The count/cutoff approach was a tremendous improvement over DSM-II diagnosis. However, it had never previously been subjected to systematic testing against any other way of operationalizing diagnosis, particularly in clinical practice. Prototype diagnosis could be implemented with relatively minor taxonomic changes (by simply refining the prototypes tested here to match more closely the characteristics of patients with DSM-IV-defined personality disorders [
7,
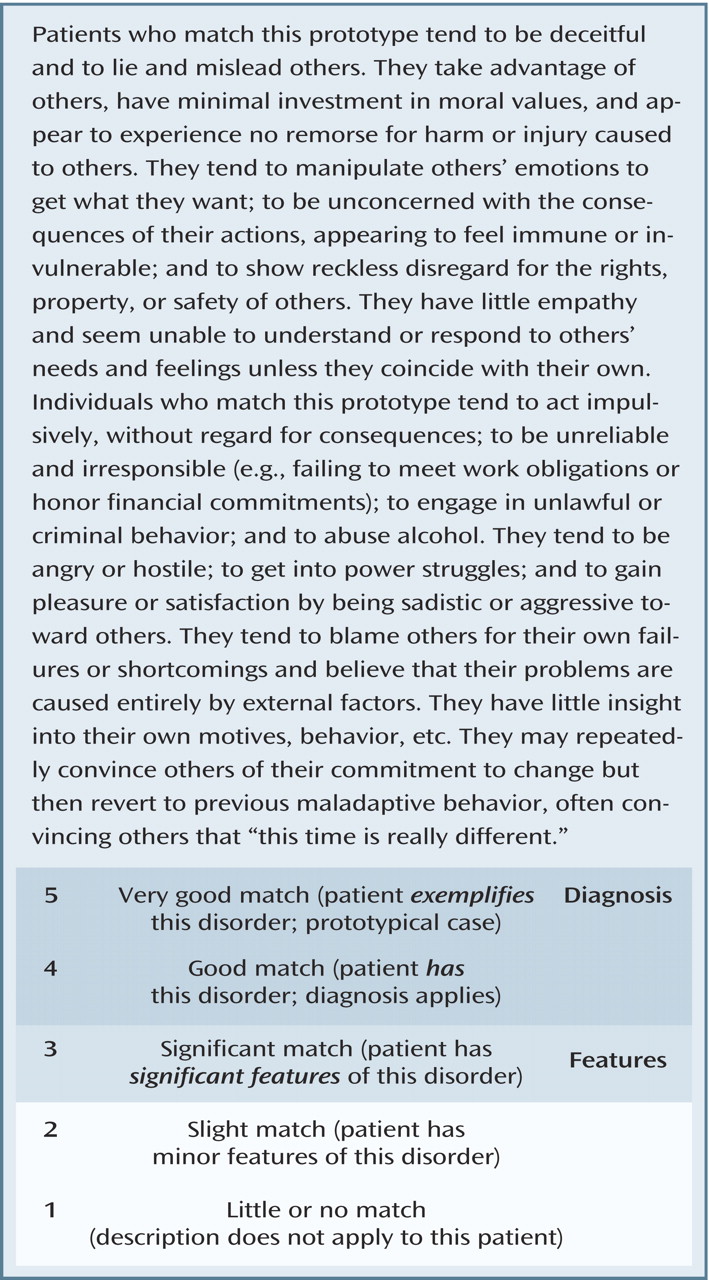
8 ]) or with more substantial changes (by deriving nonredundant diagnostic prototypes empirically). In either case, clinicians could make a complete axis II diagnosis in 1 or 2 minutes, generating a diagnostic profile (similar to an MMPI profile) that indicates, for each disorder, both the extent to which the patient resembles the prototype and whether the patient matches the prototype strongly enough to receive a categorical diagnosis useful for communication with other professionals. Prototype diagnosis has the parsimony of DSM-II diagnosis but lacks its disadvantages. For example, prototypes can be derived empirically, and, as noted earlier, they can be rated reliably.
A question we did not address here is whether prototype diagnosis is suitable only for clinical practice (similar to ICD-10, which has different diagnostic procedures for research and practice). Although single-item diagnostic ratings may not provide data that are reliable enough for research purposes (although see reference
26 ), one way of augmenting the method tested here is to obtain secondary ratings for patients who receive a score >1 for a given disorder. For example, for borderline personality disorder, this augmentation might entail 5-point ratings of subdimensions or endophenotypes (e.g. emotional dysregulation, impulsivity, and attachment dysregulation) that are generated by factor analysis. Such ratings could be aggregated along with the prototype ratings to maximize reliability or could be used as indicators of the latent construct in structural models. Alternatively, for research as well as clinical purposes, the prototypes could be rated along with a set of functional domains, such as motives and conflicts, cognition, emotional experience, emotion regulation, impulse regulation, relational functioning and representations, identity and self-experience, and adaptive strengths
(27,
28) . As we have shown elsewhere
(29,
30), researchers can obtain high interrater reliability and validity for prototype diagnosis of personality disorder by applying the SWAP-200 Q-sort to data from a systematic clinical interview and correlating patients’ profiles on the instrument with empirical prototypes; this procedure yields both a dimensional diagnosis and a functional assessment. We suspect that researchers could also derive prototype diagnoses from current axis II instruments, much as anxiety disorders researchers have derived dimensional ratings along with categorical diagnoses from structured interviews
(31) . An additional question is whether prototype diagnosis might be equally useful for axis I
(13) . We recently obtained similar findings with mood, anxiety, and eating disorders, but further research is clearly necessary.
Finally, these data raise the question of whether researchers may have too hastily invoked clinician error in explaining why clinicians tend not to use DSM-IV decision rules in assessing personality. Like all information processors, clinicians tend to elicit and organize the information they need to solve problems. Research in cognitive science has suggested that people tend to
satisfice (a cross between
satisfy and
suffice ), that is, to make a “good-enough” assessment for their purposes, and to make more precise determinations based on explicit decision rules if the need arises
(32) . Other research on categorization has suggested that the way people classify objects in a given domain reflects their goals
(33), and such goals are overlapping but not identical in research and practice. In light of the dearth of research showing any treatment implications of clinical versus subthreshold symptoms (e.g., whether the patient meets four versus five criteria of a given personality disorder), making a “good-enough” assessment—particularly one that also captures subthreshold pathology not normally diagnosable using DSM-IV—may actually be a reasonable strategy. We suspect that clinicians already rely heavily on prototype matching in everyday diagnosis
(16,
34,
35) . Formalizing the prototypes clinicians use and selecting the attributes embedded in these prototypes empirically represent a way of minimizing idiosyncratic elements of diagnosis in clinical practice.