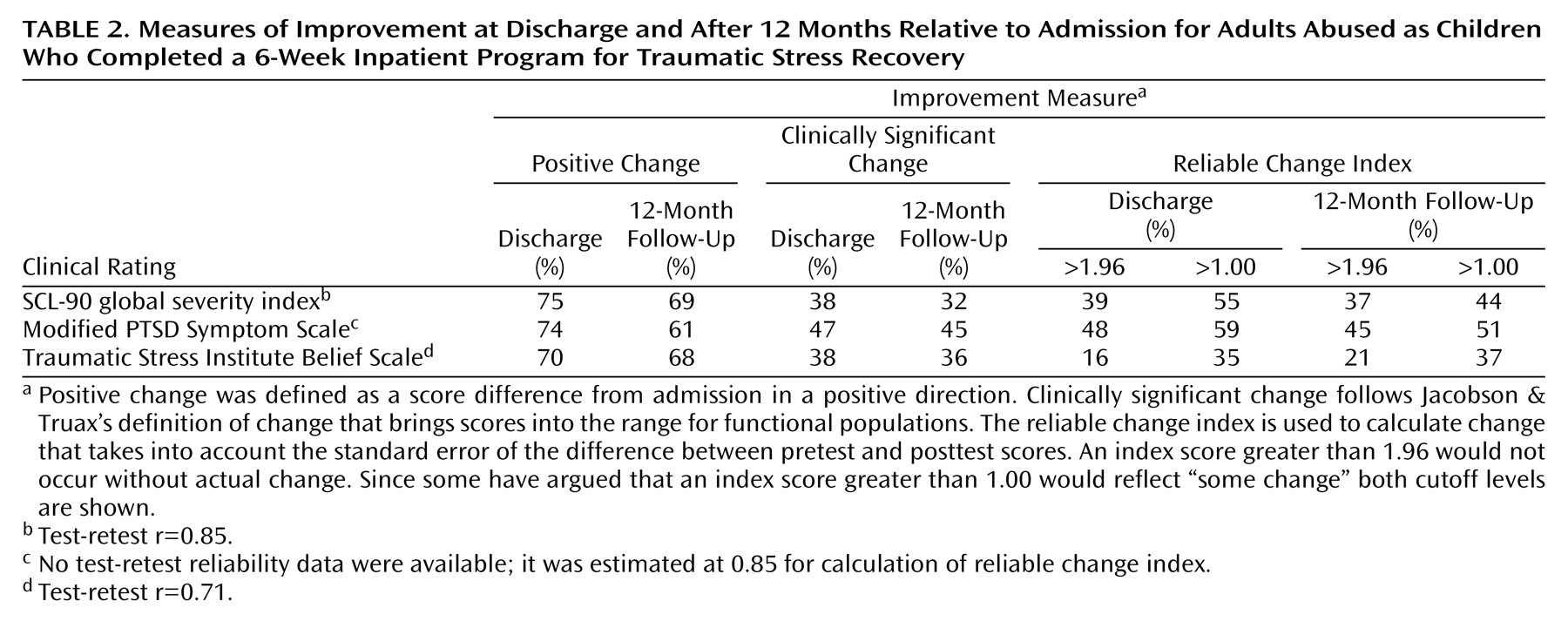
Table 2 illustrates the proportion of subjects in the treatment group that showed positive change relative to admission on outcome scores at discharge and at 12 months postdischarge. Between 70% and 75%, depending on the outcome measure, demonstrated change in a positive direction at discharge, and between 61% and 69% demonstrated positive change at 12 months. Using Jacobson and Truax’s definition, between 38% and 47% demonstrated clinically significant change at discharge, with similar proportions demonstrating clinically significant change at 12 months. Jacobson and Truax
(18) also suggest that for changes in scores to be considered reliable, the reliable change index must be greater than 1.96, because a change larger than 1.96 would be unlikely to occur (p<0.05) without actual change. Others
(20) have suggested that a reliable change index greater than 1.00 can be seen as an indication of “some gain.” The proportions of the treatment group that met these two cutoff points at discharge and at 12 months are also shown in
Table 2.
Discussion
This study has demonstrated that, as a group, adults abused as children who were admitted to a specialized 6-week inpatient treatment program for traumatic stress were improved relative to admission at discharge and 6 and 12 months postdischarge. At 3 months, mean scores deteriorated somewhat compared with discharge scores, but on two of the three outcome measures, the change in a positive direction between admission and 3 months was statistically significant.
When compared with participants on a wait list, the treatment group was significantly better on all outcome measures at discharge. However, when compared at a 3-month follow-up evaluation with a different wait list group, the treatment group was better only on PTSD symptoms, and further analysis suggested that this difference was not robust.
It appears that some participants find the transition from the hospital milieu to the home environment difficult, and that symptoms and disrupted beliefs tend to increase as the participant experiences the stress of this transition. We believe that if a wait list group had been followed for a longer period, significant differences between the treatment and wait list groups would have been evident at the 6- and 12-month follow-up assessments. The following two findings support this hypothesis: 1) the mean outcome scores for the treatment group at 6 and 12 months were significantly better relative to admission; 2) the government health coverage wait list group did not change significantly over that period. However, a study that followed wait list participants for a minimum of 6 months would be required to strengthen this argument.
Interviews with participants indicated that the treatment approach involving the assumption of a connection between child abuse experiences and PTSD symptoms, interventions that encourage participants to separate the past from the present, and the teaching of self-help skills for coping with PTSD symptoms was experienced as helpful, validating, and respectful.
The relatively large size of the treatment group, assessment of PTSD symptoms, inclusion of wait-list comparison groups, and a 1-year follow-up period represent methodological improvements over prior studies of abused adults following inpatient trauma treatment. The results replicate a previous noncontrolled study
(8) by again demonstrating a pattern in which participants lose some treatment gains 3 months postdischarge but regain them at 6 and 12 months postdischarge. They also support the contention of Allen et al.
(5) that the clinical course following inpatient treatment may be more encouraging for adults abused as children than has been observed in studies of veterans. For abused adults who are relatively well educated and economically secure, as were the majority of the participants in this study and that of Allen et al.
(5), the findings suggest a substantial proportion benefit from a specialized inpatient program.
This study also indicates that the course of recovery, especially as assessed by the Modified PTSD Symptom Scale, may vary with differences in age and income, as well as the number of axis II disorders. These findings need to be replicated with a larger sample. We can speculate that the greater deterioration from discharge of PTSD symptom improvement after 3 months for younger compared with older adults may be related to greater sensitivity to the loss of the inpatient treatment milieu or to other factors in the home environment. The finding that dependence on employment insurance or government assistance is negatively associated with the course of recovery evokes questions about whether current social policies are sufficiently supportive of individuals coping with chronic PTSD.
The finding that 39% of the study group exceeded the cutoff for reliable change on the global severity index at discharge can be compared with the 28% of combat veterans reported in an outcome study by Ford et al.
(21) to meet this proportion of reliable change on the same measure following inpatient treatment. Also, in that study, only 22% reported reliable change on a different measure of PTSD symptoms, whereas the current study found that 48% had exceeded the cutoff for reliable change on PTSD symptoms. These findings also support the argument that adults with chronic PTSD associated with child abuse may respond better to specialized inpatient treatment than combat veterans.
The proportion considered improved depends on the criteria used; defining as improved those who demonstrate any amount of change in a positive direction between pre- and posttest is a liberal approach. However, the criteria developed by Jacobson and Truax seem stringent, especially in view of research suggesting that chronic PTSD is associated with structural changes in neuroanatomy
(22). Expectations of this magnitude of change, at least in response to a 6-week program, are unrealistic for many individuals with this diagnosis. Whichever criterion for improvement is used, the findings support previous observations that chronic PTSD, at least for some proportion of abused adults, tends to be resistant to treatment and that the norm may be a partial rather than complete response to intervention, at least in the relatively short spans of time studied thus far
(4,
23).
The field could benefit from studies of adults abused as children that compare outcomes of specialized inpatient programs with those admitted to general psychiatric units and with specialized outpatient treatment. Outpatient treatment has the possible advantage of avoiding separation from family and friends and the difficult transition to the home environment following discharge. However, such separation may be a treatment component that is necessary for many adults dealing with trauma related to child abuse.