These data indicate that the adult course for many adolescent girls with antisocial behavior is not benign. Compared to their nonantisocial peers, these women have higher mortality rates, a 10- to 40-fold increase in criminal behavior, a variety of psychiatric problems, dysfunctional and sometimes violent relationships, poor educational achievement, less stable work histories, and higher rates of service utilization.
Continuity Between Adolescent and Adult Pathology
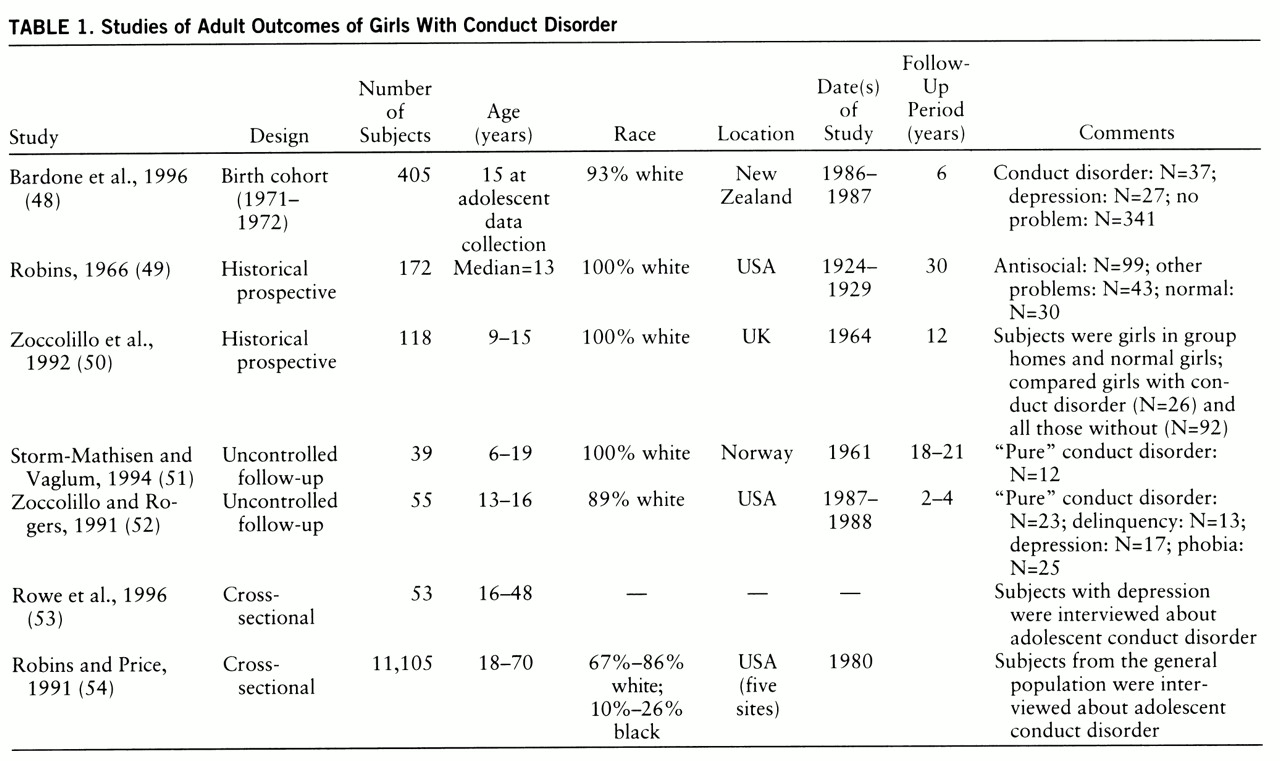
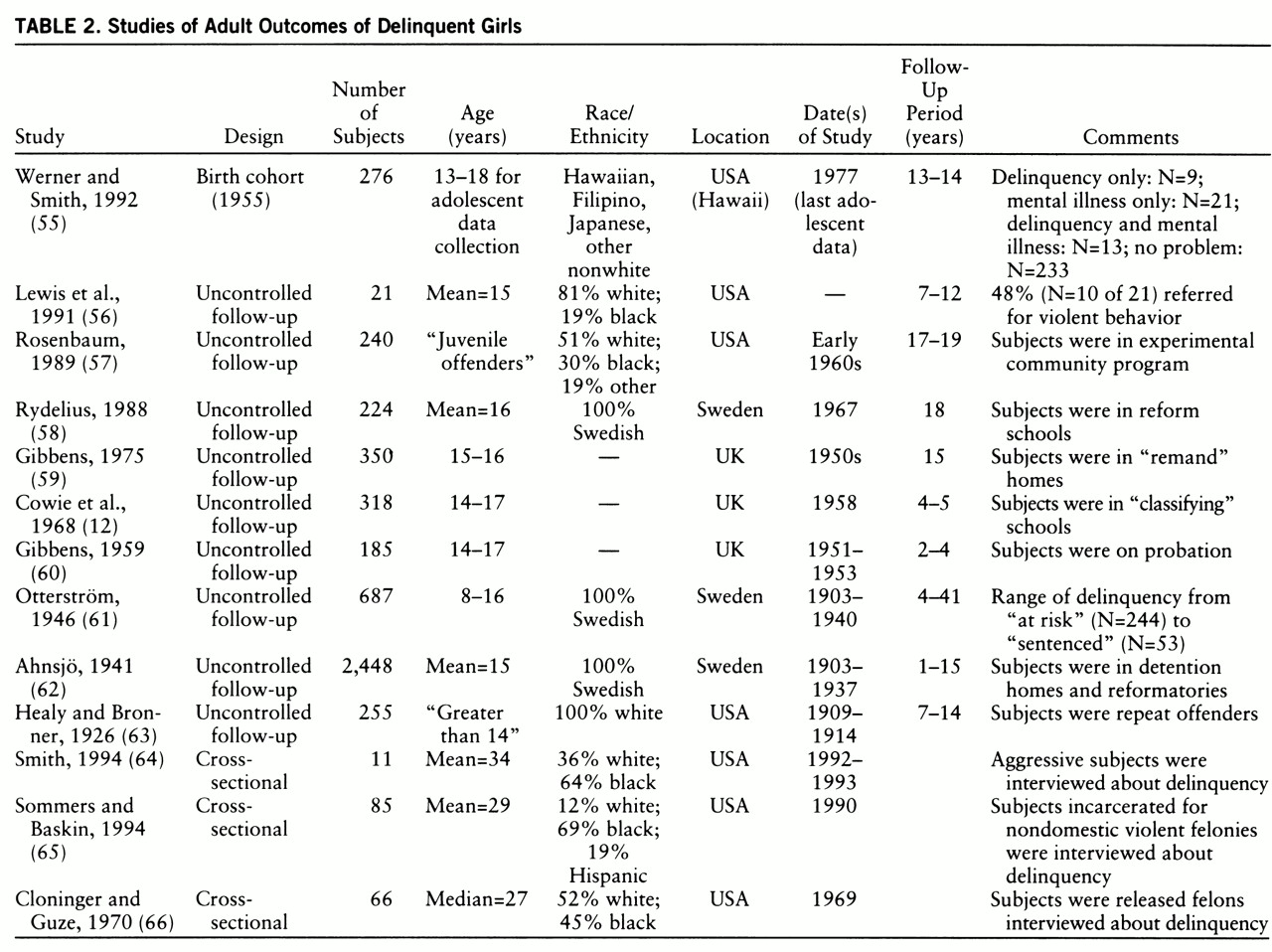
The data clearly support a model of homotypic continuity. At least 25%–50% of antisocial girls engage in adult criminal behavior, and recent delinquency follow-up studies suggest that the rates may be even higher in contemporary cohorts. The cross-sectional studies report that 60%–80% of women with criminal records have histories of antisocial behavior as teenagers. Taken together, these findings imply that antisocial behavior in adolescence is the initial step in the predominant pathway to female adult crime.
Do these girls have an antisocial lifestyle that simply persists into adulthood? Do they start with minor infractions, progressing to more severe criminal behavior? Is there a pattern of misconduct followed by a quiescent period, then emergence of a different type of crime in adulthood? Anecdotal and retrospective data suggest that there are at least two paths between antisocial deviance in girls and such behavior in women (
14,
64,
65,
67,
68). The first is a pattern of persistent, aggressive antisocial behavior beginning during latency and continuing throughout adolescence into adulthood, with a steady increase in the severity and aggressiveness of offenses. The second path is characterized by norm violations starting in the teen years, escalating to more severe adult criminal activity in the context of substance abuse or continued association with deviant peers. These paths are similar to some of those described in boys (
4,
5,
69–
71), although the findings need to be replicated in controlled prospective studies of girls.
Antisocial behavior among adolescent girls was not associated just with adult crime. Regardless of the outcome measure used, the studies reported that substantial percentages of antisocial girls did poorly in adulthood. This multiplicity of adverse outcomes may be a reflection of 1) latent heterogeneity in the population, with subgroups of girls who at baseline may have different prognoses (susceptibility bias) or 2) a large proportion of antisocial girls who display problems in multiple domains of adult life (heterotypic continuity). The data indicate that both conditions may be in operation.
It is quite probable that the population of antisocial girls contains subgroups defined by baseline characteristics that may have prognostic significance, for example, aggression, psychiatric comorbidity, history of abuse, or family dynamics. If a correction for this heterogeneity is not made in the sampling process or in the data analysis, adverse outcomes may show up in every domain. However, this would be a reflection of susceptibility bias, with each of the subgroups developing the outcomes unique to them, rather than a reflection of the majority of the girls having widespread pathology.
In support of this explanation, several studies examined the effects of baseline aggression or psychiatric comorbidity and reported that groups of girls with these characteristics each had sets of outcomes different from those of the girls without them (
12,
48,
52,
55,
56,
62). Future cross-sectional studies of antisocial girls and women should be designed to identify subgroups with potentially different outcomes. Similarly, longitudinal stud~ies should include measurements of the prognostic effects of aggression and baseline psychiatric comorbidity as well as explore the effects of variables such as history of abuse, family psychiatric history, and family functioning.
Although susceptibility bias could explain the variety of untoward outcomes, six studies (
48–
52,
55) reported that one-half of the girls had serious problems in multiple domains of their adult lives, data that clearly support a model of heterotypic continuity. There are two possible mechanisms for heterotypic continuity: 1) there may be a core biological or psychological deficit underlying symptoms in both stages of life, or 2) adolescent antisocial behavior may derail the normal developmental process so significantly in these girls that it seriously compromises their ability to cope with adulthood.
A core biological or psychological deficit would generate a picture of heterotypic continuity by producing maladaptive behavior across all adult domains. Several biological or psychological abnormalities have been associated with antisocial behavior (primarily in males) and could potentially be the mechanism(s) for heterotypic continuity, but I will discuss only the two most likely deficits—prefrontal lobe dysfunction and poor attachment.
Prefrontal lobe dysfunction has been suggested as a potential biological deficit in antisocial behavior (
72,
73). Abnormalities in one or all of the three prefrontal lobe circuits responsible for executive functions, mood regulation, and motivation would result in women characterized by impulsivity, short attention span, difficulty planning or delaying gratification, inability to learn from experience, mood instability, and poor motivation, all of which would impair normal adult functioning. Research into the relationship between prefrontal lobe function and antisocial behavior has predominantly focused on executive functions in deviant males (
73). Two studies that included antisocial girls (
74,
75), however, reported that girls with inattention, distractibility, and impulsivity had higher rates of psychosocial impairment. We have no data on any other aspects of prefrontal lobe function and no research using more sophisticated diagnostic techniques such as imaging. Further research should be done on the role of prefrontal lobe dysfunction in antisocial females.
A core psychological deficit in attachment has long been postulated as an etiologic factor in antisocial behavior (
76) but could also be the mechanism for the heterotypic continuity reported here. Poor attachment has been associated with the inability to form and maintain stable adult relationships with partners, children, peers, and co-workers. This could certainly explain the pervasive dysfunction in women with histories of adolescent antisocial behavior. Most of the studies on the effects of attachment are cross-sectional, use self-report delinquency measures, and have been done on males, but several (
77–
79) have studied female adolescents and reported that attachment difficulties are associated with antisocial behavior. We clearly need to investigate the developmental effect of poor attachment as a factor in adverse adult outcomes.
The second possible mechanism explaining heterotypic continuity is interference with normal adolescent development. This derailment may occur because antisocial behavior prevents girls from learning the social and psychological skills needed for adulthood, or because antisocial conduct may expose girls to situations in which each behavioral choice leads to further deviance. There are no data with which to test this hypothesis, but prospective studies of development in girls with other types of problems, such as early puberty, histories of institutionalization, or depression (
80–
83), indicate that such experiences can derail normal development and lead to multiple poor outcomes in adulthood. We need to collect detailed longitudinal data from antisocial females about the impact of their behaviors on their daily lives. To determine whether antisocial deviance has a uniquely deleterious effect on development, comparison data should also be collected from normal girls and girls with other psychiatric disorders.
Directions for Future Research
In spite of these limitations, this review establishes that female antisocial behavior has important individual and societal consequences. The studies reviewed here suggest that if we do a 10-year follow-up on Jennifer, described at the beginning of this article, we are likely to find that she has not graduated from high school, has had multiple, unstable relationships, is using drugs and alcohol, uses aggression to solve conflicts, has received psychiatric and social services, has been in jail, and has had difficulties caring for her children. Our understanding of the developmental trajectories of antisocial girls and women is so limited, however, that as policy makers or clinicians, we do not know how to prevent or treat such outcomes.
Several lines of research should be developed to resolve these issues. In all types of studies, particular emphasis should be placed on including antisocial females from nonwhite populations, and comparison data should be collected not only from normal females but from psychiatric groups as well. The first type of further research needed is phenomenological studies of antisocial girls and women. This would allow us to assess the validity of our current diagnostic criteria for conduct disorder in girls (
20) as well as identify variables in adolescence that may have long-term prognostic value, such as aggression, psychiatric comorbidity, and type of delinquent behavior. Second, we need cross-sectional studies of the rates of prefrontal lobe dysfunction and poor attachment in antisocial females to determine whether these are important factors in the trajectories to adult pathology. Third, the next generation of longitudinal studies on antisocial adolescent girls should be designed with multiple data collection points, should track subgroups of antisocial girls with potentially different prognoses, and should assess brain and psychological changes over time. Data from these three types of studies will give us the knowledge necessary to develop treatment and secondary prevention strategies for girls like Jennifer.