Compared with other designs, population-based studies with prospective data have yielded limited effects (
2,
5,
6). There is little consensus as to which, if any, specific pregnancy and perinatal factors may be related to schizophrenia, although there is accumulating evidence to support links with exposure to infection (
7), poor nutrition (
8), and hypoxia (
9). The timing of such events is of interest given the debate on putative obstetric causes of cerebral palsy (
3,
10), as is the question of whether events manifest at delivery are themselves the result of earlier problems. Pasamanick et al. (
11) raised the possibility of a spectrum of adverse outcomes of pregnancy and obstetric mishaps. Schizophrenia may be one of these outcomes, but the direction and mechanisms of any causal relationships remain speculative (
12).
METHOD
Study Population and Sample
The 1966 North Finland birth cohort, first described by Rantakallio (
13), is an unselected, general population sample ascertained during midpregnancy. It is based on 12,068 pregnant women living in the provinces of Oulu and Lapland who were due to deliver during 1966. Their 12,231 children, the majority of whom were born in 1966, represent 96.3% of the births subsequently registered at the Finnish Central Statistical Office. The mothers of the remaining 3.7% either refused to participate or did not obtain prenatal care. Of the total 12,231 births, 12,058 were live births. The present study of schizophrenia is based on a risk set of 11,017 cohort members alive in Finland at age 16; before reaching that age, 457 children had died and 757 had emigrated. The members of the risk set have been followed from late gestation through birth to the end of their 27th year.
Case Definition
The ascertainment of cases according to the DSM-III-R criteria for schizophrenia is described in detail elsewhere (
15). It took place in two stages. In the first, each member of the risk set who had appeared in the Finnish Hospital Discharge Register by age 27–28 (i.e., end of 1993) or who had attended a psychiatric outpatient clinic was identified by date of birth and unique social security code. These registers, which themselves classify routine clinical diagnoses according to DSM-III-R, have been shown to have high validity and reliability for a number of diseases, including psychiatric illness, for which the sensitivity for mental disorder and diagnostic specificity were found to be excellent (
15).
In the second stage, the clinical case records of all 224 individuals with clinical DSM-III-R diagnoses of functional psychoses (codes 290–299), personality disorders (code 301), or substance abuse (codes 303–305) were examined by four independent raters. While blind to data on pregnancy and childhood, the raters extracted clinical information according to the Operational Criteria Checklist for Psychotic Illness (
16), and the data were processed by the associated OPCRIT program. This procedure generated DSM-III-R diagnoses. In addition, clinical information was also entered onto the standard form for DSM-III-R diagnoses used by the Finnish Adoption Study (
17). All clinical material was then considered by two senior clinicians (with high diagnostic reliability; kappa=0.77) in order to reach a consensus DSM-III-R diagnosis. Interrater reliability at all stages was high (kappa=0.64–0.96).
A case of schizophrenia was defined as any individual who at any time satisfied the DSM-III-R criteria for diagnosis 295.1, 295.2, 295.3, 295.6, or 295.9. Our hypotheses concerned only schizophrenia; individuals with clinical diagnoses of psychiatric disorders other than schizophrenia were excluded from the study at this stage.
Information on Mothers, the Pregnancy, Delivery, and Postnatal Course
These data have been described in detail by Hartikainen (
18).
Mother and pregnancy to the third trimester. Information on the mother and her pregnancy to date was collected between 24 and 28 weeks of gestation by using routine forms developed especially for the study (
13). This was undertaken by 188 local midwives working in the 157 prenatal clinics serving the area. The data included the following characteristics of the mother: age, educational level, date of last menstrual period, parity, course and outcome of earlier pregnancies (numbers of previous abortions, neonatal deaths, and previous deliveries with birth weights less than 2500 g), smoking habits, prepregnancy height and weight, weight at first prenatal visit, and whether she considered her frame of mind to be as usual or felt depressed or very depressed.
Late pregnancy and delivery. Data on late pregnancy and the deliveries, 98.8% of which occurred in hospitals (
13), were transferred from the delivery records onto standardized forms. This was done by the midwives at the time of delivery. The information on the
mother comprised prepregnancy physical health, bleeding during pregnancy, treated threatened abortion, history of fever higher than 38°C during pregnancy, albuminuria, highest systolic and diastolic blood pressures, edema, and Rh incompatibility. Information on the
child included presence of abnormalities in fetal heart rate (<120 or >160 bpm), fetal presentation, cesarean section, forceps delivery or other intervention, presence of meconium in the amniotic fluid, placental abnormalities, Apgar scores at 1 and 15 minutes, and congenital malformations.
Postnatal period. At the routine postnatal clinic visit, information on postnatal course was transferred from the pregnancy and maternity cards carried by all mothers onto standard forms by the clinic midwives. The variables analyzed in the present study were birth weight, sex of child, and placental weight and diameter.
Perinatal brain damage. An operational definition of perinatal brain damage has been established for this cohort (
19). Perinatal brain damage was defined as the occurrence of one or more of the following:
1. Neonatal convulsions.
2. Low Apgar score (0 at 1 minute or <5 at 15 minutes).
3. Diagnosis of asphyxia (based on arterial blood gas analysis and need for assisted ventilation).
4. Intraventricular hemorrhage (based on CSF analysis).
5. Being detained in, or readmitted to, a neonatal unit in a children's hospital.
6. Brain injury during the newborn period (clinical diagnosis plus abnormal neurological signs at discharge from pediatric unit).
Children with an etiological diagnosis such as CNS malformation, chromosomal aberration, or hereditary CNS degeneration were excluded.
Operational definitions of obstetric complications. In addition to testing hypotheses concerning specific complications, we wished to investigate the association between schizophrenia and two operational definitions of obstetric complications used in the literature. The scale of Lewis et al. was used as published (
20) except that short labor—less than 3 hours—was not considered as a definite complication. We compared the prevalence of definite complications with the prevalence of equivocal and no complications combined.
The definitions of Buka et al. were used as published (
5). First was a general category of any deviation from the norm, analogous to a combination of definite and equivocal complications according to Lewis et al. (
20). Second, subcategories of this deviant group as defined by Buka et al. (
5) were as follows.
1. Chronic fetal hypoxia. Severe preeclampsia (toxemia), maternal hypertension in the third trimester (diastolic blood pressure >94 mm Hg), hypotension in the third trimester (diastolic blood pressure <80 mm Hg), maternal anemia (hemoglobin <105 g/liter), and/or maternal diabetes.
2. Prematurity. Gestational age of less than 36 completed weeks.
3. Other complications. Placental: abruption, infarct, placenta previa; umbilical cord: prolapsed, knotted, or around fetal neck; duration of labor >20 hours; breech delivery; neonatal: asphyxia, respiratory distress syndrome; apnea.
Subjects not meeting any of the preceding criteria were defined by Buka et al. as normal.
Completeness of Data Available for Analysis
Information regarding the mother, the first two trimesters of pregnancy, the postnatal course, and the occurrence of perinatal brain damage was available for all case and comparison subjects. Owing to restricted resources in 1966, particularly computing capacity, the transfer of late-pregnancy and delivery data from the delivery room records to study forms was done in 1967 only for a stratified, random sample of the deliveries (
13). This sample comprised all low-birth-weight infants (<2500 g), preterm and postterm infants (<38th and >42nd gestational weeks), perinatal deaths, and twins. For the remainder (N=8,517 in this risk set) of “normal” births, i.e., single, full-term, normal-birth-weight deliveries, of infants who were alive after the perinatal period, the data were transferred in 1967 for a random 10.7% sample (N=910).
If the null hypotheses are assumed to be true, at the outset of our schizophrenia study delivery information would have been in the study data archive for only 10.7% of the schizophrenia cases from the category of healthy births with normal birth weight and gestational age; the remainder of the information would still be in the birth records. To overcome this discrepancy, the original 1966 birth records were identified in 1994 for 53 (89.8%) of the 59 cases of schizophrenia for which the detailed delivery data had not been transferred to the archive in 1967. Information was then transferred from these original delivery records onto the same standard forms used in 1967, by an obstetrician (P.S.) blind to the hypotheses under study. Thus, the same information and process was used for all subjects.
Comparison Samples and Statistical Analyses
Data regarding the mother, pregnancy to the third trimester, birth weight, postnatal factors, and perinatal brain damage were available for the whole cohort. For these variables the schizophrenia group was compared with the remainder of the risk set, the main comparison group. For the late-pregnancy and delivery variables only, the schizophrenia group was compared with a different, supplementary comparison group. This comprised the original 10.7% random sample of offspring with single, full-term, normal-birth-weight deliveries who were alive after the perinatal period together with a single, random 10.7% sample of the preterm, postterm, and low-birth-weight groups. Subjects with psychiatric diagnoses in the Discharge Register other than those with schizophrenia were then excluded. This process ensured a balanced sample for these analyses, no longer stratified except by case-control status.
Associations are expressed as both crude odds ratios and odds ratios adjusted for confounding by sex, social class, maternal depression, and maternal smoking. These odds ratios are presented with 95% confidence limits. Also presented are F test statistics for removing the term from a model calculated by linear logistic regression and including these confounders. Attributable fractions and population attributable fractions were calculated where appropriate. For continuous variables, group means adjusted for confounding were compared by using analysis of variance (ANOVA).
Thus, basic pregnancy information and postnatal information was analyzed as a routine cohort study with reported odds ratios and based on a risk set. Analysis of the detailed late-pregnancy and delivery information available for the cases of schizophrenia and the supplementary comparison group formed a standard, “nested case-control” design. The sampling fractions were known for both comparison groups, which were each of substantial size.
RESULTS
Occurrence of Schizophrenia
In the first stage of case ascertainment, 515 members of the risk set were identified, of whom 224 (43.5%) had register diagnoses of schizophrenia, schizophrenia spectrum disorders, other psychotic disorders, substance use disorders, or personality disorders. The hospital case notes of all subjects in this latter group were scrutinized and subjected to diagnostic validation.
The diagnostic validation identified 76 cases of schizophrenia (cumulative incidence up to age 28 years=0.69%; 95% confidence interval=0.54%–0.86%). The 439 individuals (4.0% of the original risk set) who appeared on the registers but who were not confirmed as having schizophrenia or whose psychiatric diagnoses remained unvalidated were excluded from this study.
Thus, 10,502 subjects remained in the risk set and formed the main comparison group representing the unaffected population. The supplementary comparison group used for the analysis of detailed delivery data comprised 1,074 subjects not known to be affected by psychiatric disorder.
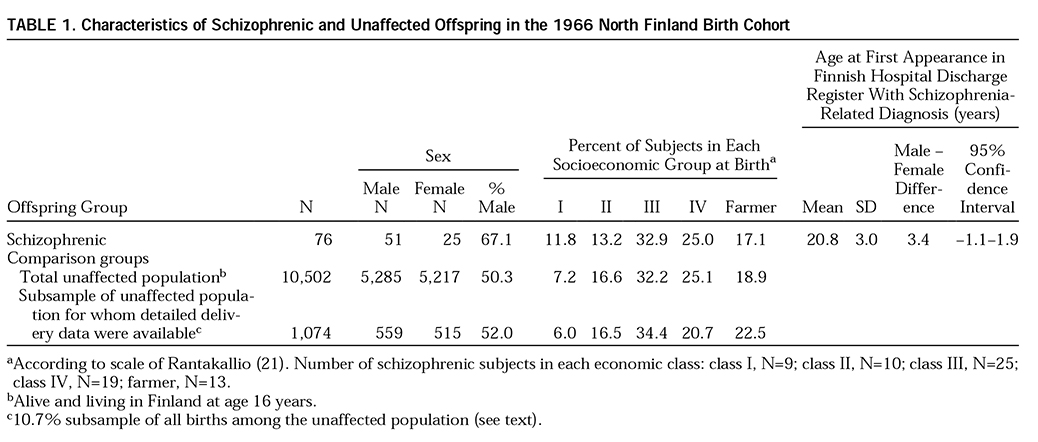
The sociodemographic characteristics of the case and comparison groups are summarized in
table 1. Overall, the distribution of the socioeconomic groups of origin of the schizophrenia group differed little from that of the general population (χ
2=2.9, df=1,4, p=0.57). Men were more likely than women to develop schizophrenia by age 28 (crude odds ratio=2.0, 95% confidence interval=1.3–3.3; F=8.15, df=1,10,573, p=0.004).
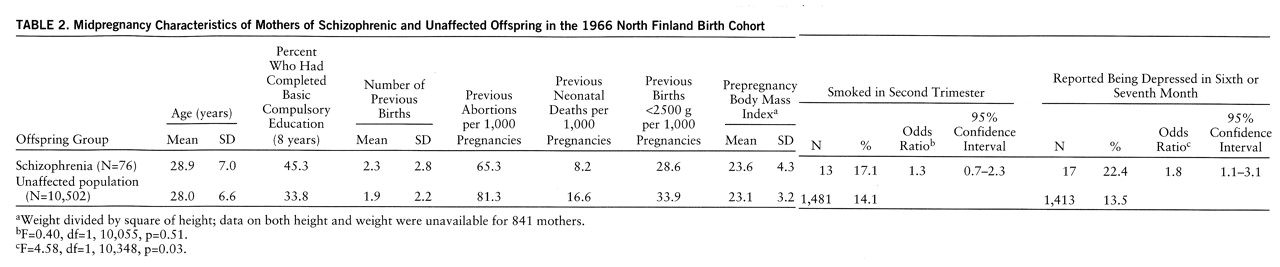
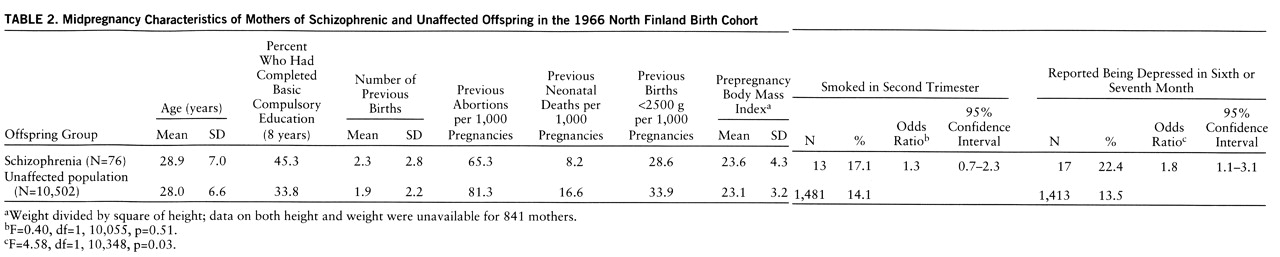
Characteristics of Mothers
Table 2 shows the characteristics of the mothers. These data were available for the whole cohort. There were few differences in previous obstetric history, particularly given the slight differences in the mean ages of the mothers; none of these differences was statistically significant.
The mean prepregnancy body mass indexes of the mothers of the affected and unaffected subjects were similar (
table 2). An ANOVA taking into account the mother's socioeconomic status revealed a significant association between that variable and body mass index (F=8.46, df=4,9,651, p<0.001) but not between subsequent schizophrenia in the offspring and maternal body mass index (F=0.05, df=1,9,651, p=0.82). In a second approach to the analysis of the mother's body mass index, we examined the leanest and the largest fifth percentiles of mothers, defined as those with body mass indexes below 19 (N=497) and those with body mass indexes of 29 or greater (N=524), respectively. These two groups were compared with mothers in the middle 90% of body mass indexes (N=8,640) in terms of risk of schizophrenia among the offspring. In the group of lean mothers, four children (0.8%) developed schizophrenia, similar to the rate for the 57 children (0.7%) from the middle group. Among the offspring of the largest group, seven children (1.3%) developed schizophrenia. Adjusted for sex of offspring, social class, and age of mother, this doubled risk was not statistically significant (odds ratio=2.1, 95% confidence interval=0.9–4.6; F=3.18, df=1,9,521, p=0.07).
Smoking was more common in the mothers of the schizophrenia group, but this small effect was not statistically significant (
table 2). At the sixth to seventh month of pregnancy, the mothers of children who would develop schizophrenia were almost twice as likely as those in the comparison group to classify themselves as depressed (
table 2). This effect persisted in subsequent analyses adjusting for physical problems during the pregnancy.
Late Pregnancy and Delivery
Factors associated with chronic fetal hypoxia. Results for these variables are displayed in
table 3 and concern the supplementary comparison group. There was only inconclusive evidence of a modest effect for factors contributing to chronic fetal hypoxia, with or without the inclusion of maternal smoking, a manipulation we did a priori. Post hoc inclusion of placental complications in the definition of chronic fetal hypoxia increased the effect (odds ratio=1.8, 95% confidence interval=0.9–3.3; F=2.77, df=1,993, p=0.10).
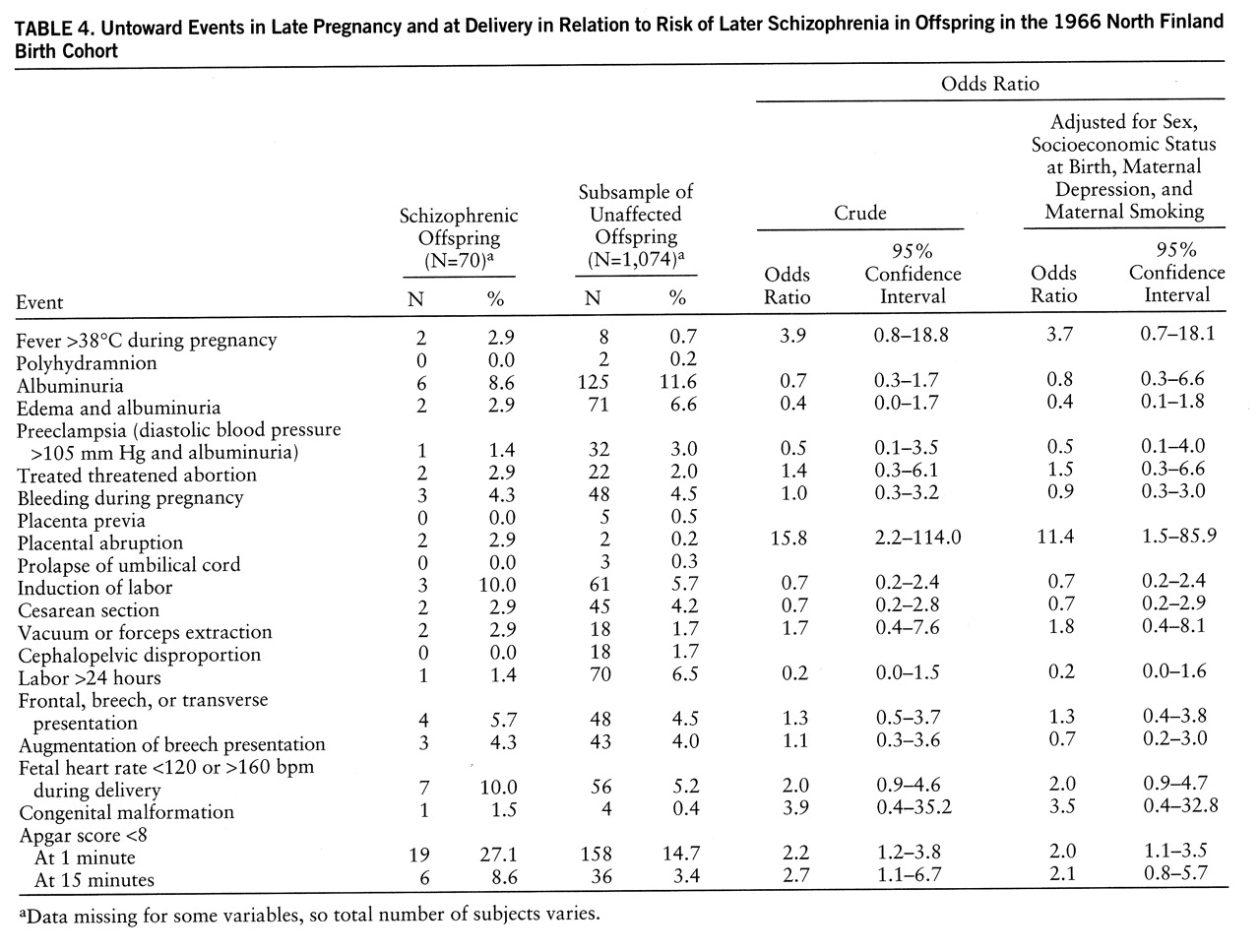
Other deviations from the norm. Table 4 shows other data concerning late pregnancy and the delivery, collected predominantly at or around delivery and involving the supplementary comparison group. There were
few differences between the two groups, with most effects scattered around unity.
We had hypothesized that there would be an excess of maternal fever >38°C in the schizophrenic group, possibly a reflection of infection during pregnancy. The adjusted odds ratio of 3.7 (95% confidence interval=0.7–18.1; F=2.57, df=1,1,092, p=0.11) supported the hypothesis, although the data remained statistically inconclusive at 95% confidence. Abnormal fetal heart rate during delivery and persistent low Apgar scores formed a cluster of variables indicating serious fetal/neonatal illness, considered in the following section concerning perinatal brain damage. Indicators of abnormal delivery, e.g., abnormal presentation or instrumental delivery, were not associated with later schizophrenia.
Birth Weight and Fetal Growth
Mean birth weight. Details of birth weight, placental size and weight, and gestational age were available for the complete cohort. The mean birth weight for the schizophrenia group (3505 g, SD=774) was similar to that of the main comparison group (3488 g, SD=532; difference=17 g) (F=0.07, df=1,10,572, p=0.79). Adjustment for sex of the child and socioeconomic status in an ANO~VA confirmed no significant difference in mean birth weight between the groups (F=1.11, df=1,10,554, p=0.29).
Data on placental size (diameter in square centimeters) and weight were available for 67 subjects with schizophrenia and 9,131 persons in the main comparison group. These mean values were similar in the two groups; no differences between mean values were revealed once sex and social class were adjusted for in ANOVAs (size: F=0.33, df=1,9,111, p=0.57; weight: F=0.30, df=1,6,781, p=0.59).
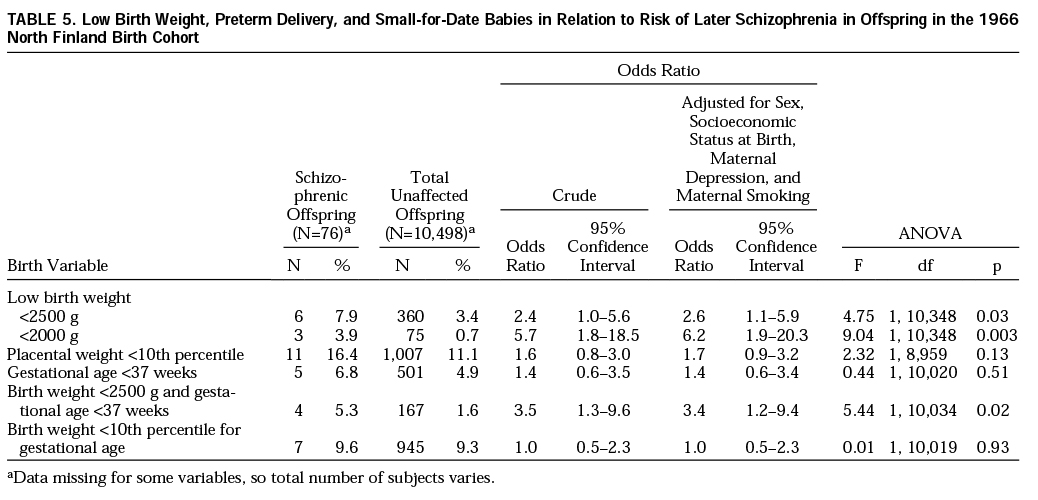
Low birth weight. While the mean birth weights were similar, the schizophrenic subjects were more likely to have been born both small
and early, and there was evidence that small placentas (<10th percentile for placental weight) were more common in this group, as would be expected (
table 5). Thus, it appeared that short gestation but appropriate growth was associated with a subgroup of children who went on to develop schizophrenia. The proportions of schizophrenic offspring and subjects in the main comparison group who were born below the 10th percentile of weight for gestational age (i.e., were small for date) were virtually identical (
table 5).
Perinatal Brain Damage
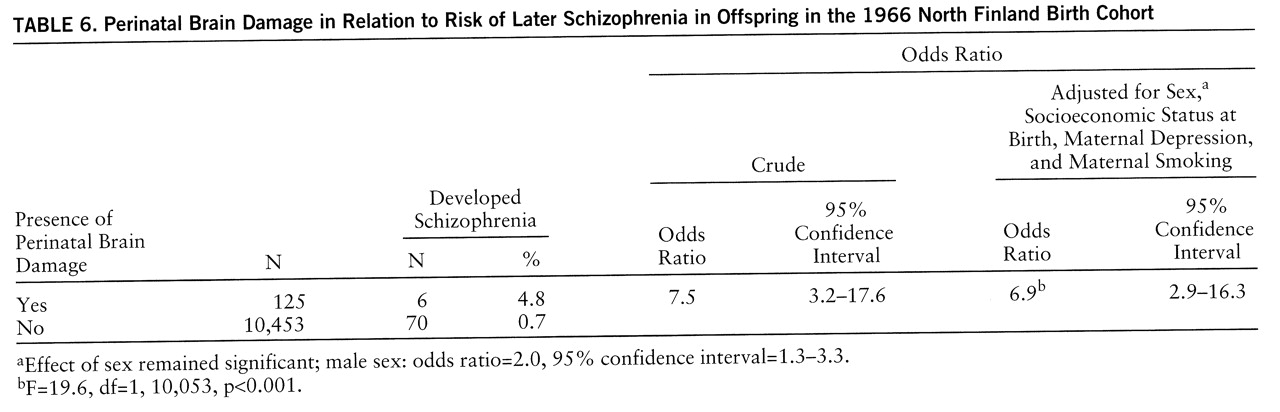
There were 125 subjects in the entire risk set who had met the prior definition of perinatal brain damage and survived to age 16 years without a psychiatric diagnosis in the hospital registers. Subsequent schizophrenia was some seven times as common in this exposed group as in unexposed individuals (
table 6).
Of the six individuals with perinatal brain damage who developed schizophrenia, three had birth weights below 2500 g, and two were below 2000 g. A formal test of interaction was not statistically significant for either birth weight category, and so we cannot exclude the hypothesis that both perinatal brain damage and low birth weight are independently associated with increased risk of schizophrenia. Five of the six subjects were each admitted to a neonatal nursery within the first week of life and spent a prolonged period (>4 weeks) there; the occurrence of this event was statistically more common in those who developed schizophrenia than in those who did not (adjusted odds ratio=3.9, 95% confidence interval=1.4–11.2; F=6.59, df=1,1,092, p=0.01).
If causal, these results indicate that 86% of the cases of schizophrenia in the offspring who survived perinatal brain damage might be attributable to the brain damage (attributable fraction=86.0%, 95% confidence interval=68.5%–93.8%) and that almost 7% of schizophrenia in the general population might be attributable to this factor, as defined here (population attributable fraction=6.8%, 95% confidence interval=5.4%–7.4%).
Operational Criteria for Obstetric Complications
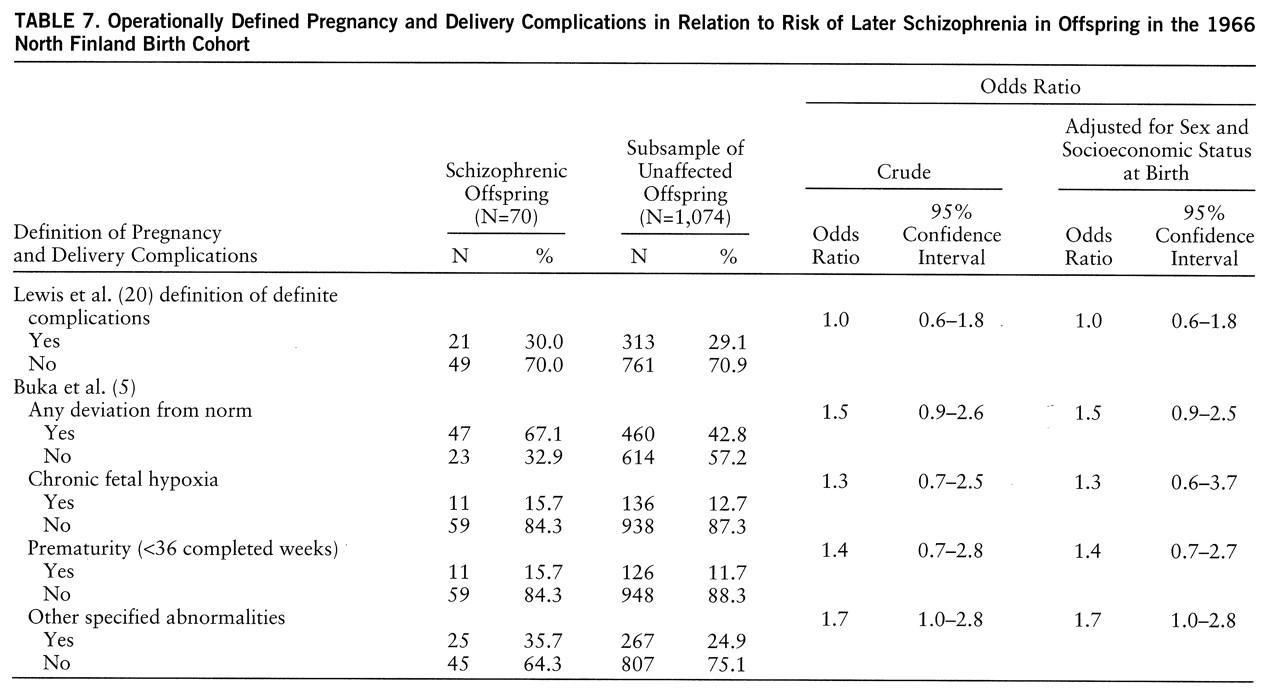
Results for obstetric complications are displayed in
table 7 and are based on the supplementary comparison group and the schizophrenic offspring. There was little difference in the rates of definite complications according to the scale of Lewis et al. (
20). Complications occurred in 29.1% (95% confidence interval=26.5%–32.0%) of the general population.
The category of “any deviation from the norm” defined by Buka et al. (
5) was also common (42.8%, 95% confidence interval=39.9%–45.9%). The three subdivisions were all more common in the schizophrenia group, but no effect was large. The excess of “other specified abnormalities” was attributable largely to a higher rate of placental complications in the schizophrenia group (2.9%, N=2) than in the comparison group (0.2%, N=2) (adjusted odds ratio=11.4, 95% confidence interval=1.5–85.9; F=5.55, df=1,1,092, p=0.02).
Missing Data
The majority of analyses presented involved complete data for the schizophrenia cases and the main comparison group. Delivery data were unavailable for six persons with schizophrenia in the normal-birth-weight, normal-gestation section of the cohort; birth records could not be located. These subjects tended to come from lower socioeconomic groups, four were boys, and their mothers were more likely to be smokers.
DISCUSSION
This investigation confirmed that specific aspects of pregnancy and the perinatal period are associated with later schizophrenia. These effects appeared to be due largely to characteristics of the child, not the delivery. There was no association with conventional obstetric risk factors in the mothers.
The large, unselected general population sample with a high rate of follow-up through record linkage minimized selection bias. The majority of our hypotheses, and our major results, involved data that were collected at the same time and in an identical manner for the case and comparison groups and by investigators who were blind to outcome. The delivery data for a proportion of the cases were available to the study through a slightly different mechanism, thus giving rise to the possibility that information bias may have influenced what were largely negative results (e.g., tables
3 and
4). We feel this is unlikely to have been a major effect. The original information and observations were collected at the same time (delivery) and in a standard manner (on a delivery record used routinely in Finland at the time) for the entire cohort. These items were objective events, not subjective ratings. The difference was only in the time at which some data were transferred from these standard, contemporary delivery records to the data entry sheets for the study. In all cases, the persons transferring the data were blind to the current hypotheses.
We used risk-based analyses, rather than life table methods and survival analyses. This is appropriate for relatively rare conditions such as schizophrenia and for samples such as the North Finland birth cohort, in which emigrations and deaths (N=88) after the age of 16 have been minimal and follow-up is virtually complete. The denominator remains representative of the population at risk of schizophrenia throughout the follow-up period. We excluded the 4.0% of subjects appearing in the hospital registers for psychiatric reasons other than schizophrenia. This decision was taken a priori because this group will be a target of future research in this area. We shall wish to use the same comparison groups so as to allow comparison of effects for schizophrenia and other diagnoses. If it is assumed that these individuals with other diagnoses would, in fact, be at theoretical risk of schizophrenia, their exclusion from the denominator will have caused only minimal bias in our results unless the effect sizes regarding perinatal events and these diagnoses are enormous; there is no evidence to suggest that this is the case (
5).
Boosted by large comparison groups, the study gave reasonable statistical power for our primary analyses. Our focus on confirmatory analyses reduced the risk of both type I and type II statistical errors; large effects are likely worth considering even when the confidence limits include unity. However, mindful of the latter error, we have presented all associations tested so that they might be interpreted in the light of future ideas or can be included in systematic reviews.
The cumulative incidence of DSM-III-R schizophrenia by age 28 years, estimated at between 0.54% and 0.86%, is quite high but in line with results from previous epidemiological studies in Scandinavian and Nordic countries, including Finland (
22); there is no evidence that we missed many cases. All but two of the persons with schizophrenia were hospitalized at one time or another. Hospitalization in the initial stages of schizophrenia remains the rule in Finland, and in addition, schizophrenia appears to be similar in hospitalized and never-hospitalized individuals (
23). We acknowledge that, in a strict sense, our results are relevant only to schizophrenia with a fairly young age at onset.
We have reported elsewhere on the relationship between socioeconomic status and schizophrenia in this cohort (
24). In the current study, adjustment for social class made little difference to any effects, perhaps a reflection of the relative social homogeneity in Finland (
24). There were no gender interactions, and male sex remained an independent risk factor for schizophrenia in all analyses. Subjective depression in the mother and the objectively measured physical variables concerning both mother and child remained independent predictors. Together with the contemporary standardized recording of events, these findings argue against the hypothesis that staff may have been more likely to record abnormalities in the mothers of children who later developed schizophrenia (
25). However, the association with depression in the mother during pregnancy is intriguing, and it may represent the predictably higher prevalence of psychosis in this group of women. Unlike Buka et al. (
5), we were unable to examine family history any further or to look for interactions of genetic risk with pregnancy and perinatal events. This represents a shortcoming in our results and should be an object of future inquiry.
The results from the comparisons of operational definitions of broad categories of pregnancy/obstetric complications demonstrated that they are a fairly blunt instrument and beg the question as to the mechanisms that may be involved. Severe or definite abnormalities were common in the general population, confirming the findings of Sacker et al. (
25) in a cohort in the United Kingdom.
The finding that a proportion of children destined to develop schizophrenia were born early but at appropriate weights extends work demonstrating that low birth weight is associated with schizophrenia, only some of which has included gestational age (
26). The early delivery may have been a reflection of adverse events or may have been due to other attributes of the fetus, which is known to play an active part in the initiation of labor. It is possible that this early delivery successfully removed the infant from a hostile uterine environment where it was failing to thrive owing to generally inadequate nutrition, lack of specific nutritional factors (
8,
27), or damage from other agents, such as immunological attack (
28). Some of these factors might be due to characteristics of the mother, perhaps explaining some of the propensity for women to pass on schizophrenia more readily than men (
29). Alternatively, early birth may be merely a marker of other fetal characteristics more directly related to schizophrenia. Given the findings for perinatal brain damage, this seems unlikely as a sole explanation.
Whatever the explanation, this result adds to considerable evidence of differences in early growth and development in schizophrenia (
26,
30,
31), just as demonstrated in cerebral palsy (
10,
32) and in some chronic adult illnesses (
33). It may also be related to evidence linking childhood neurological disorder (
34) and adult schizophrenia with periods of malnutrition during fetal life (
8,
27). The possibility that schizophrenia may be more common in the increasingly large number of babies who survive very preterm birth remains a concern, while any interaction with genetic risk for these disorders remains undefined.
The prognosis of perinatal brain damage into childhood and adolescence has been studied extensively in this cohort. Rantakallio and von Wendt (
10,
19) identified 231 affected children (58.0% boys; rate, 19.3 per 1,000), of whom 36.4% died within the first 28 days of life and a further 3.0% died by age 14 years. Of the survivors into childhood, 29.9% had mental handicap, cerebral palsy, or both. That 4.8% of the 125 who remained to be included in the risk set used in the current investigation developed DSM-III-R schizophrenia after the age of 16 suggests that this disorder, or subtypes under this umbrella syndrome, might reasonably be considered as part of the long-term sequelae of perinatal brain damage. This suggestion is in accord with recent epidemiological work by Kendell et al. (
9) and with basic research suggesting that the hippocampus may be particularly at risk (
35,
36).
Taken together with the findings for birth weight, and likely the statistically inconclusive although predicted effect implicating maternal fever, the similarities with risks for cerebral palsy are striking (
3,
10,
32,
37,
38). Just as proposed by Pasamanick et al. (
11), the full story of early perturbations of early brain development may take many years to unfold, at least while we have only the current phenotype of schizophrenia to guide us. Our estimate of the population attributable risk of some 7% for tightly defined perinatal brain damage represents a worthwhile public health target, with further benefits extending beyond schizophrenia. However, this statement is based on an assumption of causality that may not be warranted. Even if this assumption is correct, longitudinal population studies can estimate attributable risk only insofar as the perinatal damage (or other exposures) can be identified. If more-sensitive methods demonstrated that the relevant damage were more prevalent, then the calculated population attributable risk would be greater. In the present study, low Apgar scores falling short of the threshold required for our definition of perinatal brain damage were, indeed, more common in schizophrenia (
table 4). This raises the possibility of a more widespread effect and a target for further research.
Our findings suggest that the vulnerable period during which effects occur
may extend over a period during and beyond pregnancy. The study establishes antecedents of schizophrenia detectable in the earliest minutes of postnatal life, but, as we noted earlier, it does not establish them as causes of schizophrenia. They may, themselves, be due to abnormalities already present. Thus, we cannot be certain that the perinatal brain damage was not a manifestation of much earlier events, although the deliveries themselves seemed unremarkable. However, an association between exposure to CNS infections during childhood and later schizophrenia has been demonstrated in this cohort (
39), suggesting that vulnerability
may extend for many years. This question of primacy and the timing of events remains unresolved, but overall the majority of evidence points to an early event. Even the propensity to severe infection after birth may be a result of an abnormal nervous system (
3).
Thus, predisposition to the syndrome of schizophrenia may follow a number of distinct events. Causal heterogeneity (
40) is compatible with the notion of homogeneity of developmental mechanisms; different causes may have similar results. We have shown in this cohort that wantedness of a pregnancy may be an independent risk factor for schizophrenia (
41). This suggests that this heterogeneity may be unexpectedly wide, although we acknowledge that this finding may be due to unmeasured physical factors. Other cohort studies indicate that it may be not that a subgroup of schizophrenia is predated by developmental differences, but that the majority of children destined to develop major mental illness show some decrement of function (
4,
42,
43), although most remain within the normal range, undetected by a group test of abnormality. Parsimony would suggest that the developmental delays and IQ deficiencies shown before schizophrenia (
4) are the result of single, or a small number of, events. Some possibilities during early life have been demonstrated here. Others, including genetic factors (
44), remain obscure. Epidemiology continues to have a role in revealing these causes, but uncovering the mechanisms underlying the development of schizophrenia will require a unified approach across many disciplines.