In the past decade, various proposals and legislation for mental health care reform have been advanced, but mental illnesses often remain untreated. The mental illnesses of as many as half of patients with a psychiatric disorder are not even recognized by their primary care physicians (
1,
2).
Several factors are known to limit access to and delivery of mental health services, including race, age, income, gender, and the stigma associated with mental disorders. In addition, it is widely believed that many health care providers are inadequately trained to detect mental illnesses. However, the extent of the understanding of mental health benefits among the general public and its influence on service utilization have received less attention.
The study reported here addressed two main questions. First, how informed is the general public about insurance coverage for mental health care? Second, what types of providers of mental health services are preferred by members of the general public, and how do these preferences vary with age and gender?
Background
Mental disorders are misunderstood, feared, and stigmatized, and consequently they often go untreated. In the United States, an estimated 5.4 million individuals (2.7 percent of the population) have a severe and persistent mental illness, 11.4 million (5.7 percent) have a severe mental illness, and 48.2 million (24.1 percent) have some form of a diagnosable mental disorder (
3). Overall, mental illnesses affect one of four families and fill more hospital beds than heart disease. Unfortunately, only one in five persons with a mental illness seeks help.
Primary care providers often fail to recognize mental illness, especially among older adults (
2,
4). Reasons for this failure include ageism (
5), the tendency not to make referrals to mental health professionals (
6), negative views of mental health services (
7), and the complex comorbidity of mental and physical disorders in later life (
8). In addition to these barriers, recent cost-cutting measures in the Medicare and Medicaid programs have led some providers to reduce or eliminate mental health services (
9).
Access to and utilization of psychiatric services are also influenced by gender. Gender differences in prevalence rates for psychiatric disorders, presentation for treatment, course of illness, and treatment response have been noted (
10,
11). In a recent study exploring the effects of sexism on the provision of mental health services, women received more treatments when they first reported a psychiatric episode (Bowers-Walsh H, Byrne C, unpublished data, 1995). Furthermore, women visited their physician more and were given significantly more prescriptions for psychotropic medications than men.
Age and gender notwithstanding, little information has been gathered about whether service patterns might also vary depending on an individual's understanding of mental health coverage. One might speculate that a mental health benefit structure that was difficult to understand, purposely vague, or separate from the benefit design for general health services would constitute a barrier to consumers' gaining access to mental health services. In turn, impediments to access could contribute to lack of timely and appropriate specialized care. The aims of the study reported here were to assess the understanding of mental health benefits design and preferences for mental health providers among the general population and to determine how age and gender may influence these areas.
Methods
This report is based on the 13th quarterly State of the State telephone survey conducted by Michigan State University's Institute for Public Policy and Social Research between November 1997 and February 1998. The survey, which focused mainly on health policy issues, involved random sampling of 1,358 Michigan adults drawn from the major regions of the state and included an oversampling of 418 respondents age 50 and older. The figures contained in this report are based on the entire sample. The overall sampling error is 3.2 percent. The mean age of respondents was 52±16.5 years, with a range from 19 to 103 years. Respondents were predominantly white (78 percent) and female (64 percent).
Of primary interest in this study is the level of understanding of mental health coverage among the general population. Respondents were asked whether they had mental health benefits and whether their mental health coverage was equal to their coverage for general medical services. Persons over age 65 were asked whether the significant limits for psychiatric services and psychotherapy under Medicare would prevent individuals from seeking care when needed.
In addition, all respondents were surveyed about where they would first seek services if they had a mental health need. The following choices were offered: primary care physician, psychiatrist, psychologist, social worker, member of the clergy, family member or friend, mental health clinic, other source of care, and do not know or nowhere. The accompanying box shows the exact wording of the survey items.
Results
Although the total number of respondents in the survey was 1,358, data for only 1,095 of these individuals were included in the analysis, as they had insurance and had completed the questions about mental health. Approximately two-thirds of these respondents, or 76 percent, claimed to be informed about their health plan's coverage of mental health services. Seventy-one percent stated that mental health benefits were included in their insurance plan, and only 5 percent reported that mental health services were not covered. Nearly one-quarter of the sample, or 24 percent, seemed to be unsure.
Perceptions about mental health coverage varied significantly with age (χ2=16.9, df=2, p<.001). Individuals over age 65 were less likely to report having mental health coverage (60 percent) than were younger persons (72 percent). Individuals over age 65 were also more likely to be unsure if they even had mental health coverage (34 percent, compared with 22 percent for those under age 65). There were no significant differences in perceptions by gender.
The survey question on parity of coverage for mental health and general medical services was omitted in data collection from the 333 respondents who reported that they were unsure of their mental health coverage or who stated that they had no coverage. The remaining 760 respondents were asked if their health plan covered the same percentage of costs for mental health services and for general medical services. Although most mental health benefits are in fact not on par with coverage for general medical services, 43 percent of the sample stated that their coverage was equal. Only 18 percent reported unequal coverage. Nearly two-fifths of the respondents, or 39 percent, did not know how the two benefits compared. Perceptions about parity of coverage differed significantly depending on respondents' age (χ2=13.8, df=2, p<.01). In particular, respondents over age 65 tended to be more confused about the specifics of their benefits (52 percent) than younger adults (36 percent).
Despite serious payment restrictions for mental health services under traditional Medicare, however, the majority of the 427 survey respondents over age 65 (57 percent) stated that they would still seek help for a mental health problem if needed. Twenty percent reported that they were unsure. A notable finding is that nearly one-quarter of older persons in this sample, or 23 percent, reported that cost restrictions would prevent them from seeking help.
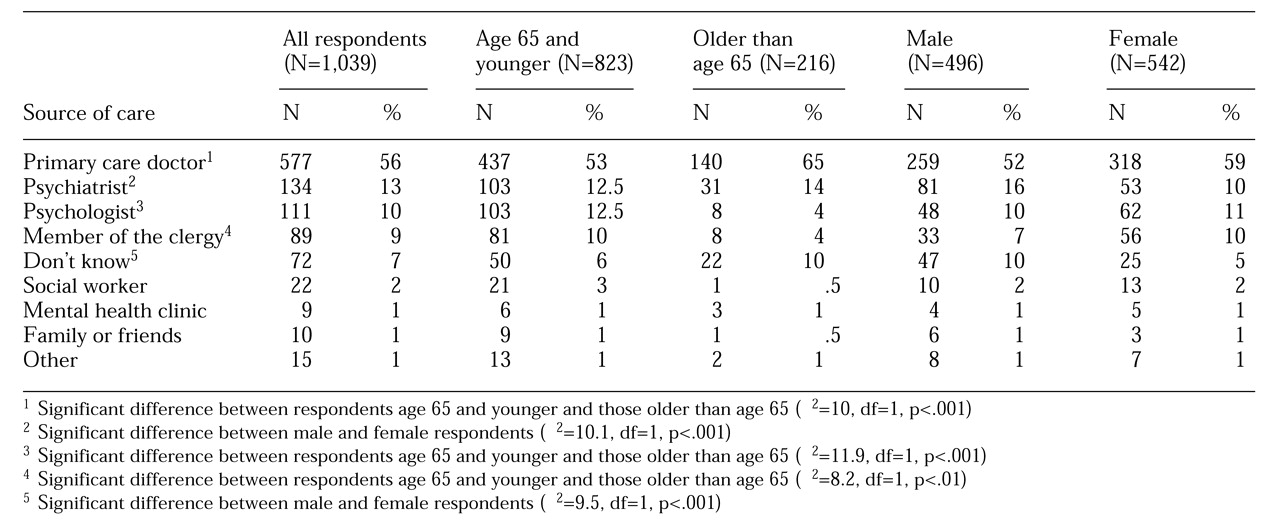
When asked where they would seek mental health services if needed, respondents of all ages gave a wide range of answers from the list provided. As
Table 1 shows, the vast majority of persons indicated that they would choose a primary care doctor for mental health services. Significantly fewer reported that they would select care from a psychiatrist (13 percent), a psychologist (10 percent), and a member of the clergy (9 percent). The next highest percentage of respondents—7 percent—reported that they did not know where they would seek help.
Respondents over age 65 and those age 65 and younger differed significantly in preferences for sources of mental health care (χ
2=36.9, df=11, p<.01). Further analysis indicated that most of the difference was accounted for by choices involving primary care physicians, psychologists, and members of the clergy. As
Table 1 shows, individuals over age 65 were more likely to choose their primary care physician and were less likely to seek help from a psychologist or a member of the clergy, compared with younger persons.
Preferences for care also tended to vary strongly by gender. A greater percentage of men than women preferred a psychiatrist, and men were less likely than women to know where to turn for care.
Discussion and conclusions
Despite the importance of mental well-being throughout the life course, a sizable portion of the general public do not understand their health plan's mental health benefits. Our findings indicate that a large percentage of the public did not know whether their health plan covered mental health at all.
In addition, nearly half of the sample believed that their mental health benefits were comparable to their general medical benefits. Although the Mental Health Parity Act of 1996 required employers and insurers to increase coverage limits for mental health services to the same level as those for general medical services, a recently released Rand study of 4,000 plans demonstrated that 90 percent were not in compliance with the legislation (
12). Thus, although some respondents may have had comparable coverage for mental health and general medical services, that is unlikely to be the case for such a large proportion of the sample. Without accurate information about the individual plans of the respondents, this issue remains speculative.
Medicare's mental health benefits do not have parity with its general health benefits in terms of inpatient service limits and copayment policies. Therefore, the study findings suggest that substantial misunderstanding exists among the older respondents who thought they had similar mental health and general medical coverage. However, perceptions of parity, irrespective of their accuracy, would likely encourage rather than discourage service utilization.
This study also highlighted the strong preference among the general public for a primary care physician as the initial contact in addressing mental health needs. This finding reinforces the conclusion of Marino and colleagues (
13) that patients with psychiatric illnesses tend to see a primary care physician before they see a mental health specialist. Given the gate-keeping task of primary care providers, however, the infrequency with which psychiatrists or psychologists were chosen as the initial source of care may be partly dictated by the constraints of managed care.
Unfortunately, primary care physicians do not detect mental disorders in a high percentage of their patients (
1,
3), and they may not have the time or inclination to effectively manage patients with psychiatric disorders. However, by integrating mental health concerns into their interactions with patients, health professionals may be better able to understand their patients' physical condition. In short, these findings document the strong need to increase attention to mental health issues in primary care medical education.
A rather disturbing finding was that Medicare cost limitations for mental health services may represent a deterrent for a substantial number of older adults in this study, even when the need to seek mental health care may be warranted. However, if services are sought, older adults have a clear preference for receiving care from their primary care physicians. This preference may be due to older respondents' familiarity with their physicians and with the typical routes they used to gain access to health services combined with their lack of experience in utilizing mental health specialists. An additional reason for this preference may be the stigma of mental illness and of seeing a mental health professional, which may be a stronger influence for the older respondents.
Education and outreach to older adults that are focused on mental health issues and benefits are therefore critical. Given the abundant evidence of undetected and misdiagnosed cases of mental illness in later life, ample opportunity exists for improvement in delivery of mental health services to this population.
The study findings also suggest that older persons are less likely than younger persons to discuss mental health issues with members of the clergy and often do not know where to turn for assistance. These findings appear counterintuitive, given the religious bond many older adults are believed to have with their clergy. Elderly persons may view their clergy in the more traditional role as a source of spiritual guidance. In addition, mental health issues that are more appropriate for pastoral counseling, such as marital relations, do not encompass the more common psychiatric needs of elderly persons. Instead, the more common mental health problems experienced by older persons, such as depression or memory disorders, typically require a clinical assessment and intervention.
Women respondents were less likely than men to report using the services of psychiatrists. We have no clear explanation for this finding, which contradicts national trends showing higher utilization of mental health care among women (
14). Women tended to be less uncertain about where to turn to for mental health needs, a finding that may be related to higher prevalence rates of mental illness compared with men.
This study had several limitations. It assessed only subjective knowledge about mental health benefit design and preferences for service providers and did not explore respondents' actual utilization of services. Because the study was limited to Michigan residents, we do not know how well our results generalize to other states or regions.
To the best of our knowledge, however, national surveys such as the National Survey of Psychiatric Practice or the National Health and Nutrition Examination Series have not dealt with these issues. A review of public opinion surveys from 1989 to 1994 focused on voters' support for the expansion of mental health coverage and their willingness to pay for additional benefits but did not include information about the respondents' understanding of their own coverage or choice of providers (
15).
Information is still lacking about the extent to which preferences for care and knowledge of coverage issues are associated with utilization of services. It may be possible that health status is related to both understanding and preferences for care, because individuals with immediate mental health needs or past experience with services are more likely to have the best understanding of how to identify sources of care and navigate the mental health system. From a policy perspective, the widespread misunderstanding of mental health benefits among the general public has likely contributed to overall apathy toward both mental health reform and the implementation of current mental health legislation.