The majority of community studies that have examined the prevalence of pathological eating behaviors have sampled Caucasians in North America and Western Europe (
1–
3). Theoretical models have emphasized Western sociocultural factors as central in the development of eating disorders (
4,
5). Consequently, eating disorders have been conceptualized as illnesses from Western industrialized countries where white women experience social pressures toward thinness (
6). Within these societies, white women are believed to be at risk of developing eating disorders, while black women are not exposed to the same social pressures regarding weight (
7).
One implication may be that non-Western populations are “shielded” from developing eating disorders. In support of this hypothesis, studies generally have found that Caucasian women demonstrate greater concerns about weight and shape than black women (
8–
12). It has been argued that black cultural expectations “protect” black women from developing eating disorders because of more lenient weight and shape standards (
9,
13,
14). In contrast, though, findings from a recent study revealed a considerable degree of body image dissatisfaction in both white and black subjects (
15), indicating that this debate is far from settled.
Research designed to investigate eating attitudes and behaviors in a developing, ethnically diverse society could add significantly to our knowledge of the eating disorders. South Africa is a society that could provide such information because it is a developing country with subsections that espouse Western sociocultural ideals. Epidemiologic data about the prevalence of eating disorders in South Africa's non-Caucasian community are almost entirely absent (
17), and only a handful of published reports are available for the Caucasian community (
18–
23). To date, no systematic investigation has explored the prevalence of eating pathology in adults across all ethnic groups in this society.
This study sought to provide information regarding eating pathology by investigating the presence and severity of unhealthy eating habits and attitudes in female and male students from different ethnic backgrounds in South Africa. Our hypotheses were that 1) Caucasians would demonstrate significantly greater eating attitude and behavior pathology than non-Caucasians, i.e., we predicted a main effect for ethnicity; and 2) females would exhibit greater concern than males regarding food and weight issues, i.e., a main effect for gender.
METHOD
The study was conducted over a 2-year period (July 1992–1994) during which a survey was administered to South African college students. Students at six tertiary institutions from two cities in South Africa (Cape Town and Durban) participated in the study. Although Caucasians are a minority in these communities, they are disproportionately represented in at least four of the six universities surveyed. Nevertheless, these geographical regions provide a representative study group of the ethnic diversity in South Africa. After consent was obtained, undergraduate social science students were invited to volunteer for an anonymous survey of eating attitudes and behaviors. (With South Africa's affirmative admission policy, “typical” undergraduate students from previously non-Caucasian schools tend to be older than those in the United States. Female students are overrepresented in the social sciences.) This invitation was extended during class time, and, instead of a lecture, students were asked to give their time toward this study. A small number of students (approximately 10%) declined to complete the questionnaires that were administered in English.
Subjects completed a demographic questionnaire that was compiled for this study and included items about weight, height, and eating history. The respondents' self-report of their present weight and height was used to calculate body mass index. Subjects also completed the Eating Attitudes Test (
24) and the Bulimic Investigatory Test, Edinburgh (
25). The Eating Attitude Test is a 40-item self-report scale measuring symptoms associated with anorexia nervosa. A score of 30 or higher suggests a possible eating disorder. The Bulimic Investigatory Test, Edinburgh, is a 33-item self-report measure of both the symptoms and severity of bulimia nervosa. A score of 25 or higher suggests a bulimic disorder.
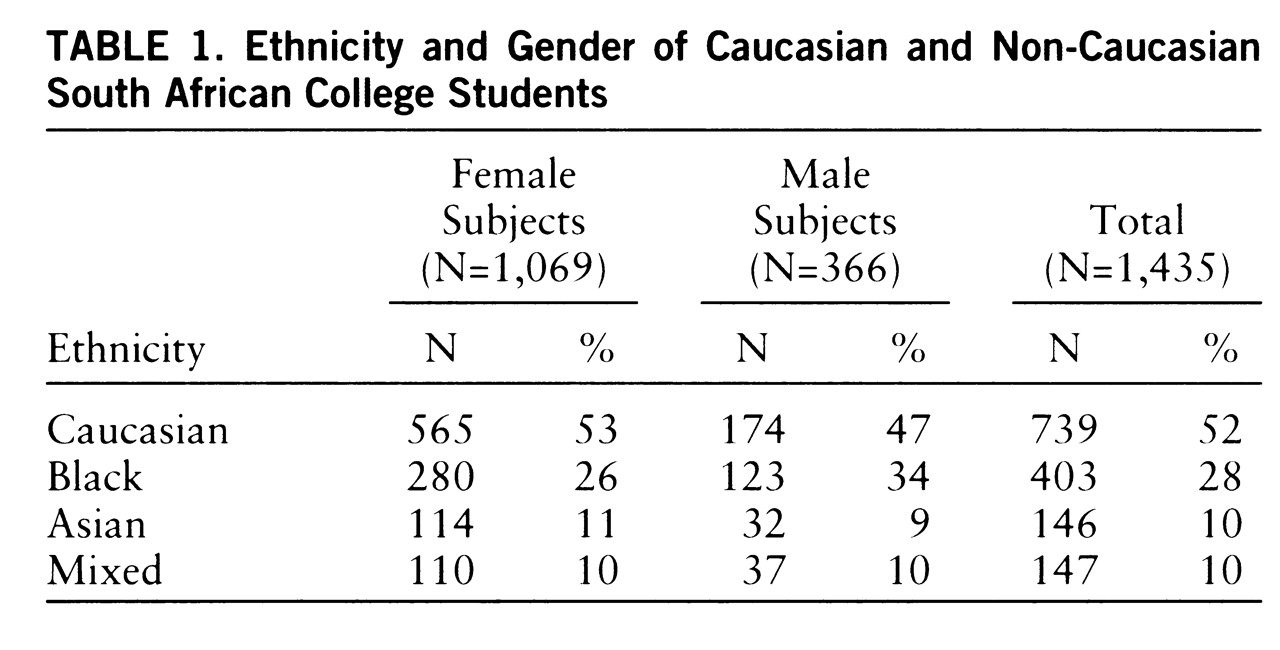
The volunteers included 1,435 social science students 17–25 years years old (mean age=20.0, SD=1.8). We excluded 87 subjects older than 25 years (26–47 years) in order to confirm a study group representative of typical college students. The ethnic breakdown was 739 Caucasian subjects (51%) and 696 non-Caucasian subjects (49%). The mean ages were 20.0 years (SD=1.9) for males and 19.5 years (SD=1.6) for females. Black subjects were heavier (mean body mass index=22.9, SD=4.9) on average than Caucasian (mean=21.2, SD=2.6), mixed race (mean=21.5, SD=3.0), and Asian (mean=20.8, SD=3.7) subjects (F=22.92, df=3,1431, p<0.0001). Therefore, all analyses were conducted with weight as a covariate. The ethnic and gender composition of the study group is reported in
table 1.
RESULTS
Ethnicity and Eating Disorder Psychopathology
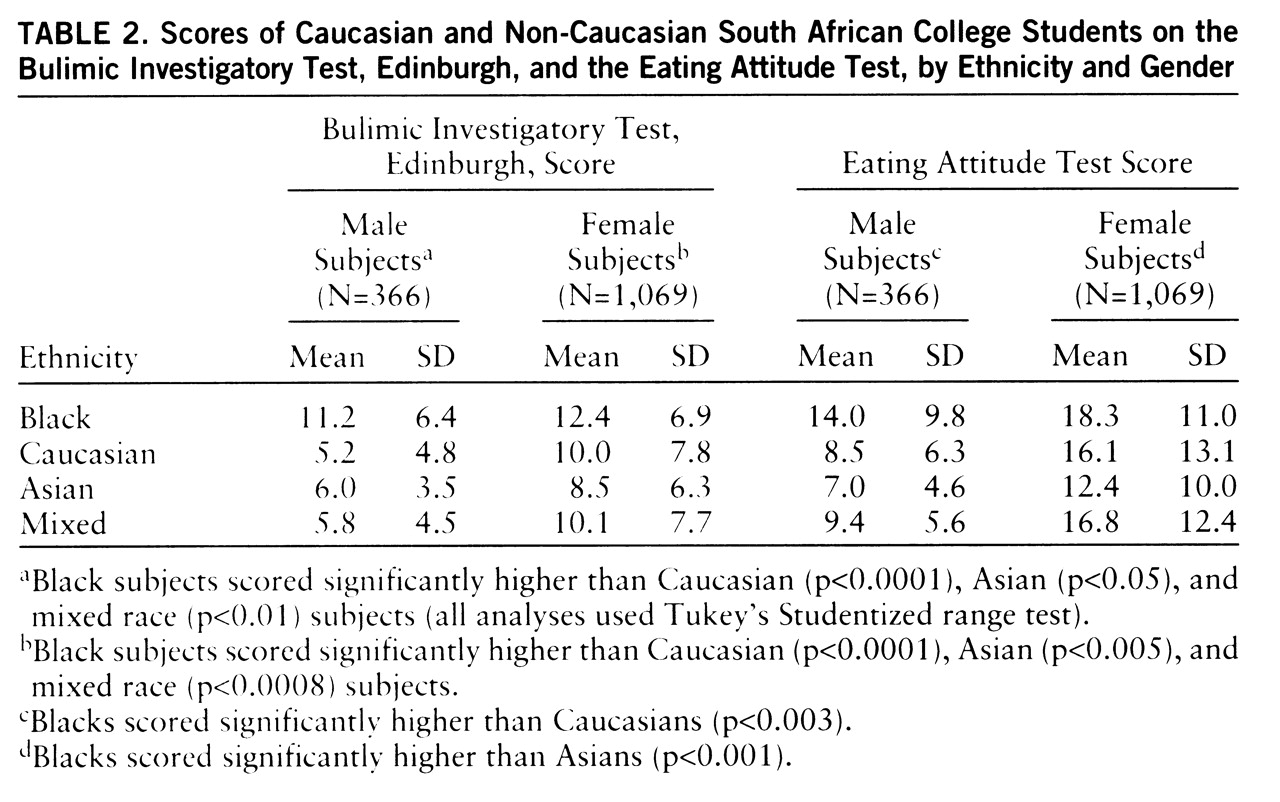
Two-way analyses of variance (ANOVAs) (ethnicity by gender) were performed on subjects' Bulimic Investigatory Test, Edinburgh, and Eating Attitude Test data (mean scores are reported in
table 2). Analyses conducted on Bulimic Investigatory Test, Edinburgh, scores revealed a main effect for ethnicity (F=36.5, df=3,1426, p<0.0001) and for gender (F=75.2, df=1,1426, p<0.0001). Post hoc analyses revealed that blacks scored, on average, higher than the other three ethnic groups. The main effect for gender reflects the fact that females scored substantially higher than males. The interaction between ethnicity and gender was also significant (F=10.23, df=3,1426, p<0.0001); this reflects the fact that the black/nonblack difference in scores on the Bulimic Investigatory Test, Edinburgh, was much greater in males than females, although a simple effects analysis indicated a significant race difference in both genders.
Analysis for the Eating Attitude Test revealed a main effect for ethnicity (F=12.7, df=3,1426, p<0.0001) and for gender (F=51.6, df=1,1426, p<0.0001). Post hoc analyses revealed that black subjects scored higher than the other three ethnic groups and that females scored significantly higher than males, although the interaction failed to reach significance. Thus, contrary to expectations, black subjects scored higher than the other ethnic groups, but, as expected, females generally scored higher than males.
Possible Subclinical Cases
Subjects who reported scores on the Bulimic Investigatory Test, Edinburgh, and Eating Attitude Test above the cutoff points (25 or higher and 30 or higher, respectively) were defined as representing “possible subclinical cases” of eating disorder.
High scores on the Bulimic Investigatory Test, Edinburgh. Of the total study group, 69 subjects (5%) had scores of 25 or higher on this test, indicating a propensity toward binge eating or bulimia. The mean test score for this subgroup was 29.4 (SD=4.7), compared to 8.7 (SD=5.8) for those below the cutoff. The subgroup with high scores comprised 39 Caucasians (5% of Caucasians) and 30 non-Caucasians (4% of non-Caucasians), i.e., 21 black (5%), six mixed race (4%), and three Asian (2%) subjects. These subjects had a mean weight of 64 kg (SD=11), mean body mass index of 22.8 (SD=3.5), and mean age of 19.7 years (SD=1.9). The majority were female (88%) and single (100%). The mean Eating Attitude Test score for this subgroup was also higher than that for subjects scoring below the cutoff for the Bulimic Investigatory Test, Edinburgh (mean=32.8, SD=16.9, versus mean=13.9, SD=10.5).
High Eating Attitude Test scores. A total of 153 subjects (9%) had scores on this test of 30 or higher, which indicates a propensity for anorexic-like behavior. Of these, 84 were Caucasian (11% of Caucasians) and 69 non-Caucasian (10% of non-Caucasians), i.e., 51 black (13%), five Asian (3%), and 13 mixed race (9%) subjects. This subgroup had a mean age of 19.6 years (SD=1.9), mean weight of 59 kg (SD=10), and mean body mass index of 22.5 (SD=5.0). The mean Eating Attitude Test score was 41.0 (SD=9.8), and the mean score on the Bulimic Investigatory Test, Edinburgh, was 19.3 (SD=8.9). This subgroup was predominantly female (92%) and single (99%). Twenty-eight percent (N=43) of those with an Eating Attitude Test score of 30 or higher also had a score of 25 or higher on the Bulimic Investigatory Test, Edinburgh.
These findings suggest that the percentage of subclinical cases of eating disorders does not differ among Caucasian and black subjects.
Subject Characteristics and Gender Differences
The mean weight and height for the study group were 60.0 kg (SD=10.6) and 1.7 m (SD=0.1), respectively. The mean body mass index was within normal limits (mean=22.0, SD=3.6); males had higher body mass indexes than females (mean=22.2, SD=3.3, versus mean=21.5, SD=3.7) (F=12.21, df=1,1433, p<0.0004). Half the subjects (49%) considered themselves at normal weight (mean body mass index=21.0, SD=2.9) (60% of males and 45% of females), and one-third (35%) believed they were overweight (mean body mass index=23.0, SD=3.5) (19% of males and 41% of females). Nine percent believed themselves to be slightly underweight (mean body mass index=20.0, SD=2.5) (18% of males and 6% of females). These percents exclude extremely overweight and underweight subjects. The only ethnic difference worth noting here is that Caucasian female subjects viewed themselves as overweight more frequently than did the other three groups.
The majority of subjects in this study were single (99%) and female (75%). Of the female subjects, 21% reported irregular menstrual cycles. One-way ANOVA showed that compared to female subjects who menstruated regularly, females who did not menstruate regularly tended to have significantly higher scores on the Eating Attitude Test (mean=15.8, SD=11.9, versus mean=19.1, SD=13.4) (F=12.91, df=1,1055, p<0.0003) and Bulimic Investigatory Test, Edinburgh (mean=10.1, SD=7.3, versus mean=12.2, SD=8.1) (F=14.74, df=1,1055, p<0.0001). One inquiry in the demographic questionnaire asked subjects to state whether, in their opinion, they had had a serious eating difficulty in the past. Twelve percent (N=165) of subjects answered affirmatively (mainly binge eating and purging). Most of these subjects were female (N=139; 58% Caucasian, 30% black, 10% mixed race, 3% Asian), and they represented 13% of all females sampled. Of the 26 males who reported that they had serious eating difficulties, 77% were black.
A total of 474 subjects (33% of all subjects) had a body mass index below 20 (mean=18.5, SD=1.2). Most of these subjects were single females (83%, N=391) and were younger (mean age=19.0 years, SD=1.6) than the combined study group. However, the subjects' scores on the Eating Attitude Test (mean=13.5, SD=11.2) and Bulimic Investigatory Test, Edinburgh (mean=8.4, SD=6.5), were all well below the cutoff points. The ethnic breakdown of this underweight subgroup was as follows: 263 Caucasian (36% of Caucasians) and 211 non-Caucasian (30% of all non-Caucasians), i.e., 95 black (24%), 70 Asian (48%), and 46 mixed race (31%).
DISCUSSION
Our findings unexpectedly revealed that black subjects demonstrated significantly greater eating disorder psychopathology as measured by the Eating Attitude Test and Bulimic Investigatory Test, Edinburgh, than Caucasian, mixed race, and Asian subjects. An equal percentage of black and white subjects scored above the cutoff on these measures. In addition, the percentage of female subjects who reported irregular menses and who were underweight was meaningful in all racial groups. Taken together, our findings suggest that significant eating disorder pathology may be prevalent in developing non-Caucasian societies.
In terms of severity of eating pathology, the majority of high scorers on the Eating Attitude Test and Bulimic Investigatory Test, Edinburgh, were black and Caucasian females and were heavier than the rest of the study group. Hence, potential cases of eating disorder were as likely among black as among Caucasian subjects. Nine percent of subjects had Eating Attitude Test scores above the cutoff point, indicating anorexic-like behaviors. Previous investigations using the Eating Attitude Test vary in terms of scores within the clinical range. In Western Caucasian samples, scores ranged from 7% to 12% (
26,
27), while 20% of Hispanic females in Texas scored within the clinical range (
28). Mean Eating Attitude Test scores from previous studies vary from 11 to 19 (
4,
26–
30), similar to findings from our study. What needs to be noted from our results is the ethnic diversity of these high scorers.
Five percent of subjects reported Bulimic Investigatory Test, Edinburgh, scores above the cutoff point, indicating possible bulimic pathology. Compared to the Eating Attitude Test, it was surprising to find relatively few high scorers on the Bulimic Investigatory Test, Edinburgh. However, North American studies have found that between 4% (
31) and 13% (
2) of students experience symptoms of bulimia. In terms of subclinical bulimia nervosa, a recent study in Eastern Europe (
32) found the rate to be between 2% and 4%. This rate is similar to that found in the present study, which may underline earlier claims (
29) that North American findings are not necessarily transferable to other populations. Another study (
27) underscores this point, stating that bulimia nervosa is rarely diagnosed in Poland. Moreover, there are indications that previous estimates of bulimic behaviors in Western samples may be inflated (
33). However, these studies did not use the Bulimic Investigatory Test, Edinburgh, and all subjects were Caucasian, leaving our findings open for interpretation.
Subjects' weight may influence scores on the Eating Attitude Test and Bulimic Investigatory Test, Edinburgh. In our study, black subjects scored highest on these indices and also had the highest body mass indexes (weight was controlled for by means of covariate analyses). One hypothesis, supported by previous studies (
21,
34), is that heavier subjects are more likely to have weight concerns. This point is emphasized by the fact that subjects with body mass indexes below 20 failed to reach the clinical range for either the Eating Attitude Test or Bulimic Investigatory Test, Edinburgh, regardless of ethnicity. In contrast to an earlier proposal that eating disorders are rare in non-Western societies in which plumpness is not stigmatized (
35), our data support the contention made by a recent study (
15) that black and white women experience similar weight concerns.
Our findings with regard to gender were as predicted; females scored higher than males on the eating disorder indices, and almost all cases of possible subclinical eating disorder involved female subjects. One unexpected finding, though, was that black males scored much higher on the Eating Attitude Test and Bulimic Investigatory Test, Edinburgh, than the other three male groups; and their scores were almost as high as those of the female groups. This is difficult to explain, and to our knowledge only one other study has reported similar findings (
9). It is worth noting that 77% of the 26 males in our study who reported serious eating difficulties in the past were black, signaling that eating difficulties may not be that rare among this group. One hypothesis is that black subjects in general and males in particular face new social pressures and expectations by way of “Western syntonic” activities amidst a rapidly changing South Africa.
Some methodological issues concerning our study need to be considered. First, although the study group was representative in terms of ethnicity, most subjects were female university social science students. Our findings could therefore not be extended beyond this population. Second, the Eating Attitude Test and Bulimic Investigatory Test, Edinburgh, were conducted in English, which was not the first language for a large minority of our study group and could be a confounding factor. However, subjects studied English for several years in high school and passed English proficiency requirements for university admission, and instruction and testing at the universities were in English. Therefore, we believe the differences recorded between the ethnic groups may reflect genuine eating pathology as opposed to language difficulties. An alternative hypothesis is that blacks scored higher because of cultural differences. This question should be addressed in future research in which subjects receive the same questionnaires, one in English and a translated version in their first language.
Finally, this study is unique insofar as it is the first to examine eating disorder psychopathology in a large and ethnically diverse South African study group; and it provides much needed insight into the prevalence of unhealthful eating behaviors in this population. Future studies would do well to investigate the nature and course of the full spectrum of eating disorders (
33) across a broader age, race, socioeconomic, and societal range than previously studied.