Studies following the events of Sept. 11, 2001, have shown posttraumatic stress disorder (PTSD) symptoms and widespread anxiety among directly and indirectly exposed civilians
(1 –
5) . These studies have also shown more severe reactions among those residing near the sites of the attacks (a proximity effect) and progressive decline of symptoms with time (a time effect
[6] ). The clinical and public health implications of reporting early PTSD symptoms have been questioned
(5) .
Studies of the psychological effects of Sept. 11, however, may have limited relevance to living under continuous terror. Whereas the Sept. 11 studies evaluated the aftermath of a discrete occurrence, after which recuperation could follow undisturbed by further attacks, continuous terror may evoke other reactions. For example, scattered attacks may defy the proximity effect in that they may seem to occur everywhere. Repeated attacks may also challenge the time effect by interfering with recuperation. In addition, a degree of adjustment might be seen as people develop effective ways of coping
(7) . Terrorism, and the efforts to contain it, can also disrupt people’s daily living (e.g., by affecting transportation and other forms of freedom) and thereby create a secondary stressor of unknown effects
(8) .
It is important to note that under continuous threat, the symptoms that are currently subsumed as posttraumatic and therefore purposeless and somewhat exaggerated (e.g., avoiding previously dangerous places and situations, responding emotionally to threat signals, remaining vigilant and “on guard”) may reflect anticipation and self-protection. This possibility predicts that there would be a gap between reporting such “symptoms” and being outstandingly distressed or dysfunctional.
Finally, terrorism may elicit excessive distress in a subgroup of vulnerable individuals (e.g., those with previous traumatic experiences, those with lesser resources) and thereby underscore a disparity between those severely affected and others who are more resilient. This possibility predicts that the distribution of PTSD symptoms within affected communities will not be homogeneous.
From October 2000 on, Israel has faced a lengthy wave of terror. There have been 132 suicide bomber attacks between October 2000 and April 2004, causing 666 deaths and 4,447 injuries among Israeli civilians and 276 deaths and 1,843 injuries among the security forces (i.e., 0.11% of the Israeli population of 6,667,000)
(9,
10) . Indirect exposure was also prevalent: 45% of Israelis reported having had “some exposure” to terrorism, and 60% felt that their life was in danger
(11) .
This work evaluates the effect of continuous terror by looking at the prevalence of PTSD, PTSD symptoms, and symptoms of general distress in two differentially exposed suburbs of Jerusalem. Data collection took place 10 months into this wave of violence. The study assessed the contributions of direct exposure and that of the disruption of daily living to symptom severity. It explored the distribution of PTSD symptoms within affected communities and the association between expressing PTSD symptoms and reporting outstanding distress and impairment.
Results
Participants and Background Characteristics
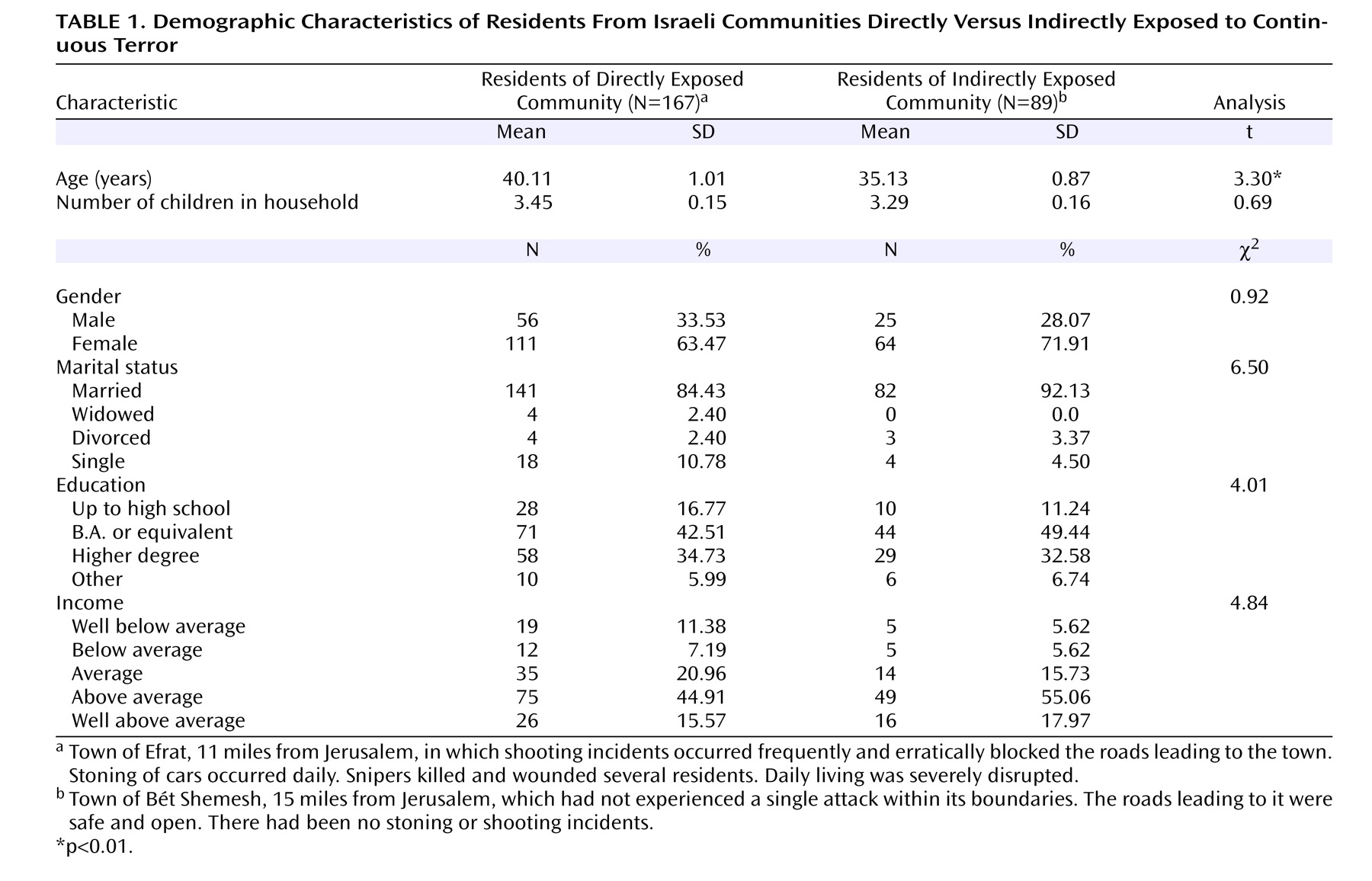
We approached 362 residents of the two communities, and 277 (76.5%) agreed to participate in the study. Subjects who declined did not differ from those who participated in gender rates. Refusal rates were similar in both communities. Comparisons between the current study group’s age, education, and number of children in the household and those reported for the same communities in Israel’s Central Bureau of Statistics’ Population Census
(10) were performed. According to the National Census, the mean age of residents in Efrat was 38.9 years and in Bét Shemesh was 41.4. In this study, the respective mean ages were 40.1 and 35.1 years. The mean number of children in a household was between 3.7 and 3.8 according to the National Census; in this study it was between 3.3 and 3.4. Education levels (data available for the directly exposed group alone) were as follows: 37.2% with college degree (B.A. or equivalent) and 39.6% with full academic degree (CM.A. or equivalent) (National Census figures) and, respectively, 42.6% and 34.6% (current study).
One subject withdrew his participation, and 20 had incomplete data. The study’s final sample was N=256: 167 from the directly exposed community and 89 from the indirectly exposed community. The two groups were similar in terms of gender composition, marital status, education, and average income but differed in age (
Table 1 ).
Frequency and Intensity of Exposure
As expected, residents of the directly exposed community were more frequently exposed to terror-related incidents (mean=6.58 incidents per resident [SD=3.96, SE=0.31]) than were those in the indirectly exposed community (mean=2.41 [SD=3.20, SE=0.34]) (t=8.94, df=254, p<0.001).
Men and women reported similar frequencies of exposure (men: mean=5.69 episodes [SD=4.56, SE=0.51], women: mean=4.87 [SD=4.02, SE=0.30]; t=1.41, df=254, p=0.20). Age-corrected ANOVA for exposure frequency showed a significant main effect of site (F=59.26, df=1, 254, p<0.0001) but a nonsignificant main effect of gender and a nonsignificant site-by-gender interaction.
The intensity of the immediate response to exposure was significantly higher in the directly exposed group (mean=1.61 [SD=0.73, SE=0.06]) relative to the indirectly exposed group (mean=1.30 [SD=0.82, SE=0.09]) (t=2.87, df=254, p<0.01). Immediate response intensity was also significantly higher in women (mean=1.65 [SD=0.75, SE=0.06]) relative to men (mean=1.27 [SD=0.76, SE=0.08]) (t=3.68, df=254, p<0.001). Age-corrected ANOVA for response intensity showed significant main effects of site (F=4.84, df=1, 253, p<0.02) and gender (F=7.42, p<0.01) but no site-by-gender interaction.
Disruption of Daily Living
With the exception of financial burden, daily life was significantly more disrupted in the directly exposed group (
Table 2 ). In both communities, women reported higher disruption of daily living. Age-corrected ANOVAs for total disruption score revealed significant main effects of site (F=73.38, df=1, 253, p<0.0001) and gender (F=3.9, 1, 253, p<0.05) but no significant site-by-gender interaction.
Prevalence of PTSD
Forty-five residents of the directly exposed community (26.95%) and 19 residents of the indirectly exposed community (21.35%) met Posttraumatic Symptom Scale criteria for PTSD, a nonsignificant difference. PTSD with significant distress was observed in 31 (18.56%) of the directly exposed residents and 15 (16.85%) of the indirectly exposed residents, also a nonsignificant difference. Last, PTSD with significant distress and functional impairment was seen in 16 (9.58%) of the directly exposed residents and six (6.74%) of the indirectly exposed residents, a nonsignificant difference.
Women and men had equal rates of PTSD according to both Posttraumatic Symptom Scale criteria (N=45 or 25.71% of all women and N=19 or 23.46% of all men) and by PTSD symptom criteria with distress and dysfunction (N=13 or 7.43% of women and N=9 or 11.11% of all men). Individuals with and without PTSD had similar age, marital status, income, and education.
Symptoms Expressed
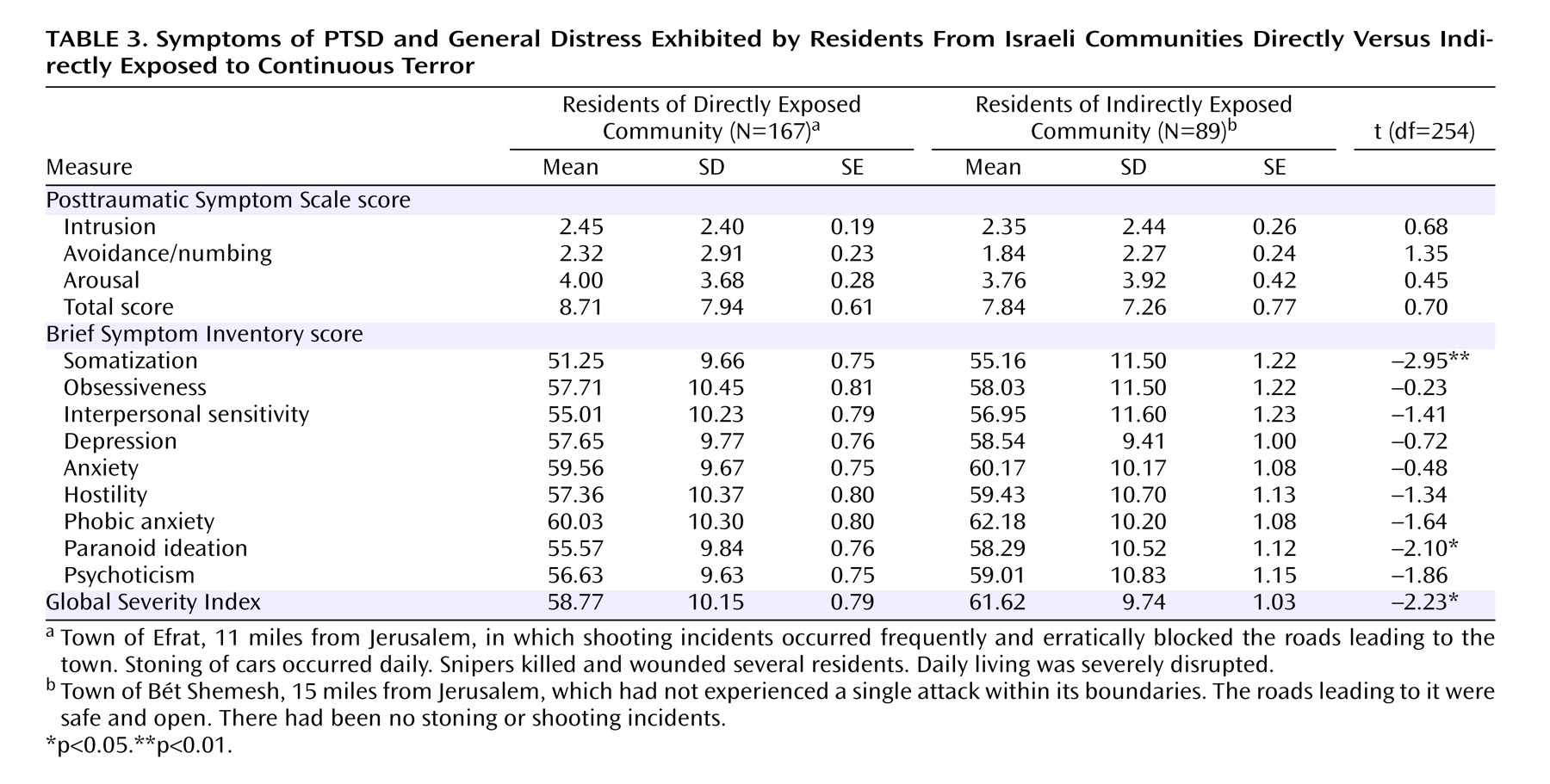
The two groups had comparable levels of PTSD symptoms and Brief Symptom Inventory scores (
Table 3 ). Somatization and paranoid ideation were somewhat higher in the indirectly exposed group, but the difference was not significant when corrected for multiple comparisons. The Global Severity Index was also higher in the indirectly exposed group.
Relative to men, women tended to endorse significantly more reexperiencing symptoms (mean=2.74 [SD=2.63, SE=0.20] versus 1.58 [SD=1.61, SE=0.18]) (t=3.68, df=254, p<0.001) and more hyperarousal symptoms (mean=4.22 [SD=3.87, SE=0.29] versus 3.25 [SD=3.42, SE=0.38]) (t=1.92, df=254, p=0.053) as well as somewhat higher, but not significantly different, avoidance symptoms (mean=2.28 [SD=4.74, SE=0.36] versus 1.89 [SD=2.74, SE=0.30]) (t=1.07, df=254, p<0.30). There was no interaction between gender and community for PTSD symptoms. ANOVA for Posttraumatic Symptom Scale total score showed a significant main effect of gender (F=5.43, df=1, 252, p<0.05) but no significant main effect of site or site-by-gender interaction.
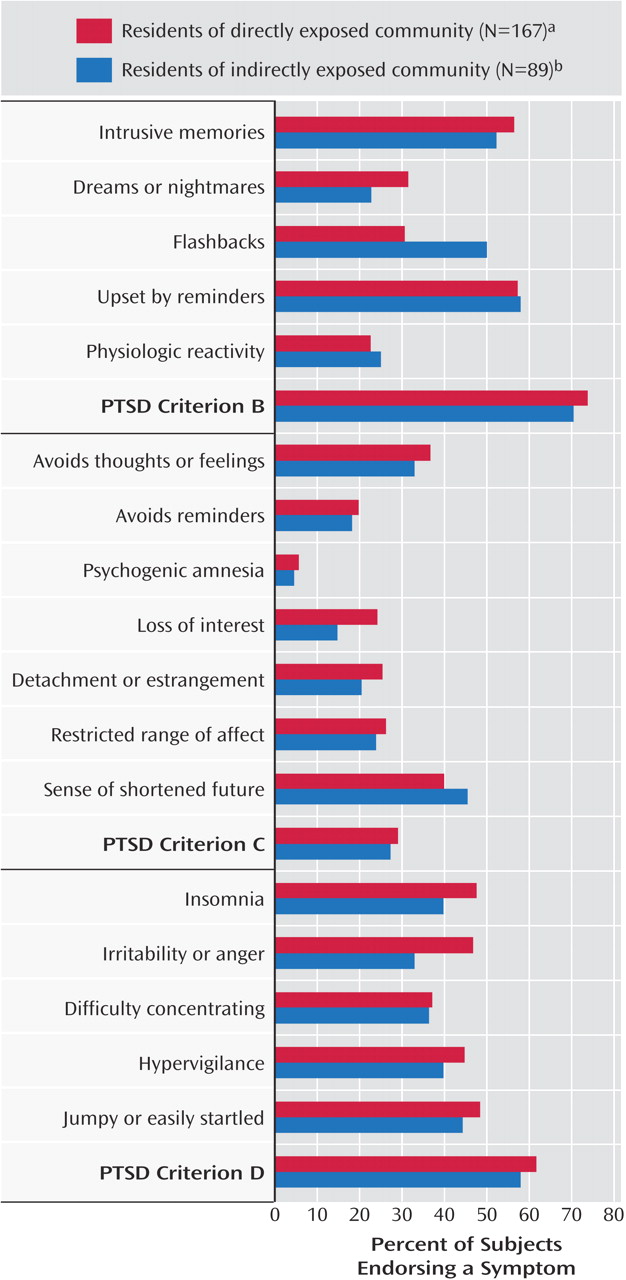
In order to further illustrate the similarity in PTSD symptom expression between the two communities,
Figure 1 displays the prevalence of each of the 17 DSM-IV PTSD symptom criteria for both sites. As can be seen, most PTSD symptoms were equally reported. Eighty-seven percent of the participants reported at least one PTSD symptom. Intrusive thoughts/recollections and being upset by reminders were the most frequently reported symptoms. Avoidance (DSM-IV criterion C) was less frequently reported than reexperiencing (criterion B) or hyperarousal (Criterion D).
Distribution of PTSD Symptoms
A goodness-of-fit test evaluated the distribution of Posttraumatic Symptom Scale scores in the study group. Posttraumatic Symptom Scale scores were not normally distributed (distribution χ 2 =64.5, df=20, p<0.0001; Kolmogorov-Smirnov d=0.14, p<0.01).
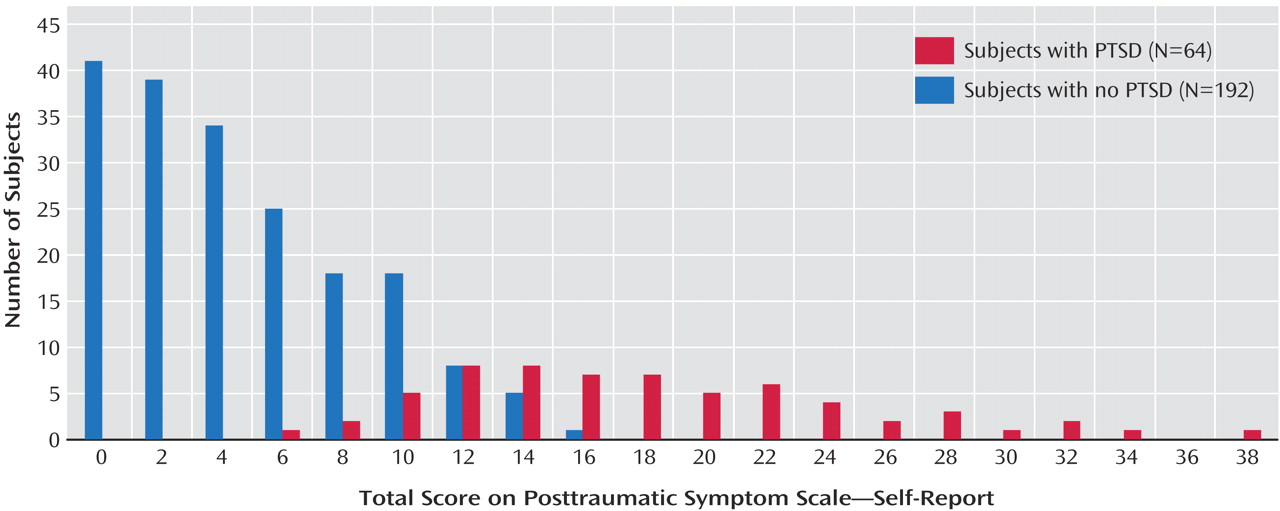
Comparison between subjects who met Posttraumatic Symptom Scale criteria for PTSD (N=64) and those who did not (N=192) revealed Posttraumatic Symptom Scale scores that were relatively high in the former (mean=18.68 [SD=6.95, SE=0.87]) and very low in the latter (mean=4.9 [SD=4.00, SE=0.29]) (t=19.20, df=254, p<0.0001).
Figure 2 illustrates the distribution of PTSD symptoms among subjects with and without PTSD.
Similarly, subjects who met symptom criteria for PTSD scored abnormally high on the Global Severity Index (mean=67.78 [SD=6.18, SE=0.77]), whereas the mean Global Severity Index of those without PTSD (mean=57.07 [SD=9.61, SE=0.69]) was within one standard deviation of the normal population score. The between-group difference was statistically significant (t=8.35, df=254, p<0.0001).
Contributors to PTSD and General Distress
Stepwise logistic regression assessed the contributions of exposure and disruption of routines (in that order) to Posttraumatic Symptom Scale-defined PTSD. In the directly exposed group, the analysis shows a significant contribution of exposure (odds ratio=1.29; maximum likelihood χ 2 =13.77, df=2, p=0.001), with an additional and significant contribution of disruption of routines (odds ratio=3.30; model χ 2 =36.64, df=3, p<0.00001; difference from previous fit: χ 2 =26.12, df=1, p<0.00001). In the indirectly exposed group, neither exposure nor disruption of routines predicted PTSD status (exposure: odds ratio=1.09 [χ 2 =2.58, df=2, p=0.28]; disruption of routines: odds ratio=1.06 [χ 2 =3.42, df=3, p=0.33]).
Stepwise regression analysis evaluated the relative contribution of exposure and disruption of routines to the Global Severity Index in each group. Disruption of routines, but not exposure, contributed to the Global Severity Index in both groups (directly exposed group: R 2 =0.21 [F=42.27, df=1, 164, p<0.0001]; indirectly exposed group: R 2 =0.08 [F=7.46, df=1, 88, p<0.01]).
Discussion
The results of this study show comparable PTSD prevalence and comparable levels of PTSD symptom intensity and general distress in two differentially exposed communities during a wave of terror. The results also show equal exposure of men and women to terrorist incidents and equal prevalence of PTSD in both genders. They additionally demonstrate an unequal distribution of PTSD symptoms, such that a subgroup of about 25% of the population was highly symptomatic, whereas others expressed low levels of symptoms. Many subjects met DSM-IV PTSD symptom criteria without simultaneously reporting significant distress and impairment. Disruption of daily living significantly contributed to PTSD symptoms and Brief Symptom Inventory scores.
In line with previous reports
(1 –
5), this study documented a frequent occurrence of PTSD symptoms in proximal and remote communities. Contrasting with previous research
(2,
3), however, a “proximity” effect was not found. This observation was consistent across symptoms (
Figure 1 ) and instruments (
Table 2 ). It replicates a previous finding
(11) of nonsignificant association between geographical proximity to sites of terrorist acts and PTSD symptoms among Israelis at about the same period.
A parsimonious explanation of this finding is that both communities were similarly affected by the stressfulness of living near Jerusalem—a prime target for terrorism, or living in a country besieged by terror. Terr et al.
(20) refer to this phenomenon as “distant-traumatic effects not connected to personal or direct threat.” The idea that the proximity to Jerusalem or an overall stressfulness of ongoing terror was sufficient to create equal responses in two differentially exposed communities raises the intriguing possibility of a ceiling effect, i.e., a saturation of responses by common threat factors. The idea of a “ceiling effect” should be further tested as a potential model for evaluating and predicting communities’ responses under duress.
The immediate and vivid way in which violent attacks are currently broadcasted and communicated may also account for the lack of difference between the communities. Accordingly, repeated exposure to unpredictable, shocking, and instantly communicated sights of terror defies the perception of safety, which geographic distance would normally confer.
Another way of interpreting this effect is a shift from probabilistic and exposure-driven, risk-assessment to indiscriminate contextual-driven fearfulness and an ensuing sense of imminent threat
(21) . Interventions designed to help people to better discern patterns of threat may, therefore, be called for in terror-prone areas.
Several symptoms were higher in the indirectly exposed group (
Table 3 ), and this requires further elaboration. Expressed symptoms reflect the summation of perceived threat on the one hand and perceived control and coping self-efficacy on the other
(22) . While this study did not measure these modulators of stress responses, it might be the case that being concretely challenged and having to actively cope with daily stressors contributes to a sense of controllability and self-efficacy. In that sense, the many ways in which residents of the directly exposed community had to concretely cope with terror threat could have contributed to better perception of controllability and self-efficacy, and thereby to a reduction in symptoms. A previous descriptive publication
(7) discussed the ways in which responding to the challenge of continuous terrorism in Jerusalem could be experienced as a sequence of small daily victories (e.g., effectively organizing one’s day, successfully driving to and from work) rather than defeats. One must also remember that the current study recorded “peritraumatic” reactions, i.e., those experienced during exposure. Psychological defenses may operate at such time and mitigate the open expression of emotions. The long-term consequences of higher exposure may be different.
The results of this study suggest that terror does not equally affect every community member. Although a minority appear to be highly susceptible to terror threat, most subjects had virtually no PTSD symptoms. The idea that only a subset of residents may require help may have important implications for planning of interventions. In addition, reporting PTSD was inconsistently associated with distress and impairment. A previous study of the 9/11 attacks
(2) used the Brief Symptom Inventory to independently evaluate the prevalence of “clinically significant psychological distress.” However, the prevalence of probable PTSD in that study was inferred from a cutoff score on a PTSD symptom scale. Our results suggest that combining PTSD symptoms, psychological distress, and functional impairment may effectively differentiate those whose defensive reactions of vigilance, worry, and caution become ineffective and who might need help.
This study is limited by the use of ad hoc measures of exposure and disruption of routines. In addition, the choice of two stable Israeli towns may not be representative of occurrences in which community resources and structures break down. However, this work identifies several clinically meaningful patterns of the response to continuous terror, such as the existence of a subgroup with very intense reactions. Furthermore, our understanding of what exposure represents should be modified in order to account for vectors of threat other than concrete exposure to acts of terror. Our results are in line with the conclusion of Silver et al.
(6) that “the psychological effects of a major national trauma are not limited to those who experience it directly, and the degree of response is not predicted simply by objective measures of exposure.” The complex interplay of the experience of danger, the disruption of daily routine, the coping behaviors, and the resulting symptoms of distress and disability provides a more nuanced picture of the dynamic impact of terror.