Studies to date suggest high levels of psychological distress in cardiac arrest survivors, particularly phobic anxiety and panic symptoms, in the early stages of adaptation
(3–
6). Investigators have also found that survivors use strong defense mechanisms to protect themselves from the overwhelming anxiety engendered by the implications of the event. Whether these coping strategies remain effective over time or lead to maladjustment is less clear. Data on long-term adaptation are rare and provide conflicting evidence about the amount and severity of emotional disability
(7–
9). The first aim of the present study, therefore, was to compare the long-term prevalence and severity of emotional disability in cardiac arrest survivors with that of cardiac patients whose course was not complicated by cardiac arrest.
Cardiac arrest survivors manifesting symptoms of intrusion, avoidance, and hyperreactivity may have failed to integrate and resolve the trauma
(16). On the other hand, suffering from involuntary intrusive memories of the cardiac arrest event may have become part of the individual biography of the patients without leading to a clinically relevant dysregulation. Patients who manifest avoidance behavior (when exposed to stimuli that remind them of the resuscitation) may also be able to go on with their lives on an acceptable basis
(17). The third aim of the present study was to ascertain whether patients who suffer from traumatic symptoms, mainly intrusion and avoidance, exhibit higher degrees of affect dysregulation and maladaptation than those who are not haunted by the memories of what happened to them.
RESULTS
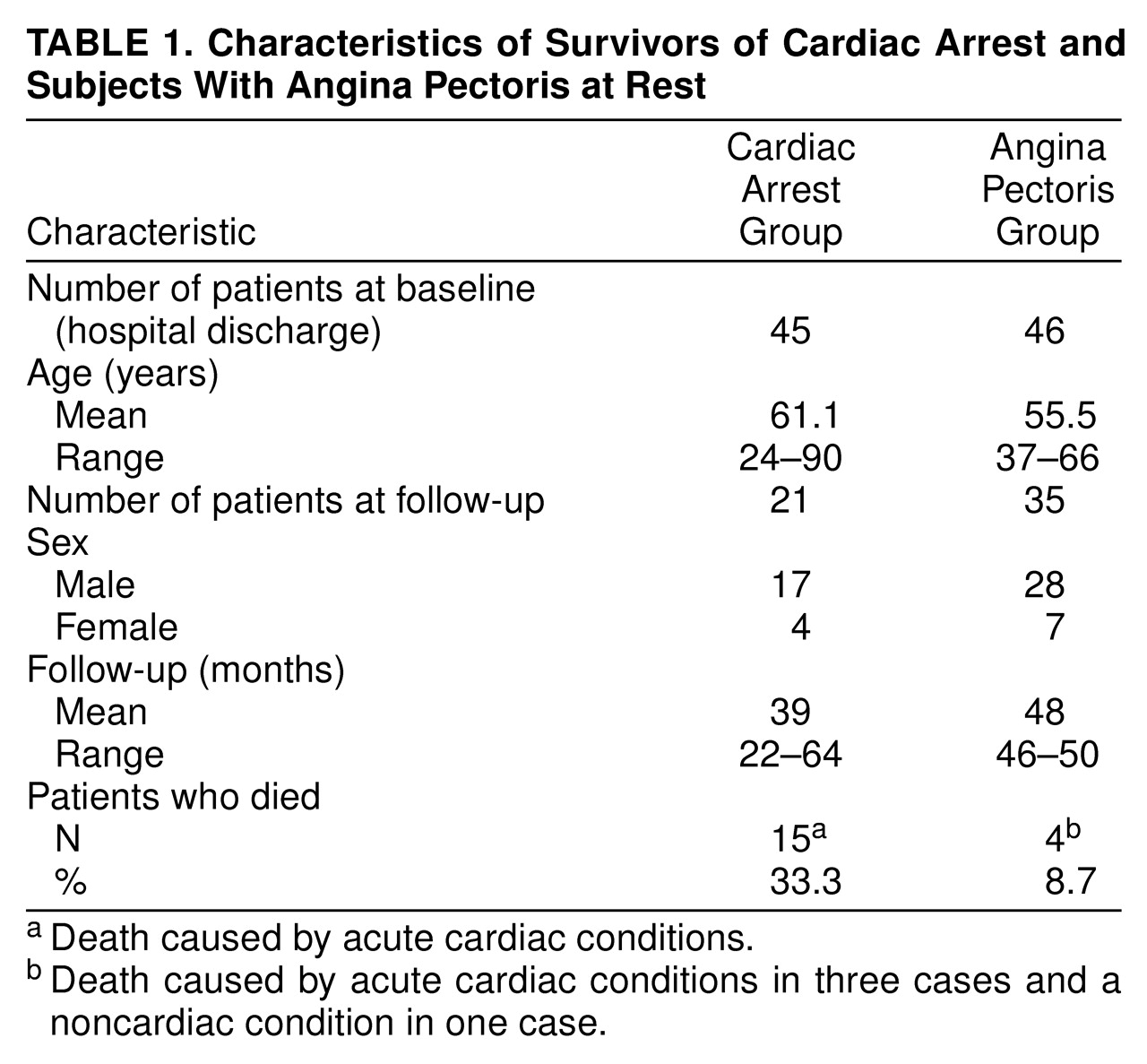
Twenty-one survivors of cardiac arrest outside the hospital were assessed within a mean interval of 39 months (range=22–64) after the life-threatening event. The study population achieved high levels of emotional stability and well-being: 15 (75%) of the patients were found to be in the normal range of both the depression and anxiety subscales of the Hospital Anxiety and Depression Scale (score of 9 or less). The index population’s mean depression score (5.3, SD=4.5) exceeded only slightly that of the German standard cardiac population (5.0, SD=3.7). The mean anxiety score was lower in the cardiac arrest group (5.5, SD=4.4) than in the reference population (6.8, SD=4.1).
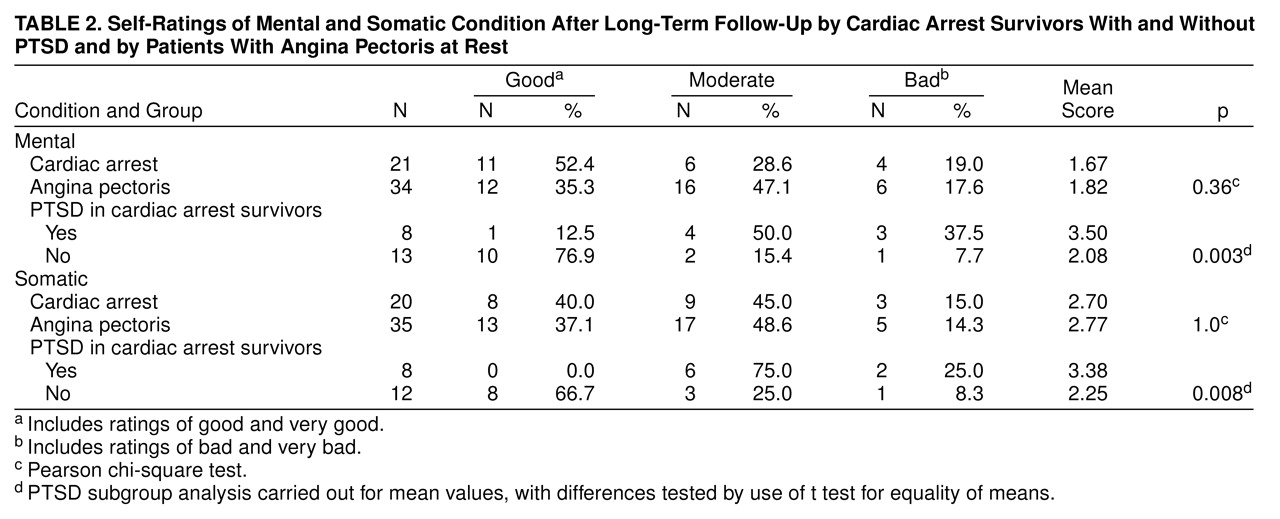
We compared the follow-up status of the index patients and 35 coronary artery patients with severe symptoms of angina pectoris at illness onset and found that the cardiac arrest group exhibited no significant differences in self-estimates of their overall mental and somatic condition (
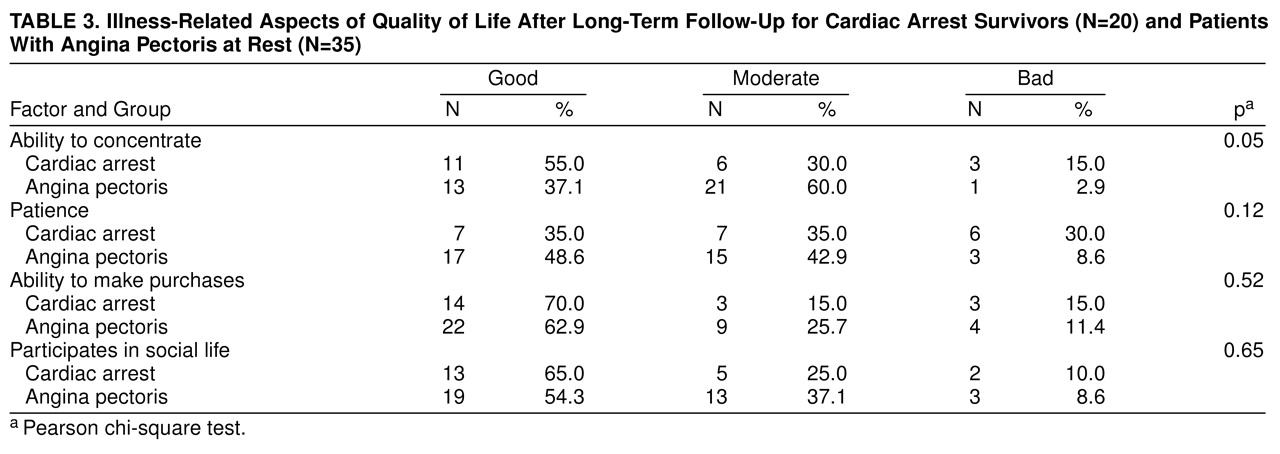
Table 2) or in illness-related aspects of quality of life (
Table 3). In addition, no significant differences concerning various aspects of sleeping disorders could be detected. Of all the factors that were measured in the cardiac arrest survivors and the coronary artery comparison group, only the ability to concentrate reached a significant difference. It was impaired in the index group in comparison to the coronary artery group (χ
2=5.8, df=2, p<0.05).
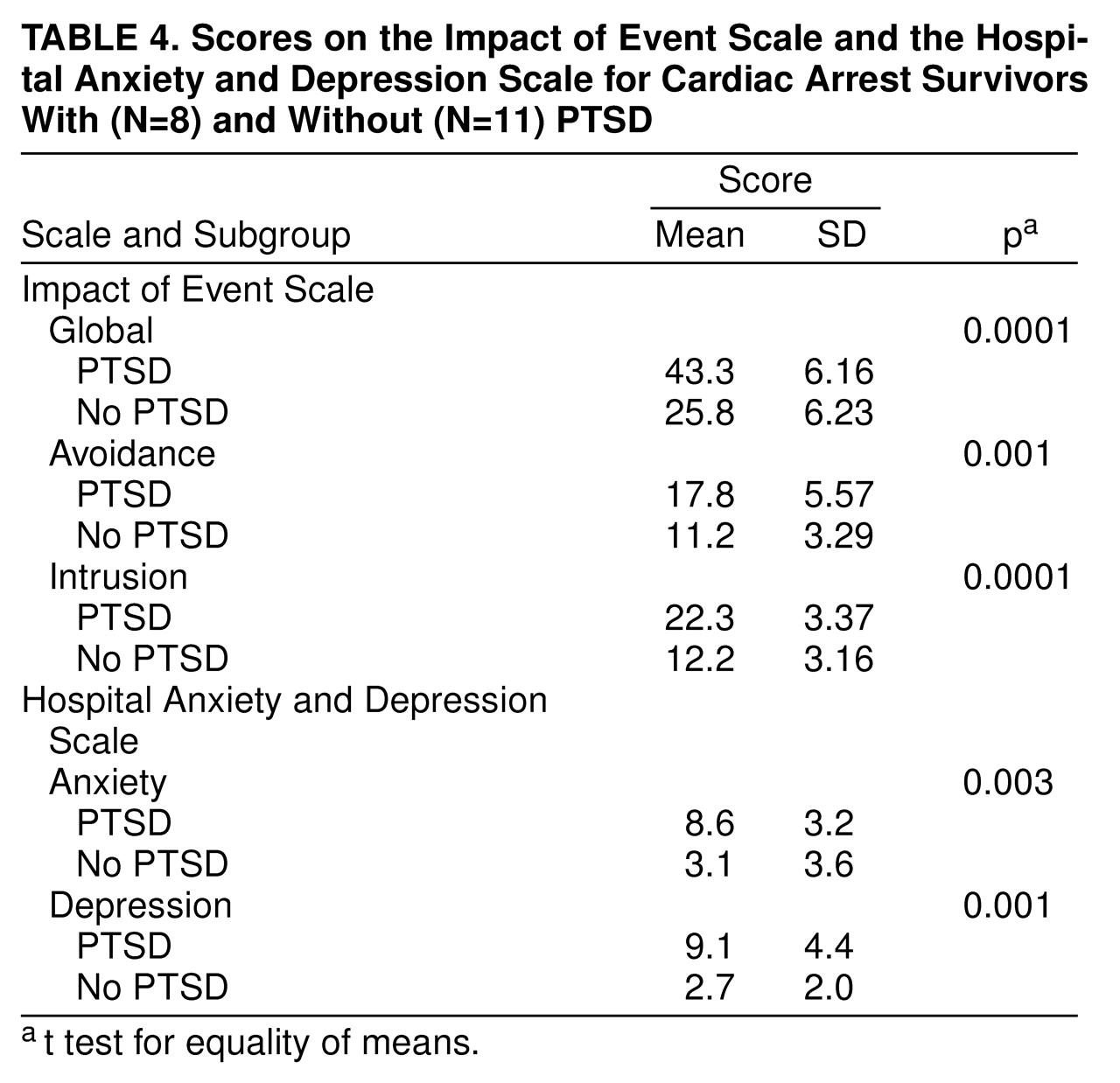
Despite this apparently favorable overall adaptation in the long-term course after the breakdown situation, more than 50% of the cardiac arrest survivors (N=11) claimed that the event had significantly changed their lives. With the help of the Impact of Event Scale, patients who had high scores (N=8) and low scores (N=13) on intrusive thoughts and avoidant states were separated in the cardiac arrest group.
Table 4 shows that the procedure to define the PTSD group led to a significant difference in the global Impact of Event Scale score (t=–7.07, df=17, p<0.0001), as well as in the avoidance subscale score (t=–3.19, df=17, p<0.001) and the intrusion subscale score (t=–7.34, df=17, p<0.0001). Furthermore, patients with PTSD had a higher mean score on increased arousal (9.88, SD=3.56) than patients without PTSD (5.82, SD=5.82). The difference was statistically significant (t=–2.33, df=17, p<0.03).
Patients with PTSD had significantly higher mean scores on depression (t=–4.46, df=18, p<0.003) and anxiety (t=–3.48, df=18, p<0.003) than their counterparts (
Table 4). Self-estimates of the patients’ mental and somatic condition were also significantly impaired in the PTSD group compared to the group without PTSD (
Table 2), as were beliefs concerning an optimistic future course of the disease condition (negative in six [75%] of the PTSD patients and three [27%] of the non-PTSD patients, χ
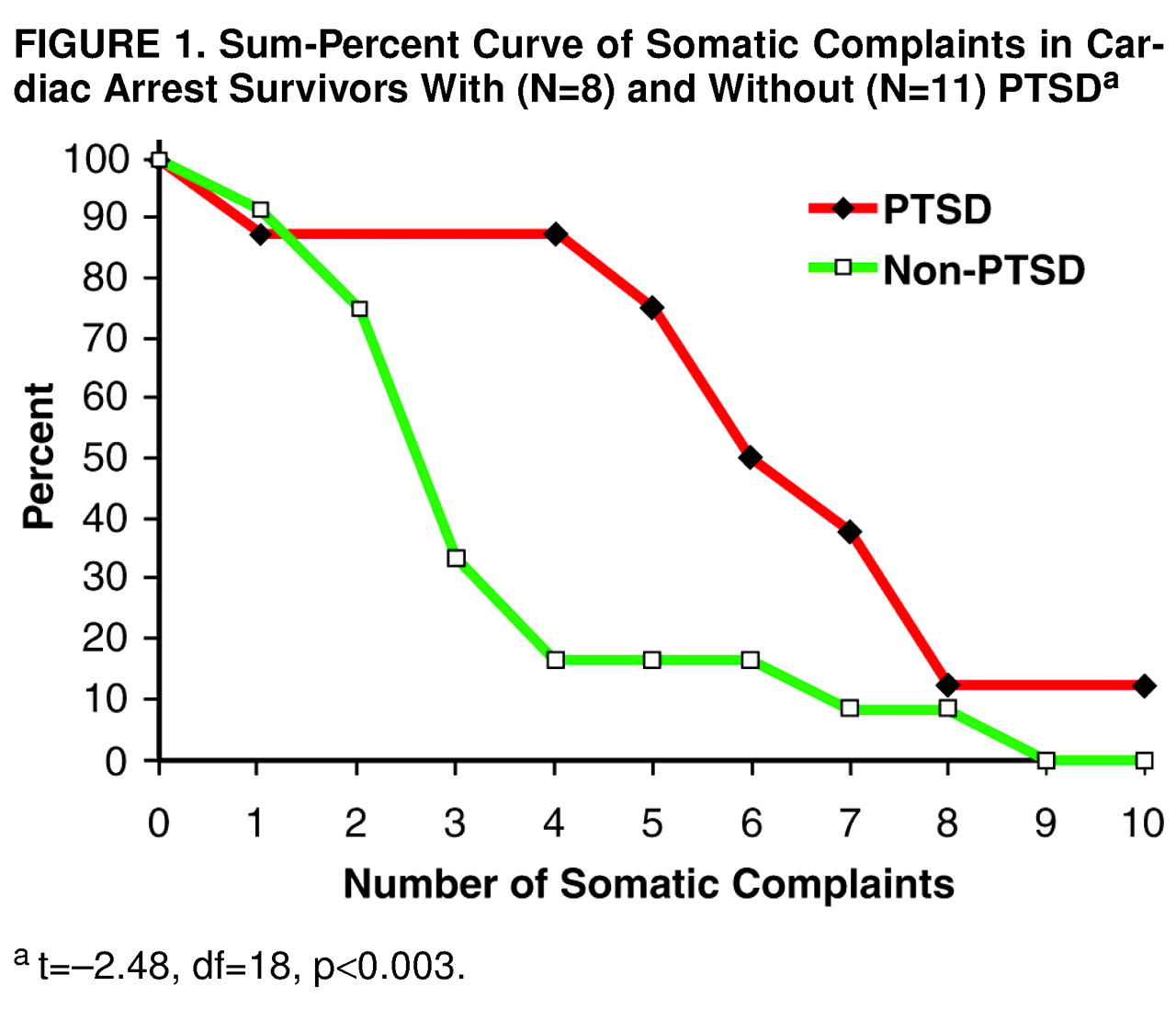
2=4.23, df=2, p<0.04). Patients with PTSD had a significantly lower score than non-PTSD patients in ability to concentrate (mean=2.75, SD=1.03, versus mean=3.91, SD=0.67; t=3.08, df=18, p<0.006). Accordingly, preoccupation with somatic complaints was significantly more pronounced in the PTSD group (t=3.00, df=18, p<0.008).
Figure 1 displays the difference between the two groups as a sum percent curve for the 10 items of the complaint scale.
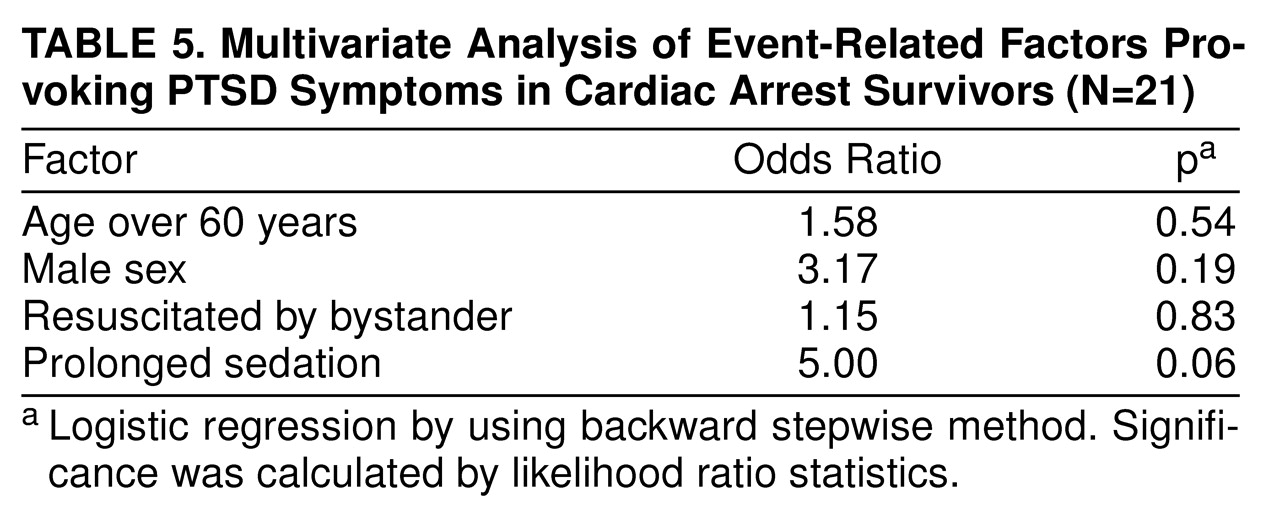
We analyzed whether age, sex, and selected factors of the resuscitation and procedures on the scene of the collapse contributed to the risk of developing PTSD symptoms. The following factors were rejected by the multivariate model: onset of event during daytime/nighttime, call response time more than 8 minutes, more than four shocks delivered, and no return of spontaneous circulation before arrival of the emergency physician. We found that sedation at illness onset significantly predicted a favorable outcome (
Table 5). In these patients, the risk of developing PTSD symptoms was fivefold lower than that in their counterparts.
DISCUSSION
The present study reveals that the prevalence of emotional disability and impairment in quality of life in cardiac arrest survivors is similar to that of cardiac patients whose clinical course was not complicated by cardiac arrest. Five patients (25%) in the present study qualified for moderate to severe forms of depression. Severe forms of depression in cardiac patients, as assessed with various instruments, have been reported to range from 15% to about 25%
(29–
31). Data on the maintenance of depressive symptoms in cardiac arrest survivors over more than a 1-year observation period have not been available in the literature until now. The present 3-year follow-up results are in line with the study of Roine et al.
(32), which revealed initially high degrees of depression in hospitalized cardiac arrest survivors and confirmed a steep decline in prevalence rates over 1 year. Bedell et al.
(33) followed in-hospital cardiac arrest survivors for 6 months and also found that they were severely depressed at the time of discharge from acute hospital care. Six months later, the patients’ mean depression score had fallen significantly and was within the range of scores for a normal community population.
Unexpectedly, the prevalence of patients who were incapacitated by fear was also low: the mean anxiety score was even lower in the cardiac arrest group (5.5, SD=4.4.) than in the reference population (6.8, SD=4.1). There were only a few patients in whom the fear of another cardiac arrest led them to regulate their daily lives and limit their activities to ensure immediate access to medical care. Considering that the fatality rate is far higher in cardiac arrest survivors than in patients with angina pectoris at rest (a fatality rate after hospital discharge of 33% in the present cardiac arrest group versus 8.7% in the comparison group), this is a remarkable finding. It proves that the majority of patients have successfully maintained or have rebuilt effective coping resources. This finding is shared by other investigations
(34–
37). Hillis et al.
(35) did not find any behavioral or emotional differences between cardiac arrest survivors and patients with coronary artery disease. Miranda
(38) and Sunnerhagen et al.
(9), however, did not confirm these favorable results. They revealed a diminished personal interest in the environment and an increased sense of disorientation in cardiac arrest survivors. Sauvé
(39) reported elevated scores for psychological distress in 61 cardiac arrest survivors 6 months to 4 years after cardiac arrest.
Low levels of impairment and the lack of significant differences between the index and comparison groups also hold true for all further affective, biobehavioral, and cognitive patient variables that were assessed in the present study (sleeping disorders, social activities, health beliefs). Among quality-of-life variables, the ability to concentrate was the only factor that was scored significantly lower in cardiac arrest survivors than in the comparison group. This finding confirms earlier investigations by Hillis et al.
(35), Sauvé
(39), Bertini et al.
(40), and Grubb et al.
(41), who also found more difficulties with memory and concentration in cardiac arrest patients than in patients with acute myocardial infarction. Beuret et al.
(42) also found that persistent mild memory disturbances were common in this patient group but did not preclude adequate professional activity and positive life perception. Those results are encouraging because they confirm the beneficial consequences of resuscitation efforts for the majority of discharge-to-hospital survivors of a cardiac arrest.
The favorable outcome in psychodiagnostic assessment that has been shown in previous studies
(8,
9,
33,
42) may be still somewhat surprising in the light of what these patients experienced. Undoubtedly, patients who survive cardiac arrest outside a hospital face an event that is outside the range of usual human experience, and the aftermath of this event would be distressing to almost anyone. Such a characterization meets the key criterion for definition of a traumatic event (in ICD-10 and DSM-IV) that may provoke PTSD. Surprisingly, there are no data available that have considered the experience of surviving a sudden cardiac arrest as a traumatic event. This study is, to our knowledge, the first one to show that evidence of the breakdown is present in a considerable proportion of survivors in the long-term course after the cardiac arrest experience and leads to recurrent and intrusive recollections of the event and to avoidance behavior in a clinically relevant number of cases.
Psychic fixation on the traumatic event may not be surprising, considering the severity of the arrest experience. The event may have become part of the patient’s individual biography without harming the subject any further. The present study revealed, however, that patients who maintained high scores of intrusion and avoidance behavior concerning the cardiac arrest experience over a long time period apparently failed to integrate the memory of the event into their preexisting schemata
(12,
13) and suffered from a serious affective dysregulation and a pronounced impairment in quality of life. Patients with PTSD symptoms exhibited significantly higher degrees of depression and anxiety and a diminished capacity to resist emotional burden
(43). They reported an enduring sense of demoralization with lack of confidence in the future and low estimates of their mental and somatic condition.
Moreover, PTSD sufferers were preoccupied by negative health beliefs, and they exhibited more somatic complaints than patients without PTSD. This finding confirms a number of studies that have noted an increased reporting of physical symptoms in patients with PTSD
(44,
45). It is unlikely that the underlying disease condition is responsible for the difference in symptom reporting because all patients had experienced the same life-threatening coronary event. McFarlane et al.
(45) assumed that the physical symptoms may be related to the high levels of arousal that form part of the symptom complex of PTSD. The pronounced awareness of endogenous somatic signals may be due to an impaired ability to process and differentiate relevant and irrelevant information.
PTSD symptoms may interact with the clinical conditions of cardiac arrest survivors in several ways. First, persistently impaired memory and concentration are widely confirmed as core symptoms in cardiac arrest patients
(35,
39–
42). More recently, alterations in memory functions have also been shown in PTSD patients
(46,
47). Cardiac arrest patients with PTSD symptoms in the present study had significantly lower concentration scores than cardiac arrest patients without PTSD symptoms. PTSD may thus amplify disturbances in cognitive functions. We used stepwise logistic regression analysis in the present study to identify the contribution of major resuscitation variables to the prediction of PTSD symptoms and could not find a significant association, indicating that it is not likely that the PTSD patients were exposed to more ischemia than non-PTSD patients. It cannot be ruled out completely that patients with PTSD symptoms suffer from more severe brain damage than their counterparts. Moreover, brain damage may be subtle and may preferentially hit areas of the brain that relate to emotional regulation. It has, in fact, been shown that ischemic damage causes selective vulnerability to the brain, with a preponderance of neural loss in region CA1 of the hippocampus
(48).
Second, PTSD is strongly associated with symptoms of alterations in sympathetic functions
(49). A growing body of evidence indicates that PTSD is associated with increased noradrenergic responsiveness in cardiovascular measures such as heart rate, blood pressure, and norepinephrine response to traumatic reminders
(50). It is well established that a markedly elevated baseline level of sympathetic neural outflow is a risk factor for derangements in heart rhythm
(51) and heart failure
(52) and a key trigger of myocardial ischemia during daily life
(53). Thus, PTSD may act as a major coronary risk factor in long-term course after cardiac arrest survival.
Not all patients suffered from PTSD-like symptoms. Obviously, the cardiac arrest event did not evoke symptoms of distress in all patients, or stress responses were not maintained over the long-term course. This phenomenon underlines the fact that PTSD is not simply a function of the experience itself but may be attributed either to factors associated with the emergency situation and/or to adaptive capabilities of the cardiac arrest victim. It is likely that a premorbid history of affect dysregulation amplifies the risk for developing PTSD
(54). In the present study, no data were available concerning personal coping abilities and personality factors of the affected patients. However, the data set allowed the estimation of the contribution of specific stress factors around the breakdown situation and revealed that prolonged sedation in the initial phase of resuscitation was a significant protective factor. It may be speculated that prolonged sedation helped to inhibit imprinting the actively troublesome and painful dimension of the event
(16,
47). There was, indeed, a marked difference in the duration of unconsciousness in the group that received sedatives (N=7) and the group that did not (N=13) (mean=618.2 minutes, SD=2205, and mean=92.1 minutes, SD=84, respectively) (p=0.01, t test for equality of means, two independent groups). Conscious processing of overwhelming adverse stimuli was inhibited during the most vulnerable stage of the disease onset. Patients were thus provided with a considerable time delay to deal with all the implications of what had happened to them, awakening within surroundings that apparently generated positive outcome expectancies.
The present study shows that the amount of emotional disability in patients surviving an out-of-hospital cardiac arrest is comparable to that in cardiac patients whose illness onset was not complicated by a comparable vital threat. However, when patients were grouped according to persistent intrusion and avoidance behavior concerning the traumatic event, it became evident that the prevalence of affective disability and behavioral maladaptation was significantly concentrated in the group suffering from PTSD-like symptoms. The application of the PTSD paradigm contributed convincingly to defining the patient population at risk for a persistent serious affective disturbance.
A major limitation of the present study is the small size of the patient population, which may provoke false negative results because of type II errors. Moreover, there are no norms and no defined cutoff points for a strict definition of PTSD. Pathologic autonomic nervous system arousal is considered to be a major key clinical feature of PTSD and is only phenotypically registered in the present study (sleeping disorders, irritability, difficulties to concentrate). Future studies should assess the degree of functional hypersensitivity and ergotropic tonus.
The encouraging results of the present study need to be confirmed in larger patient groups and may also stimulate prospective studies that address the time-dependent course of maladaptation and affective disability (including issues of critical onset during the adaptation process) and predictors for maintenance of psychic trauma in cardiac arrest survivors. The possible interaction between discrete cognitive abnormalities, which may be part of the PTSD syndrome, and emotional disability in cardiac arrest survivors also requires scientific attention before conceptualizing treatment regimes for these patients.
ACKNOWLEDGMENTS
The following hospitals in the city of Munich took part in the study: Stiftsklinik Augustinum (Prof. Dr. v. Essen, OA Dr. Reimer), Krankenhaus Dritter Orden (OA Dr. Schwarzfischer), Klinik Josephinum (Dr. Wildfeuer), Krankenhaus Neuwittelsbach (Prof. Dr. Scherer), Kreiskrankenhaus Pasing (Prof. Dr. Luther, Dr. Gutsch), Kreiskrankenhaus Perlach (Dr. Burghardt), Städtisches Krankenhaus Bogenhausen (Prof. Dr. Delius), Städtisches Krankenhaus Harlaching (Prof. Dr. Lindlbauer, OA Dr. Scheinpflug), Städtisches Krankenhaus Neuperlach (Prof. Dr. Henselmann, OA Dr. Fischer), Städtisches Krankenhaus Schwabing (Prof. Dr. Döring, OA Dr. Ohly), Medizinische Klinik Innenstadt der Ludwig-Maximilians-Universität (Prof. Dr. Theisen, OA Dr. Scheininger), Chirurgische Klinik der Ludwig-Maximilians-Universität (Prof. Dr. Schweiberer, OA Dr. Höcherl), Klinikum Großhadern der Ludwig-Maximilians-Universität (OA Dr. Jänicke), Klinikum Rechts der Isar der Technischen Universität München (Prof. Dr. Schömig).