Chronic psychosocial stressors trigger increases in the levels of glucocorticoid stress hormones that, in turn, have deleterious effects on the structure and function of CNS structures, especially the hippocampus
(1,
2) . For example, in rodents, atrophy of neuronal dendrites within the cornu ammonis of the hippocampus
(3) and deficits in spatial memory
(4) develop after chronic behavioral stress or administration of the glucocorticoid hormone corticosterone. In human subjects with chronic depression, which is frequently associated with increased activity of the hypothalamic-pituitary-adrenal (HPA) axis
(5), decreases in the volume of the hippocampus have been correlated with the duration of illness
(6,
7) . The cellular mechanisms underlying the potentially neurotoxic effects of glucocorticoid hormones are under intense investigation
(5) . In animals, behavioral stressors and corticosterone administration increase excitatory amino acid release
(8,
9) as well as the expression of
N -methyl-
d -aspartate (NMDA) glutamate receptors
(10) . Thus, glucocorticoid-triggered increases in excitotoxicity have been proposed as one mechanism of glucocorticoid-induced neuronal injury
(5) . Also, because the hippocampus plays a central role in inhibiting the activity of the HPA axis
(11), hippocampal damage could produce a repetitive cycle of increasing HPA dysregulation and ongoing hippocampal injury
(1) .
Glucocorticoid-related neuronal injury has also been proposed as a mechanism by which the CNS might be affected by “healthy” aging
(1,
12) . Age-related increases in corticosterone levels were first reported in rodents more than 25 years ago
(13) and have been correlated with spatial memory deficits
(14) . More recently, correlations have been reported between increased plasma cortisol levels, memory impairments, and smaller hippocampal volumes in nondemented elderly subjects
(15,
16) . Such findings should be interpreted with caution, however, since a portion of these subjects could have preclinical forms of Alzheimer’s disease
(17) . Lupien et al.
(18) suggested that elderly subjects could be clustered into subgroups characterized by increases, decreases, and no change in plasma cortisol levels over time. Again, a possible explanation for such findings is that the subjects in such subgroups may differ with regard to the frequency of preclinical forms of Alzheimer’s disease.
Increases in HPA axis activity have also been directly associated with Alzheimer’s disease. Increases in plasma cortisol levels have been reported in individuals with probable Alzheimer’s disease
(19,
20 –
23) but have been generally interpreted as evidence that the disease process of Alzheimer’s disease (i.e., Alzheimer’s-induced hippocampal degeneration) leads to disinhibition of the HPA axis. In line with this hypothesis, correlations have been reported between increases in HPA axis activity and dementia severity
(24) or hippocampal volume loss
(25,
26) in individuals with probable Alzheimer’s disease. Finally, decreases in cortical concentrations of corticotropin-releasing hormone (CRH) and increases in CRH receptors have been reported in postmortem studies of subjects with Alzheimer’s disease
(27,
28) . However, as with the correlations between plasma cortisol and hippocampal volumes, these findings have been interpreted as evidence of the effect of the Alzheimer’s disease process on CRH expression.
The purpose of this study was to assess the relationship between plasma cortisol levels and clinical and cognitive measures of the rate of disease progression in subjects with very mild or mild dementia of the Alzheimer type. Our hypothesis was that higher levels of HPA axis activity, as reflected by higher plasma cortisol levels, would be correlated with more rapid progression of clinical and cognitive deficits in subjects with Alzheimer-type dementia. Among cognitive measures, we were most interested in the relationship between cortisol levels and measures of memory performance, because of previous reports linking increased HPA axis activity to hippocampal volume loss and dysfunction in elderly persons
(5) . We also studied nondemented subjects age- and gender-matched to the demented subjects so that any normative relationships between cortisol levels and cognition could be assessed.
Method
The study subjects, all of whom lived in the community, enrolled in longitudinal studies of aging and dementia at the Alzheimer’s Disease Research Center (ADRC) at Washington University School of Medicine in St. Louis. Written informed consent was obtained from each participant after the nature and risks of the study were explained. Each participant was assessed annually with a standard protocol
(29) that included semistructured interviews with the participant and a collateral source (generally a spouse or an adult child) who was knowledgeable about the subject. The Clinical Dementia Rating scale was used as the primary method of recording the presence and severity of dementia
(30) . This instrument rates the presence or absence of cognitive impairment on a 5-point scale (0, 0.5, 1, 2, or 3, indicating no impairment to severe impairment) in six domains or “boxes”: memory; orientation; judgment and problem solving; function in the community; function at home and hobbies; and personal care. An overall score is then derived from the individual ratings in the six domains according to standard scoring rules
(30), such that a score of 0 indicates no dementia and scores of 0.5, 1, 2, and 3 indicate very mild, mild, moderate, and severe dementia, respectively. Also, the individual box scores can be totaled to yield a sum-of-boxes total score
(29) that ranges from 0 (no impairment in any domain) to 18 (maximal impairment in all domains). Interrater reliability for the Clinical Dementia Rating scale is high
(31,
32) . At our center, individuals with a score of 0.5 progress in a predictable manner to stages of more severe dementia, and at autopsy the large majority of such individuals have neuropathological Alzheimer’s disease
(33) . Individuals with similar impairment have been considered by other investigators to have mild cognitive impairment
(34) .
The subjects recruited for this study had Clinical Dementia Rating scores of 1 (mild dementia), 0.5 (very mild dementia), or 0 (no dementia) at the time of their assessment. To measure the rate of change of dementia severity in conjunction with the date of plasma sampling in each subject, all available annual Clinical Dementia Rating assessments were used from a period up to 2 years before and 2 years after the date of plasma sampling. The average number of assessments available in the subject groups was similar; for subjects with a score of 1, the mean number was 3.2 (SD=0.4), for those with a score of 0.5, the mean was 3.2 (SD=0.7), and for those with a score of 0, the mean was 2.7 (SD=0.8). Clinical Dementia Rating sum-of-boxes total scores were used as the clinical measure of dementia severity. Also, because of suggested links between hypercortisolemia and depression in the elderly
(5), symptoms of depression were assessed with the Geriatric Depression Scale at the time of the annual assessments
(35) .
To measure the rate of change in cognitive function, the subjects’ performance was assessed with a comprehensive neuropsychological battery administered in conjunction with the annual assessments but independently of the protocol that yielded the Clinical Dementia Rating scale. Clinicians were unaware of the results of the neuropsychological test battery, and the psychometricians were unaware of the results of the Clinical Dementia Rating evaluation. The neuropsychological battery included measures of episodic memory, semantic memory, speeded psychomotor performance, visuospatial ability, and attention
(36) . In a previous study
(37) in which this battery was used to describe the pattern of cognitive deficits in 407 individuals with very mild and mild Alzheimer-type dementia (Clinical Dementia Rating scores of 0.5 and 1), a factor analysis revealed three factors that accounted for about 70% of the variance in cognitive performance. In a subset of these subjects who were later examined at autopsy (N=41), scores for the three factors were correlated with the frequency of β-amyloid plaques in three general regions of the brain (temporal lobe, parietal lobe, and frontal lobe). Hence, the three factor scores were named according to these brain regions: temporal factor, parietal factor, and frontal factor, respectively. In the present study, these three factor scores were calculated for each subject using weightings derived from the prior factor analyses on the subjects with very mild and mild Alzheimer-type dementia
(37) .
Apolipoprotein E (apoE) gene allele status was also determined in all subjects; three (5.6%) subjects had two apoE4 alleles, 18 (33.3%) had one apoE4 allele, and 33 (61.1%) had no apoE4 alleles.
Cortisol levels were determined from plasma samples collected in conjunction with a study of CSF biomarkers of Alzheimer’s disease conducted by two of the authors (A.M.F. and D.M.H.). Samples were collected by venipuncture between 7:45 a.m. and 8:00 a.m. onto ice after an overnight fast; plasma was prepared and then stored at –80°C until the time of assay. Cortisol concentrations were assayed in duplicate using a commercially available double-antibody radioimmunoassay (Clinical Assays, DiaSorin, Stillwater, Minn.). Mean values were used for all analyses. The interassay coefficient of variation of this assay is less than 15% at cortisol concentrations between 3 and 40 μg/ml, and the limit of detection is 1 μg/ml.
Statistical analyses to test for an association between the rate of change of sum-of-boxes total scores and neuropsychological battery factor scores and plasma cortisol concentrations were performed using general linear mixed models. Random coefficients models were constructed
(38), which assumed a linear growth over time for each subject in Clinical Dementia Rating total scores and the three neuropsychological battery factor scores; the models also assumed an unstructured covariance matrix between the intercept and the slope across subjects within the three dementia severity groups. We assumed that the slope over time was a linear function of cortisol levels, allowing us to assess the association between the longitudinal rate of change of the sum-of-boxes total scores and neuropsychological battery factor scores and plasma cortisol levels. This assumption was justified because no higher-order term provided a significant effect in any of the models used in the analyses. In all t or F values from these models, Satterthwaite’s approximation was used to adjust the degrees of freedom for the denominator
(39) . The SAS PROC MIXED function
(40) was used to implement all these models.
Results
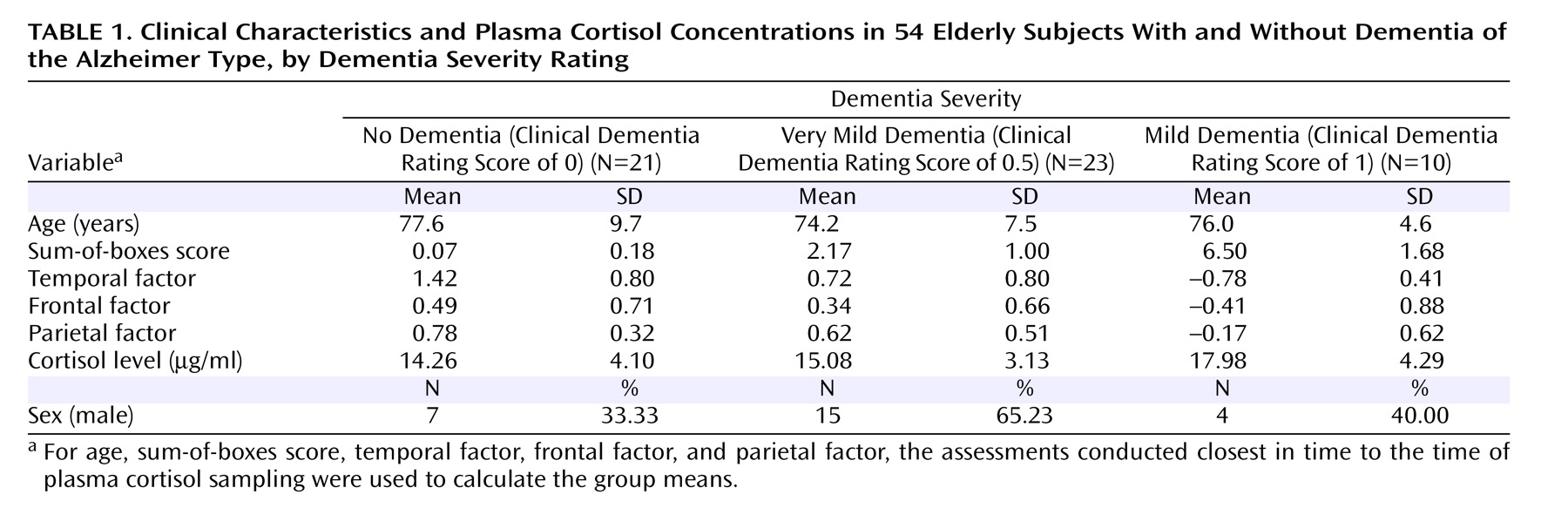
The clinical characteristics, sum-of-boxes scores, neuropsychological battery factor scores, and plasma cortisol levels for the three dementia severity groups are summarized in
Table 1 . One-way analysis of variance suggested a nonsignificant trend toward a group effect for plasma cortisol levels (F=2.3, df=2, 51, p=0.092); post hoc comparisons (least squared means) of the mean plasma cortisol levels across groups suggested that subjects with a score of 1 had slightly higher plasma cortisol levels than those with scores of 0 (p=0.013) and 0.5 (p=0.046) and also that these latter groups had similar plasma cortisol levels.
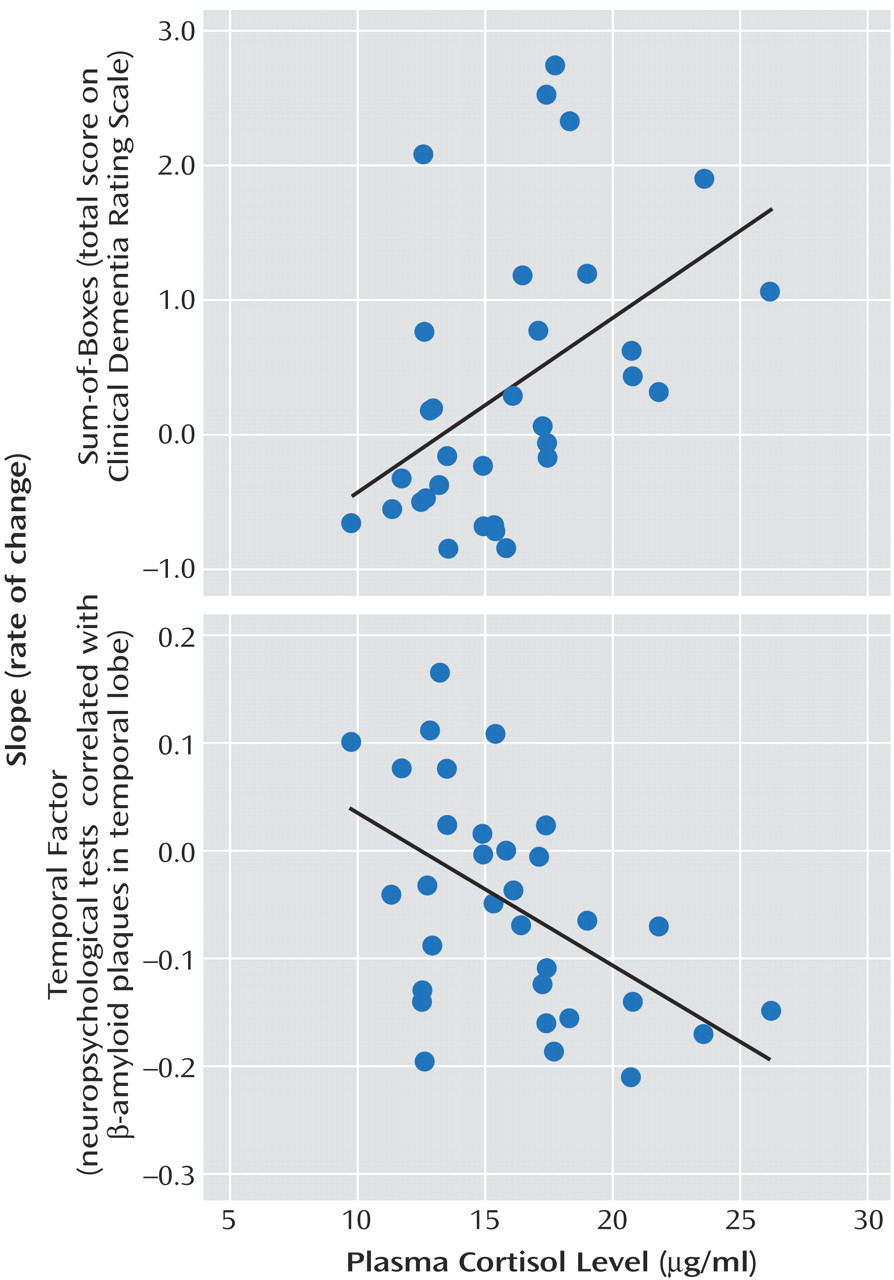
When the two groups with dementia were combined (N=33), a significant positive association was observed between plasma cortisol level and the rate of increase in sum-of-boxes scores (indicating worsening of symptoms) (t=2.86, df=40, p=0.007). There was also a significant negative association between plasma cortisol level and the rate of decrease in temporal factor scores (again indicating worsening of symptoms) (t=–2.59, df=33, p=0.014) but no association with the rates of change in parietal or frontal factor scores (see
Figure 1 ).
The magnitude of these associations was substantial: for an increase of 1 μg/ml in plasma cortisol, the annual rate of change in sum-of-boxes scores increased by 0.150 (SE=0.052), or 19% of the observed rate of change in sum-of-boxes scores (0.80 [SE=0.190]), and the annual rate of change in temporal factor scores decreased by 0.025 (SE=0.010), or 16% of the observed rate of change in temporal factor scores (–0.16 [SE=0.040]). In contrast, there were no significant associations between plasma cortisol levels and sum-of-boxes scores or temporal factor scores obtained from the assessment closest in time to the collection of the cortisol sample in the combined group of subjects with dementia.
When the subjects with very mild dementia (N=23) were evaluated separately, significant associations were observed between plasma cortisol levels and the rates of change in sum-of-boxes scores (t=2.53, df=31, p=0.017) and temporal factor scores (t=–2.58, df=26, p=0.016) but not parietal factor scores or frontal factor scores. However, when the subjects with mild dementia (N=10) were evaluated separately, there were no significant associations between plasma cortisol levels and the rates of change in sum-of-boxes scores, temporal factor scores, parietal factor scores, or frontal factor scores.
In the nondemented subjects (N=21), there were no significant associations between plasma cortisol levels and the rates of change in sum-of-boxes scores, temporal factor scores, parietal factor scores, or frontal factor scores.
When apoE allelic status was taken into consideration, the positive association between plasma cortisol levels and the rate of change in sum-of-boxes scores in demented subjects with no apoE4 alleles remained significant (t=2.76, df=41, p=0.009), but not in demented subjects with at least one apoE4 allele. The data also suggested a nonsignificant association between higher plasma cortisol levels and a more negative rate of change in temporal factor scores in demented subjects with at least one apoE4 allele (t=–1.94, df=25, p=0.063), but not in demented subjects with no apoE4 alleles. There were no significant associations between plasma cortisol levels and sum-of-boxes scores or temporal factor scores in nondemented subjects regardless of their apoE status.
There was no significant difference between groups in mean scores on the Geriatric Depression Scale obtained from the assessment closest in time to the collection of the plasma cortisol sample. There was also no significant correlation, for any group, between plasma cortisol levels and Geriatric Depression Scale scores obtained during the assessment closest in time to the collection of the cortisol sample.
Discussion
These results provide preliminary support for our hypothesis that increased glucocorticoid hormone levels, as reflected by morning plasma cortisol concentrations, are associated with the rate of change of both clinical and cognitive measures of dementia severity in subjects with Alzheimer-type dementia. It is especially intriguing that plasma cortisol levels were associated with the rate of change in the neuropsychological factor measure weighted toward memory function and previously found to be associated with neuropathological burden in the temporal lobe from Alzheimer’s disease (i.e., temporal factor scores)
(37) . This association is consistent with previous reports of relationships between increased HPA axis activity and age-related hippocampal volume loss
(5) . There have been conflicting reports about the density of glucocorticoid receptor expression in the hippocampus relative to other regions of the primate brain
(41 –
43) . Nonetheless, our findings raise the possibility that increased glucocorticoid levels have a disproportionate impact on the Alzheimer’s disease process as it develops in the hippocampus and other structures of the medial temporal lobe (e.g., the entorhinal cortex)
(44) .
The fact that no significant associations were observed between plasma cortisol levels and measures of dementia severity at the time of blood sampling suggests that increased cortisol levels were associated with more rapid rates of disease progression rather than the severity of disease. Taking this interpretation one step further, these results suggest that increased HPA axis activity as reflected by plasma cortisol levels may be associated with an acceleration of the Alzheimer’s disease process, rather than being the product of the degenerative effects of the disease on the hippocampus and HPA disinhibition.
We were surprised to find no associations between plasma cortisol and the rates of change in sum-of-boxes or neuropsychological factor scores in the elderly nondemented subjects. This finding is in apparent conflict with an earlier report of a correlation between plasma cortisol levels and the severity of cognitive impairment in nondemented elderly volunteers
(16) . One explanation for this discrepancy might be that the age range was too limited in our small group of subjects without dementia. Also, our subjects with a score of 0 on the Clinical Dementia Rating scale were rigorously screened to exclude even very mild signs of dementia. At this writing, only three (5.6%) of these individuals have been examined at autopsy, so it is not possible to determine the frequency of preclinical Alzheimer’s disease in our nondemented subjects. We also did not find any association between the severity of depressive symptoms and plasma cortisol levels in any of the subject groups. However, potential subjects who met syndromal criteria for depression were excluded from our study.
Our findings of a relationship between plasma cortisol levels and markers of disease progression in subjects with Alzheimer-type dementia may be particularly applicable to the early stages of Alzheimer’s disease. Significant correlations were observed between plasma cortisol concentrations and measures of disease progression in subjects with very mild dementia (score of 0.5 on the Clinical Dementia Rating scale) but not in those with mild dementia (score of 1). While the correlations between plasma cortisol levels and markers of disease progression would have been more difficult to evaluate in the small group of subjects with mild dementia, the values of the correlations observed in this group were not even suggestive of a trend.
At present, the mechanism by which increased HPA axis activity could accelerate the Alzheimer’s disease process is unknown. Behavioral stressors and administration of glucocorticoid hormones have been reported to increase excitatory amino acid release
(8,
9) and the expression of NMDA glutamate receptors
(10) in rodents. Using mice that overexpress the human form of amyloid precursor protein, we recently observed that chronic stress (in the form of isolation) accelerated the deposition of amyloid plaques as well as the appearance of deficits in learning and memory that usually accompany β-amyloid deposition
(45) . Also, Harris-White and Chu
(46) reported that glucocorticoid hormones may decrease the clearance of Aβ, which itself can have neurotoxic effects
(47) . Alternatively, behavioral stressors could influence cognition by decreasing hippocampal neurogenesis
(48) . Thus, stress-related increases in glucocorticoid levels could either directly or indirectly influence neuronal dysfunction and cognitive impairment associated with Aβ deposition.
There are some notable weaknesses in this study. First, our measure of the subjects’ stress responsivity was plasma cortisol levels at one time point on a single day. Our study was retrospective, and the only available plasma samples were collected in coordination with a study of CSF biomarkers for Alzheimer’s disease, which involved obtaining blood and CSF on a single day. However, a correlation has been previously reported between 8 a.m. cortisol levels and dementia severity in subjects with Alzheimer-type dementia
(24) . Also, our subjects may have had anticipatory anxiety on that day related to the lumbar puncture. Nonetheless, the associations observed between our simple measure of HPA axis activity and the rates of clinical and neuropsychological decline were substantial. Second, the samples available for this study, and especially the sample of mildly demented subjects, were small. Larger numbers of subjects with a wider range of dementia severity would have made it possible to more clearly determine whether the relationship between plasma cortisol concentrations and the rate of disease progression were specific to a particular stage of Alzheimer’s disease.
The results of this study need to be confirmed and extended by examining other measures of disease progression in larger numbers of subjects with Alzheimer-type dementia with wider ranges of dementia severity that has been assessed over longer periods. Studies of neuroanatomical markers of disease progression, such as measures of the structure of the hippocampus itself
(49,
50), would be particularly useful. If the hypothesis that stress can increase glucocorticoid levels and accelerate the progression of Alzheimer’s disease is confirmed, it would give impetus to the development of therapeutic approaches, both pharmacological
(51,
52) and nonpharmacological
(53), to decrease stress and levels of stress-related glucocorticoid hormones.