Despite years of public debate regarding assisted suicide and euthanasia, recently culminating in a Supreme Court decision upholding the ban on assisted suicide, the medical and mental health communities continue to face many unanswered questions regarding why terminally ill patients occasionally desire a hastened death. One central issue regarding the determinants in desire for death concerns the role of depression and physical symptoms in driving a patient’s desire for hastened death. Answering this question, however, has been limited by the lack of valid measures for assessing desire for hastened death. Studies of interest in assisted suicide to date have typically relied on hypothetical questions or vignettes, essentially asking whether or not assisted suicide or euthanasia might be considered an option in the future
(1,
2). This method, however, does not assess current desire for death but, rather, hypothetical anticipated thoughts or attitudes that may have little correspondence to actual end-of-life decision making.
Chochinov and colleagues
(3), in their study of 200 terminally ill cancer patients, developed the only existing measure of desire for death among medically ill individuals of which we are aware. While the authors reported no data regarding the reliability or validity of this scale, the Desire for Death Rating Scale allows for clinician ratings of desire for death on a single 0–6 scale. Scores on this global clinician-rated scale are based on responses to open-ended questions such as “Do you ever wish that your life would end sooner?” It is interesting that Chochinov and colleagues dichotomized the patients into those with “significant desire for death” and those without, rather than analyzing desire for death as a continuous variable. Several important limitations are apparent in an ordinal rating scale such as the Desire for Death Rating Scale, including the reliance on clinician ratings. Researchers unfamiliar with this scale may have difficulty achieving reliability, and even with established interrater reliability within studies, different studies may interpret the rating scale differently. In addition, the limited range of possible scores (0 to 6) is problematic for many statistical analyses, such as examining differences within subjects scoring in the “normal” range (e.g., below 3) or in the “significant” range (3 and above).
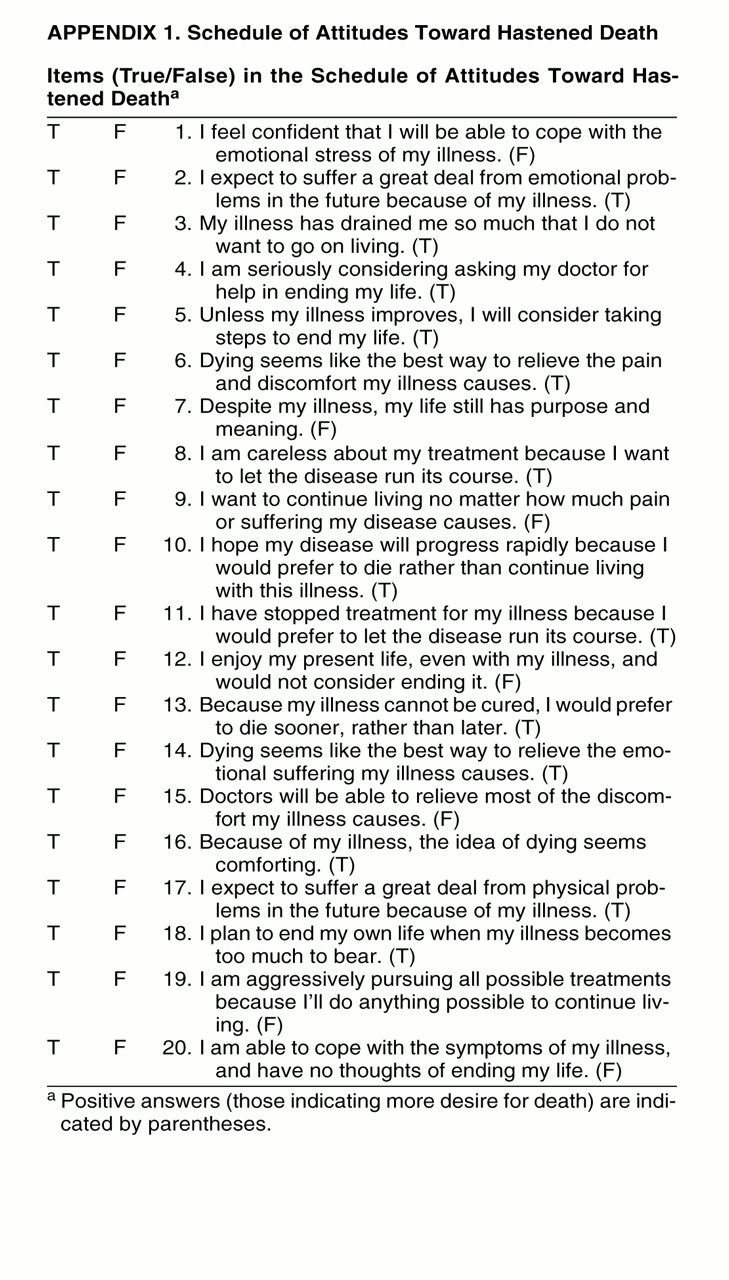
In response to these concerns, we developed the Schedule for Attitudes Toward Hastened Death, a brief self-report questionnaire designed to assess medically ill patients’ desire for hastened death. This questionnaire uses a true/false format and was intended to encompass several potential aspects of desire for death, including concerns regarding future quality of life (e.g., fear of pain or anticipated emotional suffering), social or personal factors that may influence one’s desire for death (e.g., religion, family obligations), and direct thoughts about or steps taken toward facilitating one’s own death. Such a measure has several advantages over global clinician ratings, including the potential for more varied, and possibly more accurate, measurement of the continuum of desire for death than can be achieved through a single clinical rating. In addition, the possibility for greater variation in desire-for-death ratings has important advantages for data analysis, and the self-report format is easier to use and standardize across settings and studies than is possible with a clinician rating scale.
This study presents initial validation data regarding the Schedule of Attitudes Toward Hastened Death. Along with performing reliability analyses, we compared scores on this measure to ratings on a clinician-rated measure of desire for death and several measures of psychological and physical symptom distress. Because we anticipated that desire for hastened death would be significantly associated with depressive symptoms for many patients, we expected moderate correlations between measures of depression and psychological distress. Similarly, we expected comparable associations between scores on this measure and measures of physical symptom distress.
METHOD
Initial questionnaire development began with the development of a pool of questions hypothesized to reflect different aspects of the construct of desire for hastened death. Repeated revisions of these questions, based in part on the feedback of a number of experts in the field of palliative care and consultation-liaison psychiatry (psycho-oncology, AIDS), ultimately yielded 30 questions. These questions reflected several aspects of the construct of desire for death, including an active desire for death, optimism/pessimism toward one’s future quality of life, social and personal factors that may influence willingness to consider assisted suicide or euthanasia, passive hopes for a more expedient death, and behaviors that might reflect a desire for death (e.g., preparing or revising one’s will, buying a copy of the book Final Exit). The questionnaire was designed in a dichotomous choice (true/false) format because we hypothesized that many specific thoughts or actions (e.g., “I am seriously considering asking my doctor for help in ending my life”) would be either present or absent. In addition, a true/false format was perceived by our panel of experts as a simpler, easier format for patients who are likely to be both psychologically and physically distressed, as well as burdened with other research tasks or instruments.
We then administered the scale to 55 patients with AIDS who were participating in a quality-of-life survey in order to elicit feedback regarding the clarity of writing, their level of discomfort in answering questions about death, and the relevance of the questions or frequency with which they were endorsed. On the basis of these preliminary data, five of the initial 30 items were deleted because of ambiguous wording and one item was rewritten to form two new items. Several items were retained in the scale despite being rarely endorsed because they appeared to most closely correspond to a high degree of desire for death if endorsed (e.g., “I am seriously considering asking my doctor for help in ending my life”). We also deleted six questions regarding actual behaviors that patients may have engaged in because of our observation (and the comments of respondents) that these items were not necessarily related to the construct in question. For example, several questions pertaining to end-of-life preparations (e.g., “I have recently made or revised my will or testament,” “I have preparations other than a will for after I die”) were thought to likely reflect a conscientious approach to living with a terminal illness rather than a desire for death. The remaining questions regarding actual behaviors were deleted (e.g., “I have pills or other means at home which I could use to end my life,” “I have already asked a friend or family member to help me end my life at some point”), despite appearing to reflect a desire for death. These questions were rarely endorsed by our pilot subjects and had little correlation with the total score on the Schedule of Attitudes Toward Hastened Death, and so, in light of the potential ethical problems if patients endorsed these items and later attempted suicide, these questions were omitted from the final scale. Thus, the resulting 20-item scale (appendix 1) was readministered to a new group of patients with HIV/AIDS in order to obtain the preliminary validation data described later in this article.
Participants
Patients with HIV/AIDS were recruited from two sources: ambulatory HIV-infected patients volunteering for participation in a double-blind, placebo-controlled trial of two pharmacological interventions for HIV-related fatigue (N=148) and terminally ill patients with AIDS admitted to a skilled nursing facility for end-of-life care who were participating in a study of the impact of protease inhibitors on quality of life (N=47). The study of HIV-related fatigue was approved by the Memorial Sloan-Kettering Cancer Center Institutional Review Board, while the latter study was approved by the Terrence Cardinal Cooke Health Care Center Institutional Review Board. All subjects provided written informed consent before participating in the study. Because of differences in the study design and methods, there was some variability in the measures included in these two studies. As a result, several of the analyses included only a subset of the total study group, although others included the entire, combined group.
Patients were excluded from participating in the study if they were under 18 years of age or unable to speak English fluently. In addition, brief cognitive assessments were conducted by using the Mini-Mental State
(4) in order to ensure that the patients were sufficiently intact cognitively to provide accurate information (patients scoring below 20 were excluded from study participation). Patients were also excluded from the outpatient group if they tested positive for substance abuse in urine toxicology screening. Patients were excluded from the inpatient group if they were too medically ill to complete testing or were not expected (by their attending physicians) to live longer than several days.
Procedures
Separate procedures were used for the two subgroups of patients who consented to participate in the study. All patients were interviewed by at least one member of the project staff in order to elicit background medical and social history, including demographic data, HIV transmission risk factor, religious affiliation, and prior mental health history.
After written informed consent was provided and the social/medical history interview took place, the ambulatory patients participating in the fatigue study were assessed with a series of clinician-rated instruments and self-report questionnaires. The clinician-rated instruments were the depression and substance abuse modules from the Structured Clinical Interview for DSM-IV (SCID)
(5) and the Karnofsky Performance Rating Scale
(6), a clinician-rated measure of overall physical functioning. The self-report instruments were the Beck Depression Inventory
(7), the Brief Symptom Inventory
(8), and the Medical Outcomes Study Health Survey
(9), a quality-of-life measure. The Schedule of Attitudes Toward Hastened Death was also administered to all subjects. Because many patients had visual problems and reading difficulties, all of the self-report instruments were read by the study investigator. In order to minimize potential bias, the clinician-rated instruments were completed before the self-report measures (e.g., Schedule of Attitudes Toward Hastened Death) were administered.
The patients in the palliative care group were also assessed with the SCID and the Karnofsky Performance Rating Scale, along with the Hamilton Depression Rating Scale
(10), a clinician-rated measure of depressive symptoms, and the Desire for Death Rating Scale
(3). The self-report measures included the Brief Pain Inventory
(11); the Memorial Symptom Assessment Scale
(12), which is a self-report inventory of 32 symptoms commonly associated with medical illness; and the Social Support Questionnaire
(13).
Statistical Analyses
Frequency analyses and descriptive statistics were used to assess the frequency of endorsement of the individual items on the Schedule of Attitudes Toward Hastened Death and the distribution of total scores. Reliability (internal consistency) was assessed by computing coefficient alpha and item-total correlations for the 20-item scale. Because the scores on the Schedule of Attitudes Toward Hastened Death were not normally distributed (description to follow), nonparametric statistics were used to assess associations between those scores and various demographic and clinical variables. Spearman correlation coefficients and Kruskal-Wallis tests were used to ascertain the strength of associations between total score on the Schedule of Attitudes Toward Hastened Death and the various measures used to establish concurrent validity. Finally, principal components factor analysis was used to ascertain whether any distinct factor structure existed within the 20-item Schedule of Attitudes Toward Hastened Death. Determination of the appropriate number of factors to interpret was established by examination of the scree plot and by examining the factor loadings from various alternative factor solutions.
RESULTS
Subject Characteristics
Of the 195 subjects included in these analyses, 64% were male (N=124) and 36% were female (N=71). The average age of the participants was 40.89 years (SD=7.9, range=25–67), and the average years of education was 12.18 (SD=2.3, range=3–20). The majority of subjects were African American (N=107, 55%), while 24% (N=46) were Hispanic and 17% were Caucasian (N=34). More than 50% of the participants (N=99) reported having been treated for a psychiatric disorder in the past, and 26% (N=50) reported at least one prior suicide attempt. The vast majority of patients were diagnosed with AIDS (79%, N=154).
Reliability
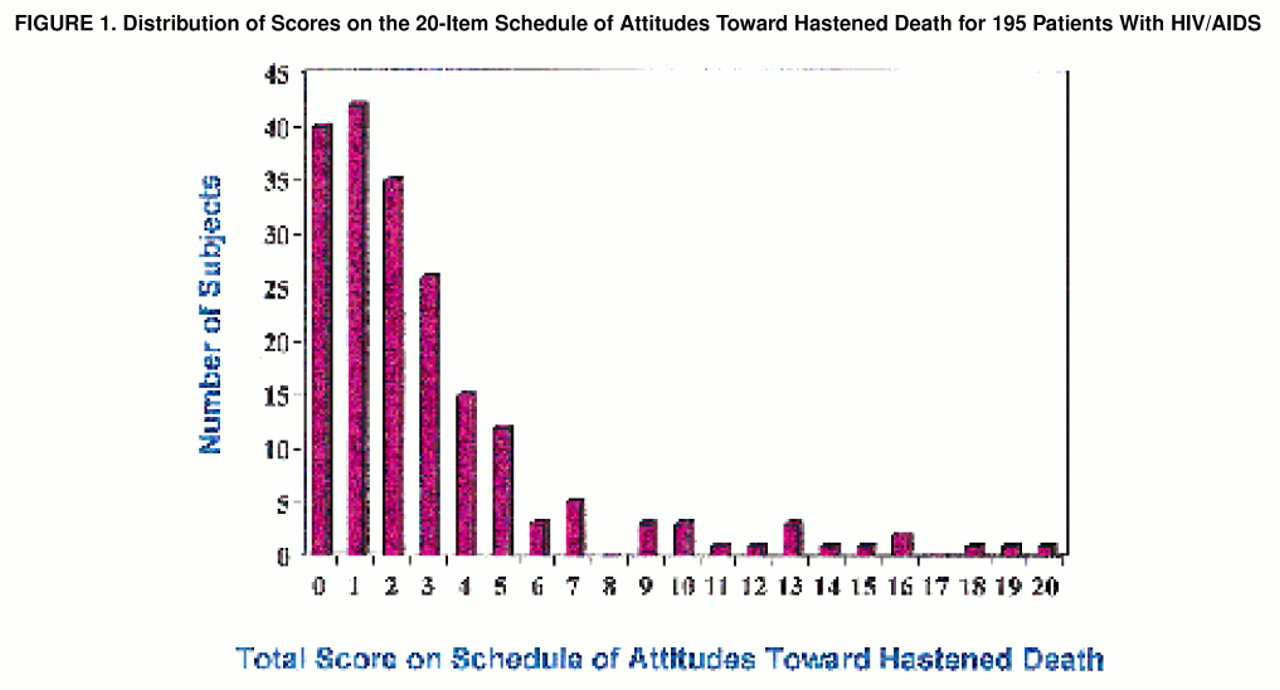
The total scores on the 20-item Schedule of Attitudes Toward Hastened Death ranged from 0 to 20, with a mean of 3.05 (SD=3.80) and a median of 2 (maximum possible range=0–20; 0=least desire for death). The distribution of scores was positively skewed, with few individuals endorsing large numbers of items and the majority of subjects (60%) endorsing 0, 1, or 2 items (
figure 1). Nearly three-quarters (73%) of the participants obtained a total score of 3 or less. The proportion of patients with a high level of desire for death depended on the cutoff score used. By using a liberal cutoff score, 7 or greater (more than one standard deviation above the mean), 12% of the subjects would be classified as having a high level of desire for death. A more conservative cutoff score, 11 or greater, resulted in the classification of 6% of patients as having a strong desire for death.
Many of the items on the Schedule of Attitudes Toward Hastened Death were infrequently endorsed; three items were endorsed by 10 or fewer patients, and only four items were endorsed by 25% or more. None of the items was endorsed by more than one-half of the patients. The most frequently endorsed items were “I expect to suffer a great deal from physical problems in the future because of my illness”—true (endorsed by 49% of the patients), “I expect to suffer a great deal from emotional problems in the future because of my illness”—true (endorsed by 39%), and “I want to continue living no matter how much pain or suffering my disease causes”—false (endorsed by 31% of the patients). The infrequently endorsed items included “I have stopped treatment for my illness because I would prefer to let the disease run its course”—true (endorsed by only seven patients, 4%), “I am seriously considering asking my doctor for help in ending my life”—true (endorsed by nine patients, 5%), “I hope my disease will progress rapidly because I would prefer to die rather than continue living with this illness”—true (endorsed by 10 patients, 5%), and “My illness has drained me so much that I do not want to go on living”—true (endorsed by 11 patients, 6%).
The overall internal consistency of the Schedule of Attitudes Toward Hastened Death was high; the coefficient alpha was 0.89. The adequacy of each individual item was established by examining the scale coefficient alpha with that item removed. None of the 20 items resulted in an increase in coefficient alpha by 0.01 or greater, and only three items increased the overall scale coefficient alpha at all. The greatest increase in coefficient alpha was 0.006, resulting from the removal of the item with the lowest item-total correlation, i.e., r=0.25. Similarly, the average item-total correlation for the 20 items was 0.53, with a range of 0.25 to 0.74. Seventeen of the 20 items on the Schedule of Attitudes Toward Hastened Death had item-total correlations of 0.40 or greater, and eight exceeded 0.60.
Validity
Investigation of the demographic and medical variables associated with the total score on the Schedule of Attitudes Toward Hastened Death revealed few significant differences. There were no differences in total scores with regard to gender (Kruskal-Wallis χ2=0.59, df=1, p=0.44), race (Kruskal-Wallis χ2=6.40, df=3, p=0.09), or HIV transmission risk factor (Kruskal-Wallis χ2=5.30, df=3, p=0.15). There was no significant correlation between total score on the Schedule of Attitudes Toward Hastened Death and age (r=–0.11, N=195, p=0.11), education (r=0.07, N=193, p=0.36), or CD4+ cell count (r=–0.09, N=188, p=0.26). There was also no difference in scores among patients of different religious backgrounds (Kruskal-Wallis χ2=0.05, df=3, p=0.97). Although the mean scores differed substantially between the two research sites (2.67 for the ambulatory patients and 4.26 for the inpatients), this difference was not statistically significant (Kruskal-Wallis χ2=1.10, df=2, p=0.29) (although this difference was statistically significant when a t test was used to compare mean scores, the more conservative Kruskal-Wallis test did not demonstrate a significant difference between ranked scores).
The total score on the Schedule of Attitudes Toward Hastened Death was significantly correlated with measures of depression and psychological distress. For example, it was significantly correlated with the score on the Beck Depression Inventory (r=0.43, N=112, p<0.0001), the score on the global severity index of the Brief Symptom Inventory (r=0.42, N=112, p<0.0001) and the Hamilton depression score (r=0.51, N=47, p<0.0003). Patients with a history of psychiatric treatment had a significantly higher mean score on the Schedule of Attitudes Toward Hastened Death than did patients without a history of prior psychiatric treatment (3.90 versus 2.16) (Kruskal-Wallis χ2=10.64, df=1, p<0.002). Patients reporting a history of at least one prior suicide attempt (N=50) also had a significantly higher score than did patients without such a history (4.58 versus 2.45) (Kruskal-Wallis χ2=7.18, df=1, p<0.008).
The patients receiving palliative care (N=47) also were examined with the Desire for Death Rating Scale. Scores on this clinician-rated measure ranged from 0 to 6 (possible range=0–6, 0=no desire for death), with an overall group mean of 1.19 (SD=1.65). One-half of this subgroup had scores of 0, while seven patients (15%) received ratings of 3 or greater, defined by Chochinov and colleagues
(3) as reflecting a “serious and pervasive” desire for death (the remaining 17 patients were given ratings of 1 or 2, reflecting mild or moderate desire for death). The correlation between the rating on the Desire for Death Rating Scale and the total score on the Schedule of Attitudes Toward Hastened Death was statistically significant (r=0.69, N=47, p<0.0001).
The score on the Memorial Symptom Assessment Scale global distress index, a measure of physical symptom distress, was also significantly correlated with the total score on the Schedule of Attitudes Toward Hastened Death (r=0.38, N=46, p=0.01). In addition, the subset of patients who reported pain revealed a significant correlation between pain intensity (with a 0–10 rating scale) and total score on the Schedule of Attitudes Toward Hastened Death (r=0.51, N=31, p<0.004). Surprisingly, the total score on the Schedule of Attitudes Toward Hastened Death was not significantly correlated with the patient rating of satisfaction with social supports based on the Social Support Questionnaire (r=–0.15, N=46, p<0.32).
Factor Analysis
Principal components factor analysis revealed a unidimensional factor structure to the Schedule of Attitudes Toward Hastened Death. Review of the scree plot, along with the factor loadings from various alternative solutions (using varimax rotation), indicated that a single factor best accounted for the variance in scores. This single-factor structure is consistent with the already-noted reliability analyses in which no items significantly raised the overall coefficient alpha and the item-total correlations were all uniformly high. Thus, despite our intent to sample various domains of attitudes in the Schedule of Attitudes Toward Hastened Death that might result in multiple discreet factors, no such solution was evident.
DISCUSSION
The measurement of desire for hastened death has become an increasingly important component of research on factors contributing to interest in assisted suicide and euthanasia. Here we present preliminary validation data on a newly developed research instrument, the Schedule of Attitudes Toward Hastened Death. It is a reliable and valid self-report measure assessing desire for hastened death among patients with HIV/AIDS. Reliability analyses demonstrated a high degree of internal consistency in this measure and strong item-total correlations, suggesting that the measure likely taps a single, unidimensional construct. This measure offers several advantages over the only existing measure designed to tap a similar construct, the Desire for Death Rating Scale
(3). Unlike that instrument, which relies on clinician estimates of the degree of desire for death along a single 0–6 scale, the Schedule of Attitudes Toward Hastened Death allows for greater variability in desire-for-death ratings, which may be meaningful in future research. This measure allows for potential comparisons between individuals with low, moderate, and high levels of desire for death, and further research with larger and more heterogeneous samples may yield meaningful factors within the overall construct of desire for death.
Concurrent validity analyses followed an expected pattern of results, demonstrating that the total score on the Schedule of Attitudes Toward Hastened Death was highly correlated with the rating on the Desire for Death Rating Scale, a clinician-rated measure of desire for death. In addition, the score on the Schedule of Attitudes Toward Hastened Death was significantly correlated, although somewhat less so, with several measures of depression and overall psychological distress (e.g., the Beck Depression Inventory, Brief Symptom Inventory, and Hamilton depression scale). As expected, the scores on the Schedule of Attitudes Toward Hastened Death were significantly higher among patients with prior histories of psychiatric treatment or suicide attempts, demonstrating some sensitivity of this measure to overall psychological distress. These relatively modest associations, however, also support the discriminant validity of the Schedule of Attitudes Toward Hastened Death, demonstrating that it is not merely a proxy for psychological distress but, rather, is likely influenced by depression and distress. Several other findings, such as the significant correlation of desire for death with pain intensity and physical symptom distress, while consistent with expectations, included a relatively small subset of the overall study group and must therefore be considered preliminary.
Despite this limited number of subjects for some analyses, the observed findings are consistent with our expectations regarding anticipated associations with a measure of desire for death, and they support the construct validity of this self-report instrument. Several limitations must nevertheless be acknowledged. First, this study included only patients with HIV/AIDS and these findings may not generalize to populations with other chronic or life-threatening medical illnesses, such as cancer or multiple sclerosis. Patients with AIDS are somewhat unique with regard to demographic and background characteristics, overrepresenting minority individuals, those with a history of drug use, and persons of lower socioeconomic background. It is possible that similar analyses with other subject populations may yield somewhat different results—for example, indicating a more distinct factor structure than was apparent in our study group. Moreover, this study lacked any formal control group against which to compare the patients with AIDS. Because of the nature of the questionnaire, any “control group” must have a chronic, if not terminal, illness in order for the questions to be meaningful. Instead of attempting to contrast patients with AIDS against another medically ill group, however, we compared patients at a relatively early stage of disease with those in a terminal stage, finding, as expected, that patients in later stages of disease scored substantially higher on the Schedule of Attitudes Toward Hastened Death than ambulatory patients (although the difference was not statistically significant when we used a conservative nonparametric statistical test, the size and direction of the group differences were consistent with expectations). In addition, as treatments for HIV/AIDS continue to evolve, the proportion of patients expressing a desire for death and the relationships between desire for death and psychological/social variables may change. These limitations further highlight the need for additional research, both with HIV/AIDS patients and with patients diagnosed with other terminal and chronic illnesses.
Another limitation in these data pertains to the modest number of subjects available for many statistical tests. Because several measures were administered only to a subset of patients, many analyses included relatively small groups (e.g., correlations with the Desire for Death Rating Scale and Brief Pain Inventory). In addition, we were unable to use multivariate analyses to assess many interrelationships among variables that might have yielded interesting findings (although not central to the focus of this manuscript). For example, path analyses may be helpful in assessing whether there are more complicated relationships between pain, physical symptom distress, psychological distress, social support, and desire for death. It is certainly plausible that desire for death is related to different causal factors among different subgroups of terminally ill patients, and multivariate analyses (e.g., cluster analysis, path analysis) may reveal more complex relationships. This study, however, was intended not to determine the factors predictive of desire for death, but merely to assess the utility of a self-report measure for assessing desire for death.
Our interest in developing the Schedule of Attitudes Toward Hastened Death was to create a research tool for assessing the degree of desire for death, rather than a clinical tool to determine or predict who may or may not request assistance in dying. Although future research may demonstrate this to be a useful clinical instrument capable of predicting requests for assisted suicide or identifying patients with a significant desire for death who require more aggressive clinical interventions, we suggest that no evidence to support such uses currently exists. In the process of examining responses to the Schedule of Attitudes Toward Hastened Death, we did attempt to identify appropriate cutoff scores that would be helpful in determining which patients have a strong desire for death. These cutoff scores, however, are not intended to be used clinically, in an effort to determine whether a patient is likely to request assistance in dying (e.g., physician-assisted suicide or euthanasia) or whether such requests are “appropriate.” Indeed, our data suggest that while high scores on the Schedule of Attitudes Toward Hastened Death may correspond to a substantial desire for hastened death, this desire may be largely influenced by depression for many patients (as evidenced by the significant correlation between the score on the Schedule of Attitudes Toward Hastened Death and the level of depressive symptoms). Thus, while the Schedule of Attitudes Toward Hastened Death may have some clinical utility in facilitating a discussion of end-of-life issues between patients and health care providers, this measure is not intended to differentiate “rational” and “irrational” interest in hastened death or appropriate and inappropriate requests for assisted suicide.
In addition, choice of appropriate cutoff scores may differ depending on the purpose of the research. For example, investigators seeking to better understand desire for hastened death may desire a lower cutoff score to obtain a subgroup that includes individuals with even mild levels of desire for death. Researchers attempting to identify individuals likely to request or seriously consider assisted suicide or euthanasia, on the other hand, may wish to use a substantially higher cutoff score. Regardless of the use or validity of alternative cutoff scores, the potential clinical utility of the Schedule of Attitudes Toward Hastened Death as a means of facilitating discussion of end-of-life issues is supported by our observation that the participants reported little difficulty or distress while answering these seemingly sensitive questions. In fact, of the 195 participants, only three expressed a feeling that the questionnaire was upsetting and many more expressed relief or gratification that they were able to address these issues directly. Thus, health care providers may find that this instrument offers an alternative method for broaching end-of-life issues that are often difficult to discuss more directly.
Despite the limitations in this research, we believe these analyses demonstrate that the Schedule of Attitudes Toward Hastened Death is a useful, valid instrument for measuring desire for death among patients with HIV/AIDS and may have more general utility with other medically ill populations. Further research with this measure may be invaluable in addressing many of the unanswered questions emerging from the ongoing debates regarding legalization of assisted suicide. Moreover, this type of information will be essential in informing the development of guidelines for any future legislation or policies regarding legalization of assisted suicide. Only with adequate methods of measuring patient interest in hastened death can we answer such critical questions as what factors increase desire for death and what interventions (if any) decrease this desire. These and many other end-of-life questions require immediate attention in order to improve the quality of life of terminally ill patients and allow for informed decision making regarding such important public policy questions.
APPENDIX 1