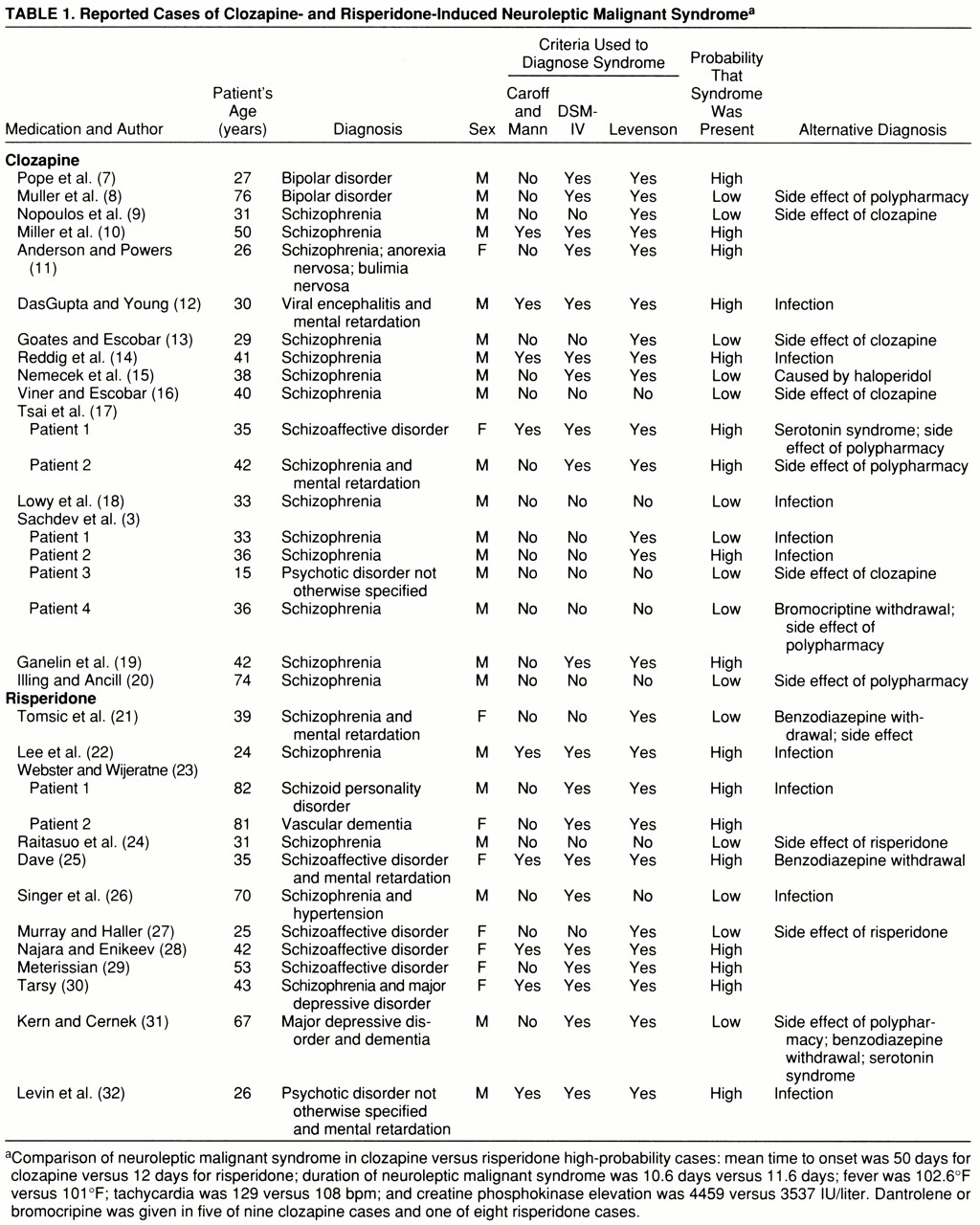
We identified 19 reports of clozapine-induced neuroleptic malignant syndrome and 13 reports of risperidone-induced neuroleptic malignant syndrome (
table 1) with variability in ascribed diagnostic certainty. When we applied the criteria of Caroff and Mann (
5), we identified four of the clozapine cases and five of the risperidone cases as being neuroleptic malignant syndrome; when we applied DSM-IV criteria, 10 of the clozapine cases and 10 of the risperidone cases were so identified; when we applied Levenson's criteria (
6), 14 of the clozapine cases and 11 of the risperidone cases were so identified. All of the cases identified as being neuroleptic malignant syndrome when we applied Caroff and Mann guidelines were also identified by DSM-IV and Levenson's criteria. All but one (a risperidone case reported by Singer et al. [26]) of the cases identified by DSM-IV also met Levenson's criteria. Four clozapine cases (3 [patients 1 and 2], 9, 13) and two risperidone cases (
21,
27) met Levenson's criteria alone. There was consensus for nine clozapine cases (3 [patients 3 and 4], 10, 12, 14, 16, 17 [patient 1], 18, 20) and six risperidone cases (
22,
24,
25,
28,
30,
32); of these, five clozapine cases (3 [patients 3 and 4], 16, 18, 20) and one risperidone case (
24) failed to fulfill any criteria.
Clozapine cases were designated as having low probability of being neuroleptic malignant syndrome if 1) presentations were not causally linked to clozapine because important differential diagnoses were not clearly excluded and concomitant medical illness (3 [patient 1], 18), and concomitant psychotropic medications (
15) were present or 2) they did not fulfill neuroleptic malignant syndrome criteria but were suggestive of possible neurotoxicity of clozapine alone (
9,
13,
16) or with polypharmacy (3 [patient 4], 8, 20). Risperidone cases were designated as having low probability if the presentations were attributable to infection (
26), neurotoxicity from polypharmacy (
31), benzodiazepine withdrawal (
21,
31), serotonin syndrome (
31), and risperidone-induced extrapyramidal side effects (
24,
27).
Nine of 19 clozapine cases were designated as having a high probability of being neuroleptic malignant syndrome, with consensus across criteria sets for four cases (10, 12, 14, 17 [patient 1]). The remaining five cases were close in presentation to typical neuroleptic malignant syndrome, and this was the most parsimonious diagnosis (2 [patient 2], 7, 11, 17 [patient 2], 19). Diagnostic ambiguity remained for three patients (3 [patient 2], 12, 14) with infections of unclear temporal sequence. Eight of 13 risperidone cases were designated as having high probability of being neuroleptic malignant syndrome, with consensus for five cases (
22,
25,
28,
30,
32). Most cases had both fever and rigidity, except two (3 [patient 1], 22) with minimal rigidity and two (
7,
29) with fevers around 99°F.