Adaptive changes in γ-aminobutyric acid (GABA) systems contribute to ethanol tolerance, dependence, and withdrawal
(1,
2). Clinical studies have shown low plasma GABA levels during withdrawal, although this finding has been inconsistently replicated in studies of GABA levels in cerebrospinal fluid
(3,
4).
GABA function has been implicated in hepatic encephalopathy because of the efficacy of benzodiazepine antagonists in ameliorating cognitive impairments related to hepatic encephalopathy
(5). However, postmortem studies have revealed no abnormalities in GABA levels
(6).
We believe the current study to be the first attempt to measure in vivo abnormalities in the total cortical level of GABA plus homocarnosine in patients with alcohol dependence or hepatic encephalopathy by means of proton magnetic resonance spectroscopy (1H-MRS).
METHOD
MRS was performed on healthy subjects (N=10), recently detoxified alcohol-dependent patients (N=5), and patients with hepatic encephalopathy (N=5). The healthy subjects had a mean age of 35 years (SD=7). They completed a clinical assessment that excluded current medical, psychiatric, and substance abuse diagnoses; five also completed additional clinical and neuropsychiatric assessments.
Alcohol-dependent patients were recruited from the Substance Abuse Program of the VA Connecticut Healthcare System, West Haven, Conn., and met the DSM-III-R criteria for alcohol dependence on the basis of a structured clinical interview
(7). Other than tobacco dependence, they had no other lifetime substance dependence diagnoses. They completed MRS testing 34 days (SD=20) from their last drink. Two patients receiving benzodiazepines were scanned 3 weeks from their last dose. The alcohol-dependent patients had a mean age of 46 years (SD=11), experienced the onset of alcoholism at a mean age of 22 years (SD=9), and had a mean duration of alcoholism of 24 years (SD=6). The mean liver function test values (IU/liter) for the alcohol-dependent patients were as follows: SGOT, 38 (SD=25); SGPT, 45 (SD=42); and γ-glutamyltransferase, 88 (SD=42). The mean values for the healthy subjects were the following: SGOT, 24 (SD=5); SGPT, 28 (SD=6); and γ-glutamyltransferase, 39 (SD=10).
Patients with hepatic encephalopathy were recruited from the Yale New Haven Hospital Section of Gastroenterology. Their mean age was 40 years (SD=6). During the 12-hour fast before MRS testing, lactulose treatment for hepatic encephalopathy symptoms was withheld from four of the five patients. Blood was drawn for determination of ammonia levels within 1 hour of the MRS scan. The mean liver function test values (IU/liter) were as follows: SGOT, 73 (SD=15); SGPT, 79 (SD=12); and alkaline phosphatase, 202 (SD=20).
All subjects gave written informed consent for the study after an interview in which all procedures were fully explained to them. The protocol was approved by the Yale Human Investigations Committee and the Human Subjects Subcommittee of the VA Connecticut Healthcare System.
After MRS the Hopkins Verbal Learning Test
(8) was administered to assess the relationship of learning and memory to the total level of GABA plus homocarnosine in the occipital cortex within groups. The subjects were asked to repeat a list of 12 words immediately after presentation and 30 minutes later.
Localized
1H-MR spectra were acquired at 2.1 T from a 1.5× 3.0×3.0-cm
3 volume in the occipital lobe
(9). Metabolites were measured from short-TE spectra following subtraction of the macromolecule spectrum. The total level of GABA plus homocarnosine
(10) was measured by using homonuclear editing
(9). Each metabolite concentration was determined from signal intensities, expressed as the ratio of the metabolite to creatine
(9); the latter concentration was assumed to be 9 mmol/kg.
Analyses of variance (ANOVAs) were performed to compare the occipital cortex metabolite levels of the subject groups. Post hoc Duncan’s new multiple range tests were performed to adjust for multiple comparisons. The relationship between scores on the Hopkins Verbal Learning Test for immediate and delayed recall and the occipital cortex concentration of GABA plus homocarnosine was determined within groups by using Spearman correlations adjusted for multiple comparisons with Bonferroni corrections. The hepatic encephalopathy patients were excluded from this analysis because data were available for only three patients.
RESULTS
Memory impairment appeared to be associated with an abnormal total level of GABA plus homocarnosine. For the alcohol-dependent patients, but not healthy subjects, there was a significant negative correlation (r=–0.96, p=0.02, N=5) between the occipital cortex GABA-homocarnosine level and the score for delayed, but not immediate, recall on the Hopkins Verbal Learning Test.
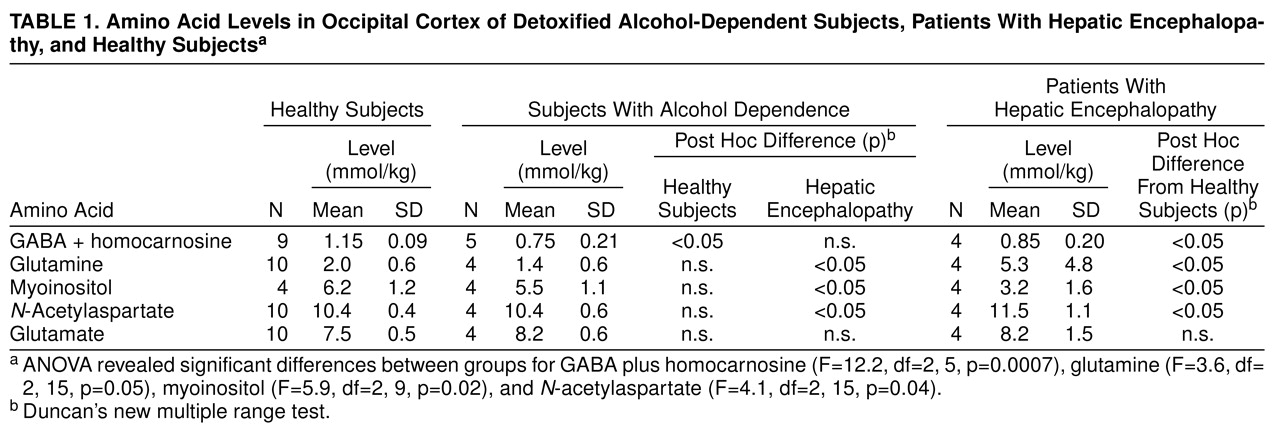
The total GABA-homocarnosine level was lower in the recently detoxified alcohol-dependent and hepatic encephalopathy patients than in the healthy subjects (
Table 1). Glutamine and
N-acetylaspartate levels were higher and myoinositol levels were lower in the patients with hepatic encephalopathy than in either the healthy subjects or the alcoholics. Venous blood ammonia levels were also higher in the hepatic encephalopathy patients (mean=70 µM, SD=26, N=4) than in the alcohol-dependent (33–42 µM, N=2) or healthy subjects (mean=34 µM, SD=2, N=4). No significant differences emerged in the analyses of glutamate, aspartate, choline (relative to brain creatine), or creatine (relative to brain water).