“Mr. J” is a 28-year-old single male financial services representative who self-referred because of problems with focus, distractibility, and completing tasks. He says his work performance is poor because of “inefficiency, poor organization, and carelessness.” He has difficulties with time management and procrastination and always works “right up to the deadlines.” He also reports having high levels of fidgetiness, internal restlessness, intrusiveness, talkativeness, and impulsivity. He denies frank depressive or manic symptoms but notes being “easily frustrated.” On interview, Mr. J reports that he started using marijuana “periodically” during his sophomore year in college, although for the past 3 years, except during a 1-month period of abstinence about 1 year ago, he has been smoking it almost every weekend and sometimes during the week. While he concedes that he may have a problem with marijuana, he maintains that he uses marijuana “to self-medicate, to relax . . . it really helps me slow my thoughts.” He admits that he occasionally drives after smoking marijuana. Mr. J suspects that he may feel “more frustration the next day after smoking,” although he states that he really does not want to quit. He reports that he drinks socially and experimented with cocaine, amphetamine, and Ecstasy in college. He also used a friend’s dextroamphetamine in college and found that it helped him concentrate, focus, and stay awake while completing large college projects. He denies smoking cigarettes. Mr. J could not remember how his academic performance was in elementary school but says he has long-standing problems with inattention, easy distractibility, daydreaming, and poor organization. In junior high school, he recalls, it took him longer than others to complete homework and examinations. He was told that he was smart, but he felt he was an underachiever in most subjects through school. Mr. J’s psychiatric history is unremarkable. His family psychiatric history is significant for a father who has never been diagnosed but is reportedly similar to the patient and gets frustrated easily. Mr. J’s sister is finishing high school and is doing well. The patient’s medical history is unremarkable, and he is not taking any medications. Mr. J’s girlfriend is concerned about his marijuana use and also has been encouraging him to seek evaluation for what she thinks is attention deficit hyperactivity disorder (ADHD). The patient is well groomed, forthcoming, and amicable. He is fidgety, appears slightly anxious, and frequently looks around the room. His speech is characterized by increased content but normal delivery. He notes having a “quick temper” but denies other mood symptoms or neurovegetative symptoms. He has no psychotic symptoms. During the interview he occasionally becomes distracted and loses track of what he was talking about, but he is redirected easily. Cognitively, he is of above-average intelligence, is alert and oriented, and has solid intermediate and long-term memory recall. He requires redirection to stay focused and notes having problems with remembering things he has just learned, such as names and directions. He has diminished focus and attention. His insight is good, and he clearly is interested in being diagnosed and treated. The results of the clinical interview and a structured psychiatric interview reveal current and past attention deficit hyperactivity disorder not otherwise specified (lacking full childhood-onset criteria) and marijuana abuse.
This case represents a typical scenario for an adult presenting for treatment for ADHD who also has a current substance use disorder, in this case marijuana abuse. The overlap between ADHD and alcohol or drug abuse or dependence in adolescents and adults has been an area of increasing clinical, research, and public health interest. ADHD generally has its onset in early childhood; 6%–9% of juveniles and 4%–5% of adults are affected. Symptoms persist from childhood into adulthood in approximately half of cases. ADHD is associated with learning disorders and psychiatric comorbidity as well as substantial educational, occupational, and interpersonal impairment throughout life (1) . Substance use disorders usually begin in adolescence or early adulthood and affect 15%–20% of U.S. adults, and a less defined but sizable number of juveniles (2) . The literature demonstrates a bidirectional overlap between ADHD and substance use disorders (3) .
Overlap Between ADHD and Substance Use Disorders
Studies of adults with substance use disorders show high rates of ADHD. Overall, 15%–25% of adults with drug and alcohol use disorders have current ADHD (3, 4) . In one study, 21% of cocaine-dependent adults had ADHD, although only 10% of those with ADHD had a history of clear childhood-onset symptoms (4) . Recent data suggest that adults who meet diagnostic criteria for current ADHD but for whom there is no clear evidence of some childhood symptoms (ADHD not otherwise specified) have characteristics similar to those with prototypic ADHD in terms of familiality of ADHD, psychiatric comorbidity, neuropsychological disturbances, and impairment (5) and may constitute a group with a viable subtype of ADHD. Among adolescents and adults with ADHD and comorbid drug use disorders, as typified in the case presented, marijuana is the most commonly misused agent (3) .
An overrepresentation of substance use disorders has also been found in studies of adults with ADHD: 17%–45% of adults with ADHD have alcohol abuse or dependence, and 9%–30% have drug abuse or dependence (3) . In a study of never-treated adults with ADHD (6), the risk of substance use disorders was found to be twice as high, and comorbid bipolar disorder or juvenile conduct disorder clearly increases the risk. ADHD itself appears to be a risk factor for later substance use disorders (6), with onset typically around 17–19 years of age (3) . Adults with ADHD plus a substance use disorder also have an elevated risk of other psychiatric disorders compared with those who have either diagnosis alone. High rates of ADHD have been reported in first-degree relatives with substance use disorders (3) . In adolescents and adults with ADHD, substance use problems are typically more substantial than in those without ADHD. Individuals with both diagnoses have been reported to have an earlier onset, a longer course, and greater severity, with more relapses and greater difficulty remaining abstinent (3) .
ADHD is associated with early initiation of cigarette smoking (before age 15), higher risk of cigarette use into adulthood, higher risk of substance use disorders, and a lower likelihood of quitting compared with age-matched subjects without ADHD (3, 7) . Given that nicotine has been shown to reduce ADHD symptoms (8), smoking cessation may be more difficult for adults with ADHD. Although treatment with stimulants has a protective effect on later cigarette smoking and substance use disorders for juveniles with ADHD, stimulants also may exacerbate smoking in current nicotine-dependent individuals (9) . The effect of methylphenidate treatment of adults with ADHD on smoking cessation is currently being investigated in a multisite study funded by the National Institute on Drug Abuse.
For a patient like the one in the case presented, would early treatment of his ADHD have diminished or increased his risk for later substance use disorders? Although some clinicians and others worry about the abuse liability and potential kindling effect of early exposure to stimulants in children with ADHD, preclinical and clinical data do not appear to support such concerns. Earlier treatment appears to be associated with a reduced risk of later tobacco and substance use (3, 10) . For example, a meta-analytic exploration of the role of early stimulant treatment in later substance use disorders found that pharmacotherapy did not increase the risk; on the contrary, the evidence indicated a protective effect against later substance use disorders (11) .
Neurobiological Relationships Between ADHD and Substance Use Disorders
The literature shows that first-degree relatives—siblings, parents, and offspring—of individuals with substance use disorders have a higher risk of ADHD; relatives of those with ADHD have a higher risk of substance use disorders; and relatives of those with ADHD plus a substance use disorder have a very high risk of both disorders compared with subjects who have neither disorder (3) . In the case presented, the patient had a father with ADHD traits. Family, twin, adoption, and molecular genetic studies show that genes have a role in the etiology of ADHD. The heritability of ADHD is about 70%, among the highest of psychiatric disorders (12) . Studies of children and adults have found evidence for the involvement of several genes in the etiology of ADHD that may be relevant to substance use disorders: the dopamine D 2 receptor gene, the dopamine β-hydroxylase gene, the dopamine transporter gene, the SNAP-25 gene, the dopamine D 4 receptor gene, and others (12, 13) . Both ADHD and substance use disorders may have a polygenic mechanism or represent variable expressivity of a shared risk factor (12, 13) .
Neuropsychological deficits remarkably similar to those observed in adults with substance use disorders have been consistently documented in studies of adults with ADHD (14) . These adults tend to have impaired performance on tasks assessing vigilance, motor speed, response inhibition, verbal learning, and working memory. Studies evaluating the relationship of neuropsychological dysfunction in ADHD to substance use disorders are under way.
The neuroimaging literature shows evidence of structural brain abnormalities in subjects with ADHD, including smaller volumes in frontal cortex, cerebellum, and subcortical structures (14) . Functional imaging studies implicate fronto-subcortical systems and deficits in anterior cingulate activation in the pathophysiology of ADHD. Three subcortical structures implicated by the imaging studies, the caudate, putamen, and globus pallidus, are part of the neural circuitry underlying motor control, executive function, inhibition of behavior, and the modulation of reward pathways—critical in substance use disorders (14 – 16) . These frontal-striatal-pallidal-thalamic circuits provide feedback to the cortex for the regulation of behavior. ADHD is thought to be mediated by catecholaminergic dysregulation of norepinephrine and dopamine, the latter of which has been implicated as a common pathway for substance use disorders (16) .
Evidence also exists that a subgroup of persons with ADHD may be self-medicating, like the patient described in the case. Adults with nicotine dependence often describe improved attention and executive function, which is consistent with the literature on nicotinic agents, and nicotinic agents have been used in the treatment of ADHD (8) . ADHD also may result in conduct symptoms and an eventual substance use disorder that is speculated to be related to demoralization and failure. Other evidence of self-medication includes preference of drugs over alcohol in both adolescents and adults with ADHD (6) and higher risk of cigarette smoking and substance use disorders in individuals with residual ADHD symptoms (10) . However, adults with ADHD have also been found to be indistinguishable from their peers without ADHD in the type of substance abused (6), with no differences evident between young adults with and without ADHD in indices of self-medication (such as mood and sleep). The specific substances individuals use do not appear to be correlated with any particular aspect of ADHD.
Assessment and Treatment Guidelines
Differential Diagnosis
Evaluation and treatment of comorbid ADHD and substance use disorders should be part of a plan in which careful attention is paid to the differential diagnosis, including medical and neurological conditions whose symptoms may overlap with ADHD (sleep difficulties, hyperthyroidism, and seizure disorder). Similarly, other psychiatric disorders may overlap with ADHD in this patient group, including dementia, substance-related organic mental disorder, bipolar disorder, and generalized anxiety disorder. Current ADHD symptoms also may be exacerbated by, or be a result of, substance use disorders such as chronic intoxication, protracted withdrawal, or neuropsychological disturbance secondary to chronic substance use disorder. It is prudent, as in the case presented, to ascertain the amount of substances currently being used, symptoms experienced while “drug free,” and symptoms associated with substance use.
The diagnosis of substance use disorder is predicated on a systematic review of the history and available objective evidence (e.g., treatment, urine toxicology screens, and consequences such as arrests). In general, the loss of control over one’s substance use should trigger concern about a substance use disorder. Briefly, DSM-IV-TR criteria for substance abuse include recurrent use despite consequences (disturbances in occupational, school, social, interpersonal, or legal domains) or in potentially hazardous situations. Substance dependence is heralded by abuse criteria plus more severe psychosocial impairment and distress despite use, inability to diminish or discontinue use despite attempts, and evidence of tolerance or withdrawal. In the case presented, the patient has marijuana abuse: a clear pattern of misuse with consequences, evidence of impairment, and use in potentially hazardous situations (driving).
Semistructured psychiatric interviews or validated rating scales for ADHD are invaluable aids in the systematic diagnostic assessment of ADHD and other psychiatric comorbid disorders in this patient group. The retrospective diagnosis of ADHD, as in the case presented, has been shown to be valid and reliable in the evaluation of ADHD (17) . Data derived from clinical trials of adults with ADHD indicate that self-report is better than collateral report for the presence of symptoms. ADHD symptoms in adults with substance use disorders appear to be developmentally related to those in children, including inattention in the majority, impulsivity, and hyperactivity. In addition, patients may have associated stubbornness, low frustration tolerance, and chronic conflicts in social relations with peers and authorities. Screening for ADHD in adolescents and adults with a substance use disorder, as in the case presented, can be undertaken with six-item and full 18-item DSM-based checklists for ADHD (17) .
Treatment
Referral to support groups for ADHD (e.g., www.chadd.org) or substance use disorders (e.g., www.alcoholics-anonymous.org) is recommended. The treatment needs of patients with ADHD and a substance use disorder should be integrated; however, if possible, it is best to address the substance use disorder initially (18) . If the substance use disorder is active, as in the case presented, attention needs to be paid to stabilization of the addiction(s). Treatment for ADHD (and, if applicable, comorbid psychiatric disorders) should be given in tandem with treatment for addiction (18) . Although the efficacy of various psychotherapeutic interventions for co-occurring ADHD and substance use disorder remain to be established, structured cognitive therapies appear to be useful in the treatment of both ADHD and substance use disorder. Therapeutics for substance use disorder and ADHD can be given in tandem with other treatment modalities for addiction, including pharmacotherapy.
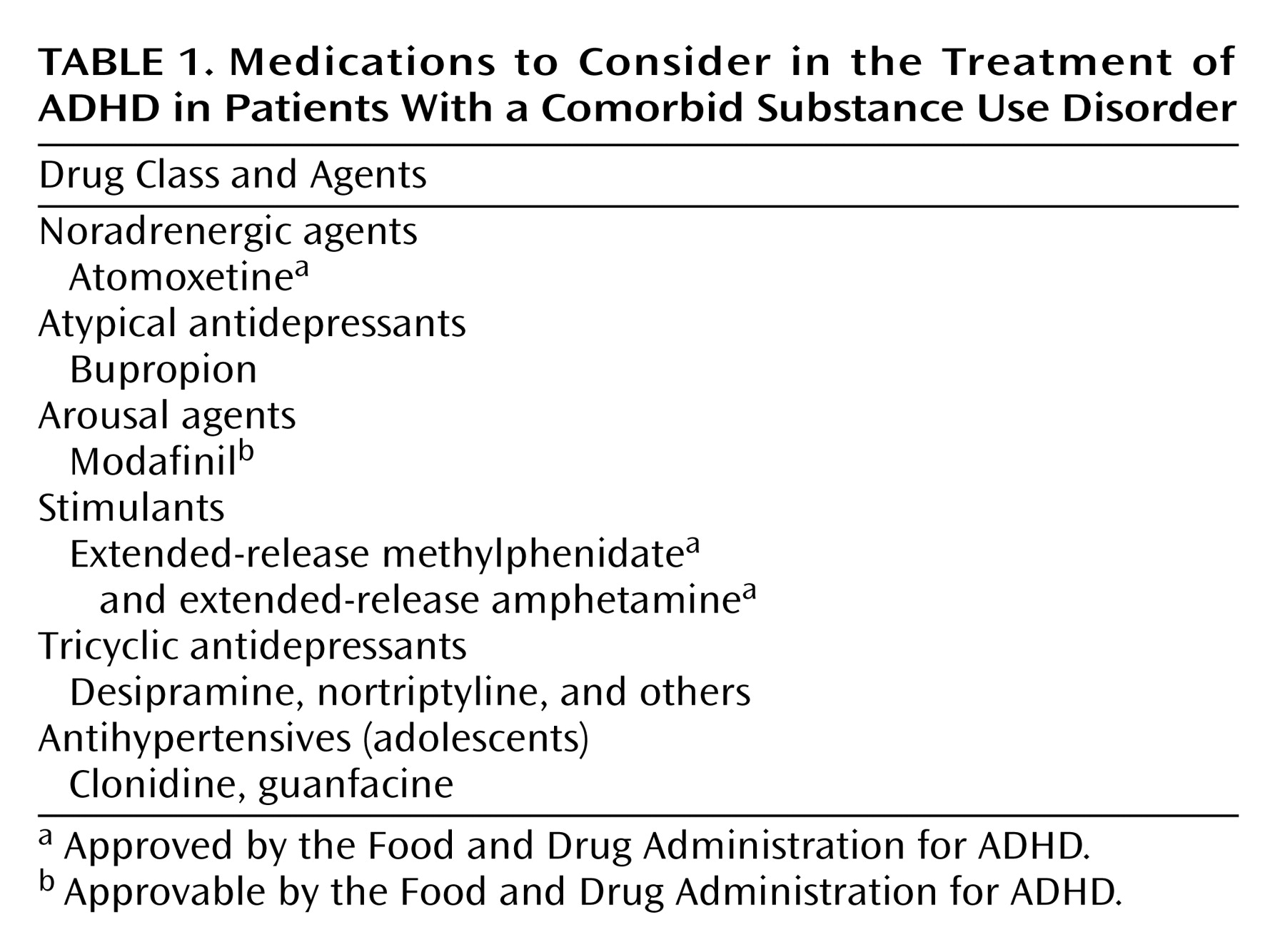
In our case, it seems prudent to consider medication for the patient’s ADHD to reduce the symptoms of the disorder. Effective agents for adults with ADHD include stimulants, noradrenergic agents, arousal agents, and catecholaminergic antidepressants (see Table 1 ). Aggregate findings from open and controlled trials suggest that in adults with ADHD and a current substance use disorder, ADHD medications marginally treat the ADHD but have little effect on substance use or cravings, and attrition rates are high. For example, in a large, prospective, double-blind, randomized trial of methylphenidate in cocaine-abusing subjects who had clinical evidence of ADHD (19), some reductions in ADHD symptoms but none in cocaine cravings or use were reported in the methylphenidate group.
There is no evidence that the specific substance of abuse predicts response or tolerability to ADHD medications. In any case, treating ADHD pharmacologically does not appear to exacerbate a substance use disorder. For instance, stimulants have been found not to increase subjective or objective measures of cocaine use or craving in ADHD or cocaine-substitution studies (20) . Studies evaluating the effectiveness of ADHD medications on recently abstinent individuals with ADHD are under way. Atomoxetine, bupropion, and extended-release stimulants are recommended for ADHD patients with very recent substance use disorder (i.e., within 3 months). Because of both lower effect sizes in ADHD and the potential for drug-drug interactions with substances of abuse (21), the alpha agonists and tricyclic antidepressants are often reserved as alternative agents for treatment of ADHD with a comorbid substance use disorder. Amphetamines should be avoided in patients with a history of amphetamine-related psychosis.
Volkow and colleagues conducted a series of studies that have helped to elucidate the mechanism of action of stimulants as well as why methylphenidate does not have the same abuse liability as cocaine. They found, for instance, that oral methylphenidate had slower uptake into the striatum, slower binding and dissociation from the dopamine transporters, and lower euphoric effects than cocaine (15) . Taking the next step, Spencer and colleagues recently reported that extended-release methylphenidate had less likeability and slower uptake and dissociation from the dopamine transporters than immediate-release methylphenidate (22) . These aggregate findings suggest a relatively low abuse liability for stimulants in adults with ADHD who do not have substance addiction; they also alleviate the concern that therapeutic oral doses of stimulants in patients with an active substance use disorder might worsen the addiction. Because stimulant diversion remains an issue in high school and college settings (23), particularly with the immediate-release stimulants, clinicians should discuss with patients the proper storage and administration of these agents.
Summary and Recommendations
In the case of Mr. J, a first step would be to have a frank and thorough discussion of the marijuana abuse, ADHD, and impairment overlap of the two disorders. Initial emphasis should be placed on self-directed abstinence or reduction in marijuana use. If this approach is unsuccessful, referral to a counselor with expertise in substance use disorders and ADHD employing cognitive behavior approaches is suggested. If the patient is able to abstain from or reduce marijuana use, medications to consider—after a urine toxicology screen to evaluate current use of marijuana and other substances and an evaluation for potential medical issues—would include atomoxetine, bupropion, or an extended-release stimulant. If Mr. J has a positive response to treatment but continues to manifest personal or professional difficulties, referral for adjunct cognitive behavior therapy is indicated. Ongoing monitoring during follow-up would include: effectiveness of the current treatment for ADHD, current marijuana (and other drug) use, presence of other psychiatric disorders (e.g., anxiety and mood disorders), and general balance in Mr. J’s life (e.g., diet, activity, and social life). Yearly evaluation of the need for ongoing pharmacotherapy is advised.
In summary, there is a strong literature supporting a relationship between ADHD and substance use disorders. ADHD is associated with higher rates of cigarette smoking and substance use disorders, often manifesting in late adolescence and young adulthood. The neuropsychological and neurobiological literature indicates important overlaps between ADHD and substance use disorders, and the two need to be treated in tandem.
Footnotes
Received May 18, 2006; revisions received Aug. 11 and Aug. 23, 2006; accepted Aug. 24, 2006. From the Clinical Research Program in Pediatric Psychopharmacology, Massachusetts General Hospital; and Harvard Medical School, Boston. Address correspondence and reprint requests to Dr. Wilens, Massachusetts General Hospital, Pediatric Psychopharmacology Unit, 32 Fruit St., YAW 6A, Boston, MA 02114; [email protected] (e-mail).Supported by NIDA grants K24-DA016264 and R01-DA14419.
CME Disclosure: Dr. Wilens has received research support from Abbott Laboratories, Ortho-McNeil, Eli Lilly, National Institute on Drug Abuse, Neurosearch, and Shire Laboratories. He is on speaker’s bureaus of Ortho-McNeil, Novartis Pharmaceuticals, and Shire Laboratories and has been a consultant for Abbott Laboratories, Ortho-McNeil, GlaxoSmithKline, Eli Lilly, National Institute on Drug Abuse, Novartis, Pfizer, and Shire Laboratories. APA policy requires disclosure by CME authors of unapproved or investigational use of products discussed in CME programs. Off-label use of medications by individual physicians is permitted and common. Decisions about off-label use can be guided by scientific literature and clinical experience.
Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE: Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry 2005; 62:593–602
Wilens TE: Attention-deficit/hyperactivity disorder and the substance use disorders: the nature of the relationship, subtypes at risk, and treatment issues. Psychiatr Clin North Am 2004; 27;283–301
Faraone SV: ADHD “Not Otherwise Specified”: conceptual issues, in 159th Annual Meeting of the American Psychiatric Association, Toronto, Canada, American Psychiatric Association, 2006, p 44
Biederman J, Wilens T, Mick E, Milberger S, Spencer TJ, Faraone SV: Psychoactive substance use disorders in adults with attention deficit hyperactivity disorder (ADHD): effects of ADHD and psychiatric comorbidity. Am J Psychiatry 1995; 152:1652–1658
Kollins SH, McClernon FJ, Fuemmeler BF: Association between smoking and attention-deficit/hyperactivity disorder symptoms in a population-based sample of young adults. Arch Gen Psychiatry 2005; 62:1142–1147
Conners CK, Levin ED, Sparrow E, Hinton SC, Erhardt D, Meck WH, Rose JE, March J: Nicotine and attention in adult attention deficit hyperactivity disorder (ADHD). Psychopharmacol Bull 1996; 32:67–73
Upadhyaya HP, Rose K, Wang W, O’Rourke K, Sullivan B, Daeas D, Brady K: Attention deficit hyperactivity disorder, medication treatment, and substance use patterns among adolescents and young adults. J Child Adolesc Psychopharmacol 2005; 15:799–809
Wilens TE, Faraone SV, Biederman J, Gunawardene S: Does stimulant therapy of attention-deficit/hyperactivity disorder beget later substance abuse? a meta-analytic review of the literature. Pediatrics 2003; 11:179–185
Faraone SV, Biederman J: Neurobiology of attention deficit hyperactivity disorder, in Neurobiology of Mental Illness, 2nd ed. Edited by Charney DS, Nestler EJ. New York, Oxford University Press, 2004
Seidman L, Doyle A, Fried R, Valera E, Crum K, Matthews L: Neuropsychological functioning in adults with attention-deficit/hyperactiity disorder. Psychiatr Clin North Am 2004; 27:261–282
Chambers RA, Taylor JR, Potenza MN: Developmental neurocircuitry of motivation in adolescence: a critical period of addiction vulnerability. Am J Psychiatry 2003; 160:1041–1052
Schubiner H, Saules KK, Arfken CL, Johanson CE, Schuster CR, Lockhart N, Edwards A, Donlin J, Pihlgren E: Double-blind placebo-controlled trial of methylphenidate in the treatment of adult ADHD patients with comorbid cocaine dependence. Exp Clin Psychopharmacol 2002; 10:286–294
Spencer TJ, Biederman J, Ciccone PE, Madras BK, Dougherty DD, Bonab AA, Livni E, Parasrampuria DA, Fischman AJ: PET study examining pharmacokinetics, detection and likeability, and dopamine transporter receptor occupancy of short- and long-acting oral methylphenidate. Am J Psychiatry 2006; 163:387–395
McCabe SE, Knight JR, Teter CJ, Wechsler H: Non-medical use of prescription stimulants among US college students: prevalence and correlates from a national survey. Addiction 2005; 99:96–106
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).
If the address matches an existing account you will receive an email with instructions to retrieve your username
Create a new account
Change Password
Password Changed Successfully
Your password has been changed
Login
Reset password
Can't sign in? Forgot your password?
Enter your email address below and we will send you the reset instructions
If the address matches an existing account you will receive an email with instructions to reset your password.
Change Password
Congrats!
Your Phone has been verified
×
As described within the American Psychiatric Association (APA)'s Privacy Policy and Terms of Use, this website utilizes cookies, including for the purpose of offering an optimal online experience and services tailored to your preferences. Please read the entire Privacy Policy and Terms of Use. By closing this message, browsing this website, continuing the navigation, or otherwise continuing to use the APA's websites, you confirm that you understand and accept the terms of the Privacy Policy and Terms of Use, including the utilization of cookies.