In 1996, Chambers and colleagues (1) reported that exposure to fluoxetine in the third trimester of pregnancy was associated with an increased risk of preterm birth, small-for-gestational-age infants, admission to special care nurseries, and poor neonatal adaptation, including respiratory difficulty, cyanosis on feeding, and jitteriness. This landmark article generated substantial concern among clinicians that third-trimester exposure to fluoxetine (and potentially other selective serotonin reuptake inhibitors [SSRIs]) was contributing to adverse outcomes in pregnancy. Of interest, no adverse effects from first -trimester exposure were observed. The offspring of women who discontinued fluoxetine before 25 weeks’ gestation had neonatal outcomes that were similar to those of comparison subjects. Similarly, in a study of maternity hospital discharge and pharmacy records, Simon et al. (2) reported that exposure to SSRIs was associated with a 0.9-week decrease in mean gestational age, a 175-g decrease in mean birth weight, and a 0.29 decrease in mean APGAR score 5 minutes after birth. The differences in birth weights and APGAR scores were not significant after adjustment for gestational age. Less favorable APGAR scores were limited to those with third-trimester exposure. Neither tricyclic antidepressant nor SSRI exposure was significantly associated with congenital malformations or developmental delay. There were no differences in infant outcome among tricyclic-exposed infants compared to unexposed newborns, which suggested a specific effect of the SSRI rather than maternal depression. In infants born to women treated with antidepressants throughout pregnancy, CNS, motor, respiratory, and gastrointestinal signs that are usually mild and subside by 2 weeks of age have been reported (3, 4) . This neonatal behavioral syndrome resulted in the Food and Drug Administration’s (FDA’s) recommendation for inclusion of this risk in the labeling of these agents.
In contrast, the Canadian Motherisk group prospective study of exposure to tricyclic antidepressants or fluoxetine during the entirety of pregnancy revealed no differences in either maternal weight gain or infant birth weights in treated versus healthy comparison mothers (5) . An intriguing aspect of this study is that the mean scores for the Center for Epidemiologic Studies Depression Scale were reported for the subjects: fluoxetine-exposed group=39.9, tricyclic-exposed group=28.0, and comparison group=10.7. Because a score of 16 is used as the cutoff point to signal significant depression, the implication is that antidepressant medications are not fully effective for remission of depression in the average pregnant patient. Therefore, studies of reproductive outcomes related to drug exposure likely include exposures to both the drug and the active (underlying) disorder in a substantial number of women. If SSRIs are contributing to reduced fetal growth, understanding the mechanism(s) that explain this relationship is of major clinical importance. Chambers and colleagues (1) could not attribute the reduced birth weight and length exclusively to the effects of fluoxetine. Mothers exposed to fluoxetine in late gestation also gained less weight than unexposed mothers. Entry of the weight gain variable into the multivariable models for birth weight and length reduced the effect of the drug, which suggested that weight gain may be in the causal pathway from fluoxetine exposure to size at birth. Chambers et al. speculated that maternal weight gain was reduced either because fluoxetine lowered appetite as a direct side effect or because third-trimester drug use was a marker for serious depression (C.D. Chambers, personal communication, 2005), which can also cause poor appetite and weight loss. The women who were taking medication through the third trimester were more likely to have severe depression than those who discontinued the drug. Women with histories of suicide attempts, marked functional impairment without medication, or partial response are less likely to stop medication during pregnancy.
For psychiatrists, a conundrum is the inclusion of these disparate findings within a comprehensive risk-benefit discussion for SSRIs or use of serotonin-norepinephrine reuptake inhibitors during pregnancy. Monitoring maternal weight gain along with other potential side effects has been recommended (6), with intervention strategies should suboptimal weight gain emerge. Inadequate weight gain during pregnancy has been shown to consistently increase the risk of preterm birth and infant growth restriction (7), which are among the main contributors to perinatal morbidity and mortality in the United States. In an effort to optimize birth outcomes, the Institute of Medicine recommended ranges for the rate of maternal weight gain and total weight gain (7) . Because the effect of gestational weight gain on birth outcomes is modified by the mother’s prepregnancy weight and height, weight gain recommendations vary based on maternal prepregnancy body mass index (kg/m 2 ). For instance, the Institute of Medicine recommended that women with a prepregnancy body mass index of 19.8 to 25.9 kg/m 2 (considered normal weight) should gain a total of 25 to 35 lb during pregnancy at a rate of 0.9 lb per week in the second and third trimesters. To implement these guidelines, the Institute of Medicine encouraged health care providers to do the following:
Measure maternal weight at each prenatal visit and plot weight on a chart included in the obstetric record (see Figure 1 for an example),
Talk to women about the importance of weight gain and set a weight gain goal together,
Monitor the pattern of weight gain at each visit relative to the established goal,
Determine the cause for any abnormal weight gain, and
Develop and implement action to correct abnormal weight gain with the women (7) .
A depressed pregnant woman who was enrolled in a research protocol that involved antidepressant use during pregnancy provided the opportunity to longitudinally dissect the contributions of SSRI use, appetite change, and depressive symptoms to weight gain trajectory and to implement the guidelines recommended by the Institute of Medicine.
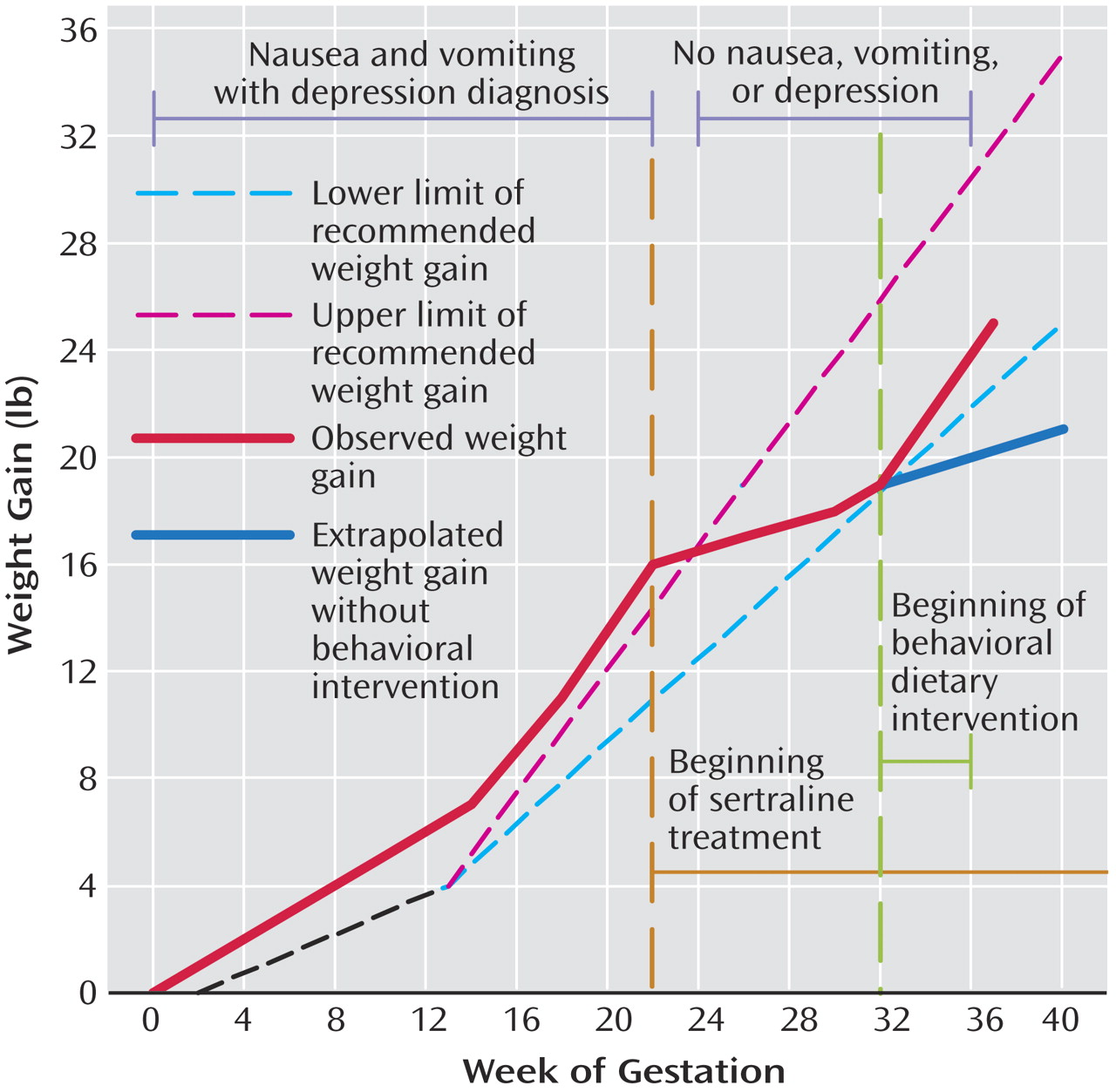
Figure 1. Gestational Weight Gain of Ms. A During Intervention With Sertraline Treatment and Change in Diet
Case Presentation
Ms. A, a 32-year-old married nurse, was referred by her obstetrician to our specialized perinatal clinical research program for evaluation and treatment of major depression during pregnancy. At her evaluation at 20 weeks’ gestation, she reported mild depressive symptoms before conception that increased in intensity soon after conception. Ms. A reported spontaneous tearfulness, low mood, and anhedonia that was present continuously and produced a moderate impairment in her ability to function at home. She had initial insomnia, psychomotor retardation, guilt, and difficulty with concentration. She reported no suicidal ideation, psychotic or manic symptoms, or substance use. Ms. A reported persistent daily nausea and occasional vomiting (2–3 mornings per week) that began immediately after conception. Although she reported a diminished appetite, she was able to maintain an adequate weight gain during the first half of her pregnancy ( Figure 1 ).
Ms. A experienced her first episode of major depression after her mother died 4 years before the evaluation. She had a course of therapy targeted toward her profound grief. Although it was helpful, her symptoms did not resolve until pharmacotherapy (fluoxetine, 20 mg/day) was prescribed by her obstetrician. Ms. A discontinued the fluoxetine after several months without consultation. Subclinical depressive symptoms returned within months of the discontinuation and continued until the time of conception of the index infant, when they again increased to the level of a full depressive episode, as described. Her family history was negative for psychiatric disorders.
The index pregnancy was Ms. A’s second. Both pregnancies were conceived with intrauterine insemination. Her previous pregnancy resulted in a preterm vaginal delivery of healthy twins at 34 weeks’ gestation. During Ms. A’s current pregnancy, the results of her antenatal urine drug screen, hematology counts, metabolic screen, thyroid function tests, and blood pressure were unremarkable. Her ultrasound scan at 20 weeks’ gestation revealed a normal singleton fetus. The intrauterine gestational age correlated accurately with dating by her menstrual cycle. Her past medical history was significant for ulcerative colitis, which was in remission at the time of the pregnancy. Ms. A was 5 feet, 4 inches tall and weighed 145 lb before becoming pregnant, which corresponded to a prepregnancy body mass index of 24.9 kg/m 2 (defined as normal weight by the Institute of Medicine) (7) .
At 20 weeks’ gestation, Ms. A received a comprehensive psychiatric assessment with the Structured Clinical Interview for DSM-IV Axis I Disorders, Patient Edition (SCID-P) (8) . The authors assessed symptom severity with the Structured Interview Guide for the Hamilton Depression Rating Scale—With Atypical Depression Supplement (SIGH-ADS) (9), that includes 17- and 19-item versions with questions from all previous versions of the Hamilton Depression Rating Scale (10), as well as atypical depressive symptoms. On the 29-item and 17-item versions of the SIGH-ADS, her scores were 22 and 18, respectively. Ms. A’s symptoms fulfilled criteria for major depression (recurrent) and dysthymic disorder. She had no history of eating disorders or substance abuse.
Ms. A was provided with education about her chronic mood disorder and the treatment options according a pregnancy risk-benefit model (11), which included information on the risks of intrauterine fetal death, physical malformations, fetal growth effects, neurobehavioral abnormalities, and neonatal toxicity. To summarize the information about taking SSRIs for a woman at 20 weeks’ gestation, no evidence of increased risk for any outcome other than decreased growth and neonatal behavioral syndrome has been reported in humans (1, 5, 12) . Because of her positive response to fluoxetine in the past, Ms. A elected pharmacotherapy treatment. She remarked, “This is best for both me and my family. We can’t take this struggle anymore.” However, she preferred sertraline therapy because of discomfort about the reported growth effects and neonatal toxicity of fluoxetine. Additionally, she preferred sertraline for breast-feeding, which she planned as her newborn feeding method. We advised her to consider that she might not respond to an agent with which she had no experience, but she was firm in her desire for a trial of sertraline. Ms. A started sertraline, 50 mg/day, at 22 weeks’ gestation with the agreement of her obstetrician. We continued to longitudinally monitor her symptoms as part of our research protocol. Within 2 weeks, a clinical assessment revealed that her mood symptoms no longer met criteria for major depressive disorder. Her excellent response to sertraline was sustained throughout her pregnancy and a 26-week follow-up period ( Table 1 ). In addition, her morning nausea was transient and her vomiting had remitted.
Ms. A’s obstetrician was satisfied with her remission of depression but contacted our team at her 32nd gestational week because she was not gaining weight adequately. She weighed 164 lb, which reflected a weight gain of 19 lb from her prepregnancy weight of 145 lb. This total weight gain fell within the Institute of Medicine’s recommended range for 32 weeks of gestation ( Figure 1 ). Of interest, despite depression and nausea/vomiting before 22 weeks’ gestation, Ms. A gained weight appropriately. However, since starting sertraline treatment at 22 weeks, Ms. A’s rate of weight gain over the 10-week period (0.3 lb/week) was substantially lower than the 0.9 lb/week recommended rate of gain for a woman of normal weight before pregnancy (7) . The Institute of Medicine advised that weight gain of less than 2 lb per month in the second or third trimesters warranted further evaluation, which includes a differential diagnosis as well as development and implementation of action to correct weight gain (7) .
In the differential diagnosis of poor weight gain were hyperthyroidism (ruled out by laboratory assessment), unreported eating disorder (ruled out by Ms. A’s report, which was corroborated by her husband), unreported substance abuse (a negative urine drug screen), and poor dietary intake. Another consideration was the use of an SSRI in the final trimester, although the only agent that had been associated with lower maternal weight gain and smaller newborns was fluoxetine (1) . Ms. A reported that immediately after starting sertraline treatment, she lost her appetite completely. She said, “I’m just not hungry. I go through the day running around after the twins, and I realize I have not eaten. I try to eat, but it’s hard when you don’t feel hungry.” Ms. A remarked, “It seems strange to me that I gained weight just fine when I was vomiting and depressed; now I feel much better, but I’m just not hungry, and when I eat, I feel full right away.” She did not recall appetite suppression related to her previous treatment with fluoxetine.
Both the obstetrician and our team reviewed the weight gain recommendations of the Institute of Medicine with Ms. A. We discussed the importance of weight gain in the final trimester of pregnancy and showed the graphic representation ( Figure 1 ) of her weight trajectory across pregnancy as a visual educational tool. We stressed that her current rate of gain could pose risks to her newborn’s well-being. If she continued to gain weight at 0.3 lb/week throughout the remaining weeks of her pregnancy, she would gain only an additional 2.4 lb by 40 weeks’ gestation, resulting in a total of 21.4 lb. This total gain would be less than the recommended range of the Institute of Medicine of 25 to 35 lb for a woman with a normal weight before pregnancy (7) . We presented the options of discontinuing sertraline treatment or implementing a behavioral intervention. Ms. A was committed to continue taking sertraline, which she judged to be more efficacious than fluoxetine because of her full remission. She was able to understand and act upon the fact that in order to gain weight at a more appropriate rate for the remainder of her pregnancy, she could no longer use her appetite as a signal to prompt her to eat.
With our team’s input and support, she scheduled six small meals per day, as recommended by the Institute of Medicine for pregnant women with inadequate weight gain and lack of appetite (13) . She was instructed to enlist her husband in acting as a monitor of her eating and to help her keep nutritious, nutrient-dense small meals and snacks readily available in their home. She generated a list of nutritious foods that had been appealing before her appetite loss, including half sandwiches made with whole wheat bread and cheese or meat, energy bars, cereal bars, peanut butter and whole wheat crackers, dried fruit, mixed nuts, granola or other cereal in full-fat yogurt, instant breakfast mixes with whole milk, ice cream, milk shakes, and pudding. The goal was to choose foods that were energy dense, high in protein and important micronutrients, easy to prepare and eat rapidly, and could be kept available for snacking as well as small meals. Systematic tracking of both her depressive symptoms and weight was accomplished throughout the remainder of her pregnancy ( Figure 1 ).
Ms. A gained 6 lb after the behavioral intervention for a total of 25 lb at her delivery at 37 weeks’ gestation. A 25-lb weight gain at 37 weeks is considered adequate by the standards of the Institute of Medicine (14) . Her sertraline dosage was maintained at 50 mg/day throughout the pregnancy and to 26 weeks’ postpartum. Ms. A reported that despite continuing to take sertraline after delivery, her appetite returned to normal, and she resumed her normal eating patterns. At 3 months’ postpartum, Ms. A had returned to her prepregnancy weight.
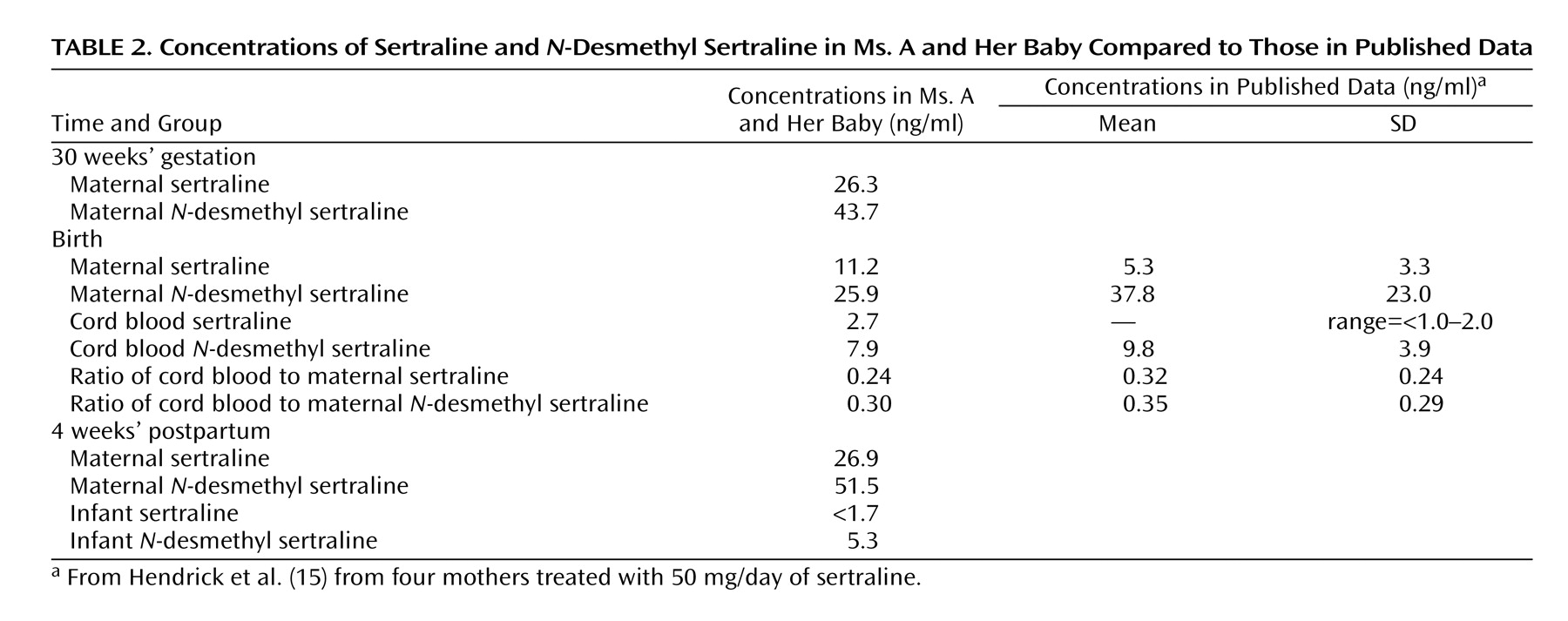
Ms. A delivered a healthy full-term male infant. His birth weight was 3880 g (90th–95th percentile), his length was 52 cm (75th percentile), and his head circumference was 35 cm (50th percentile). His APGAR scores were 9 and 9 at 1 and 5 minutes, respectively. In the first 2 postpartum weeks, no signs consistent with neonatal syndrome were observed (3, 4) . Within the research protocol, several assays of sertraline and its metabolite, N -desmethyl sertraline, were obtained from Ms. A and her son ( Table 2 ). No dose adjustment was required to maintain antidepressant efficacy in the latter part of pregnancy, as has been observed in some women (16) . Maternal and cord blood values were comparable to those obtained by Hendrick et al. (15) from four women who were treated with the same dose of sertraline (50 mg/day) during pregnancy and the postpartum period. The breast-fed infant’s serum levels at 4 weeks of life were consistent with a substantial body of published data that typically revealed sertraline levels at or lower than the levels of quantifiability and N -desmethyl sertraline levels <10 ng/ml (17) .
The infant’s growth was normal. Consistently across the first year, his growth progressed at the 75th percentile for weight (11,850 g at 13 months) and at the 75th–90th percentile for length (81.3 cm at 13 months). The infant’s head circumference was at the 95th percentile during his first year (50.2 cm at 13 months). The Bayley Scales of Infant Development (18) was used to assess mental and psychomotor development of the infant at 4, 13, and 21 months. Both the mental development index and the psychomotor development index indicated that the infant was meeting appropriate developmental milestones at 4 months (mental development index score=93, psychomotor development index score=99, age equivalency=4 months). At 13 months, the infant’s mental development was equivalent to 15 months (mental development index=112), and his psychomotor development was equivalent to 11 months (psychomotor development index=80), with the infant showing some slight delays in coordination during independent walking.
At 21 months, the infant’s mental and psychomotor development were equivalent to 20 months (mental development index=96, psychomotor development index=97), and he demonstrated developmentally appropriate progress in both independent use of language and gross motor skills. At 13 and 21 months, the behavioral rating scale from the Bayley Scales of Infant Development was used to assess the qualitative aspects of the infant’s behavior in the domains of emotional regulation, orientation/engagement, and motor quality. At 13 months, the infant’s total behavioral rating scale score was 85 (96th percentile), and at 21 months, his total score was 128 (99th percentile). Both scores are within normal limits for behavioral development. Overall, the infant demonstrated developmental competency within the domains of growth, motor and cognitive development, and emotional development.
Discussion
In this case conference, we described a depressed pregnant woman with normal prepregnant weight for her height who had appropriate gestational weight gain throughout 22 weeks of gestation, despite having significant depressive symptoms, nausea, and vomiting. After starting sertraline treatment at 22 weeks’ gestation for major depression, the patient’s depression rapidly remitted, but she reported a complete loss of appetite and a sense of feeling full after eating very little; her weight gain abruptly decelerated. A behavioral intervention of six scheduled nutritious meals of small volumes remedied the slowing of her weight gain and allowed her to achieve a total weight gain within the range recommended by the Institute of Medicine. She delivered a healthy full-term infant who developed normally. The patient’s slowing weight gain clearly was not due to depression but rather to treatment with sertraline, which caused reduced appetite as a direct side effect. This case illustrates that appropriate weight gain is achievable with an individualized nutrition intervention that overrides dependence upon appetite cues for eating. As demonstrated by our patient’s pregnancy course, lower weight gain in women treated with fluoxetine or other SSRIs may be because of appetite suppression and decreased food intake. Although weight gain has been the primary weight-related side effect of concern in the psychiatric literature, weight loss also occurs with SSRI treatment (19) .
In 176 patients treated with sertraline, the frequency of weight changes reported on a side effect interview after 24 weeks of treatment was 20.2% with weight gain and 12.4% with weight loss (19) . Weight changes across short- and long-term treatment with SSRIs also vary. In women, the rates of meaningful weight change (defined as ≥7% from baseline) after 6 to 8 weeks, 16 weeks, and 24 weeks of SSRI treatment were increases among 1.7%, 7.1%, and 14.2% of women, respectively, and decreases among 12.4%, 7.1%, and 8.4%, respectively (20) . It is noteworthy that the patient continued to take sertraline in the postpartum period, but her appetite returned to normal after delivery. This observation suggests that there was either an interaction between the drug and her appetite that was specific to pregnancy or that the initial appetite suppression was a short-term side effect that subsided coincidentally near the time of the birth. The patient was treated for the final 15 gestational weeks, which corresponds to the time at which the proportion of women who lose weight in a population treated across time diminishes (12.4% to 7.1% at 16 weeks). Research with larger groups of women should examine longitudinally changes in appetite and weight during pregnancy and the postpartum period in medicated women to investigate a potential interaction rigorously. The success of our behavioral intervention with six small structured meals suggests that sertraline was physiologically increasing energy needs that could not be met with increased dietary intake and that the process of appetite loss and intake reduction was balanced. This hypothesis dictates that treatment with any SSRI could present a risk of poor maternal weight gain in some women, which could affect fetal growth and development. Therefore, the mother and fetus should be monitored closely throughout SSRI treatment. Based on our experience with this patient, we present the following recommendations to psychiatrists who care for pregnant patients.
Monitor gestational weight gain with a weight gain grid (13) or work with the patient’s obstetrician to monitor weight gain in all pregnant patients who are treated with an SSRI. Appetite and weight should also be monitored after delivery. If weight loss and appetite suppression have occurred, reduction below a normal body mass index may compromise the recovery of postpartum maternal nutritional reserves and the nutritional composition of breast milk in lactating women. Women who used fluoxetine during breast-feeding had infants with reduced growth throughout the first 6 months of life compared with infants of mothers who breast-fed but did not take fluoxetine after birth (1) . The differential diagnosis of poor weight gain in pregnancy includes appetite loss as a side effect of SSRI treatment. It is appropriate for physicians to refer patients to a registered dietitian for a nutrition consultation to improve weight gain. Registered dietitians in local areas can be found through the search engine provided by the American Dietetic Association (www.eatright.org, click on “Find a Nutrition Professional”). Additionally, the American Dietetic Association provided a summary that physicians can use to guide women in making healthy food choices throughout pregnancy (21) .
Footnotes
Received Feb. 1, 2006; revision received March 15, 2006; accepted March 15, 2006. From the Department of Psychiatry, Western Psychiatric Institute and Clinic, University of Pittsburgh School of Medicine; and the Department of Epidemiology, Graduate School of Public Health, University of Pittsburgh. Address correspondence and reprint requests to Dr. Bodnar, Department of Epidemiology, A742 Crabtree Hall, 130 DeSoto St., Pittsburgh, PA 15261; [email protected] (e-mail).Supported in part by NIMH grants K01-MH-074092 (to Dr. Bodnar, principal investigator), R01-MH-60335 (Dr. Wisner, principal investigator), and MH-30965.The authors thank Aimee Santucci, Ph.D., for interpreting the infant development measures presented.Dr. Wisner is on the speaker’s bureau for Pfizer and GlaskoSmithKline and receives funding from Pfizer to study the pharmacokinetics of ziprasidone in pregnancy.
CME Disclosure: APA policy requires disclosure by CME authors of unapproved or investigational use of products discussed in CME programs. Off-label use of medications by individual physicians is permitted and common. Decisions about off-label use can be guided by scientific literature and clinical experience.
References
1.
Chambers C, Johnson K, Dick L, Felix R, Jones K: Birth outcomes in pregnant women taking fluoxetine. N Engl J Med 1996; 335:1010–1015
Laine K, Heikkinin T, Ekblad U, Kero P: Effects of exposure to selective serotonin reuptake inhibitors during pregnancy on serotonergic symptoms in newborns and cord blood monoamine and prolactin concentrations. Arch Gen Psychiatry 2003; 60:720–726
Moses-Kolko EL, Bogen D, Perel J, Bregar A, Uhl K, Levin B, Wisner KL: Neonatal signs after late in utero exposure to serotonin reuptake inhibitors: literature review and implications for clinical applications. JAMA 2005; 293:2372–2383
Nulman I, Rovet J, Stewart DE, Wolpin J, Pace-Asciak P, Shuhaiber S, Koren G: Child development following exposure to tricyclic antidepressants or fluoxetine throughout fetal life: a prospective, controlled study. Am J Psychiatry 2002; 159:1889–1895
First MB, Spitzer RL, Gibbon M, Williams JBW: Structured Clinical Interview for DSM-IV Axis I Disorders, Patient Edition (SCID-P), version 2. New York, New York State Psychiatric Institute, Biometrics Research Department, 1996
Williams J, Terman M: Structured Interview Guide for the Hamilton Depression Rating Scale With Atypical Depression Supplement (SIGH-ADS). New York, New York State Psychiatric Institute, 2003
Wisner KL, Zarin DA, Holmboe ES, Appelbaum PS, Gelenberg AJ, Leonard HL, Frank E: Risk-benefit decision making for treatment of depression during pregnancy. Am J Psychiatry 2000; 157:1933–1940
Pastuszak A, Schick-Boschetto B, Zuber C, Feldkamp M, Pinelli M, Sihn S, Donnenfeld A, McCormack M, Leen-Mitchell M, Woodland C, et al: Pregnancy outcome following first-trimester exposure to fluoxetine (Prozac). JAMA 1993; 269:2246–2248
Siega-Riz AM, Adair LS, Hobel CJ: Maternal underweight status and inadequate rate of weight gain during the third trimester of pregnancy increases the risk of preterm delivery. J Nutr 1996; 126:146–153
Weissman AM, Levy BT, Hartz AJ, Bentler S, Donohue M, Ellingrod VL, Wisner KL: Pooled analysis of antidepressant levels in lactating mothers, breast milk, and nursing infants. Am J Psychiatry 2004; 161:1066–1078
Sussman N, Ginsberg D, Bikoff J: Effects of nefazodone on body weight: a pooled analysis of selective serotonin reuptake inhibitor- and imipramine-controlled trials. J Clin Psychiatry 2001; 62:256–260
Asberg-Wistedt A, Agren H, Ekselius L, Bengtsson F, Akerblad A: Sertraline versus paroxetine in major depression: clinical outcome after six months of continuous therapy. J Clin Psychopharmacol (Berl) 2000; 20:645–652
Kaiser LL, Allen L: Position of the American Dietetic Association: nutrition and lifestyle for a healthy pregnancy outcome. J Am Diet Assoc 2002; 102:1479–1490
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).
If the address matches an existing account you will receive an email with instructions to retrieve your username
Create a new account
Change Password
Password Changed Successfully
Your password has been changed
Login
Reset password
Can't sign in? Forgot your password?
Enter your email address below and we will send you the reset instructions
If the address matches an existing account you will receive an email with instructions to reset your password.
Change Password
Congrats!
Your Phone has been verified
×
As described within the American Psychiatric Association (APA)'s Privacy Policy and Terms of Use, this website utilizes cookies, including for the purpose of offering an optimal online experience and services tailored to your preferences. Please read the entire Privacy Policy and Terms of Use. By closing this message, browsing this website, continuing the navigation, or otherwise continuing to use the APA's websites, you confirm that you understand and accept the terms of the Privacy Policy and Terms of Use, including the utilization of cookies.