The epidemiology of dissociative disorders has been studied in the general population in Canada
(1) and Turkey
(2), among college students in Canada
(3) and the United States
(4), in chemically-dependent populations in Canada and the United States
(5 –
8), and among general adult psychiatric inpatients in Canada
(9,
10), the United States
(11 –
14), Turkey
(15), Switzerland
(16), Norway
(17), the Netherlands
(18), and Germany
(19) . A series of dissociative identity disorder cases has been described in other countries, including Australia
(20) and Puerto Rico
(21) . These studies have established that dissociative disorders are not rare, but controversy persists concerning whether they occur naturally or are primarily a response to cultural influences and role demands made by therapists
(22 –
27) .
China is a country in which there is little public or cultural awareness of dissociative identity disorder or other forms of chronic, complex, pathological dissociation. We are not familiar with any representation of the disorder on television, in film, in novels or plays, or in popular folklore. The trauma model of dissociation is not taught at medical schools in China, and dissociative disorders are very rarely diagnosed by mental health professionals. China, therefore, is virtually free of cultural or professional contamination concerning dissociative disorders. These assertions concerning the absence of information on dissociation in China are based on the collective experience of the first seven authors of this study, all of whom are Chinese psychiatrists living in Shanghai and working at the study site, Shanghai Mental Health Center.
There are two competing models of pathological dissociation: the trauma model
(28 –
30) and the sociocognitive model
(22 –
27) . The trauma model makes three predictions concerning pathological dissociation: 1) pathological dissociation should occur in any culture in which there is chronic childhood trauma; 2) within any given culture, pathological dissociation should be more frequent among more traumatized subgroups; and 3) pathological dissociation is a psychological reaction to trauma.
According to the sociocognitive model, complex pathological trauma is an artifact of contamination, and trauma is not a relevant etiological variable. The sociocognitive model predicts that 1) pathological dissociation should be absent in any culture free of contamination and role demands for it to occur, and 2) in cultures where pathological dissociation does occur, it is caused by contamination and iatrogenesis, not by trauma. The two models differ on their theories of etiology, and they make distinct predictions concerning epidemiology.
We predicted that a structured interview for dissociative disorders and a self-report measure for dissociation would detect complex pathological dissociation in China. That is, we tested the first predictions of the trauma and sociocognitive models of dissociation. The methodology of our study did not allow a direct test of the traumatic etiology of any dissociation we detected; however, we predicted that higher levels of dissociation would be reported by more traumatized subgroups in Shanghai.
Method
Subjects
This study was approved by the ethics committee and administrators at Shanghai Mental Health Center. The respondents consisted of three groups: inpatients at Shanghai Mental Health Center (N=423), outpatients at Shanghai Mental Health Center (N=304), and a nonclinical sample of workers at a clothing manufacturing factory (N=618). The inpatients were interviewed during Dec. 1998, and they were selected from 950 inpatients screened during that month. Inclusion criteria for the inpatients were that they had to be positive for one of three of the following items: one or more Schneiderian first-rank symptoms of schizophrenia, childhood physical abuse, or childhood sexual abuse.
The outpatients were interviewed during March and April 2000. Every fifth person coming in for an appointment was screened with the same three inclusion criteria used for the inpatients until a total of 304 respondents were collected. Each day, the Shanghai Mental Health Center has between 500 and 800 outpatient appointments scheduled. The factory workers were interviewed in August and Sept. 2000. The manufacturing company provided a list of all employees, and every fifth person on the list was approached for an interview. There were less than five refusals. All the workers had agreed to participate prior to their first meeting with the interviewers, and all were given a small gift as a token of thanks for their participation.
Procedure
All interviews were conducted by a team of 12 psychiatrists. Rater training sessions were held prior to the beginning of data collection. The training consisted of a group discussion of the two measures and the meaning of all scale items and a session in which one person administered the structured interview while all the psychiatrists scored it independently. Further discussion was then undertaken to ensure that scoring decisions were consistent, but no statistical analysis of interrater reliability was conducted.
All subjects completed Chinese versions of the Dissociative Experiences Scale
(29,
31 –35) and the Dissociative Disorders Interview Schedule
(28,
36 –38) . The Dissociative Experiences Scale is a 28-item self-report measure used in over 250 published studies
(39) . It has excellent reliability and concurrent validity with other measures of dissociation
(38) . An eight-item subscale of the Dissociative Experiences Scale yields a conclusion of whether an individual is inside or outside of the dissociative taxon
(34,
35) . Members of the dissociative taxon report pathological experiences not endorsed by nontaxon members. These include experiences such as not recognizing oneself in a mirror and not recognizing family members. General population norms for the Dissociative Experiences Scale on a sample of 1,055 respondents in Winnipeg, Canada are also available
(33) .
The Dissociative Disorders Interview Schedule is a structured diagnostic interview that determines DSM-IV diagnoses of somatization disorder, major depressive disorder, borderline personality disorder, and the five dissociative disorders. In addition, it asks questions about substance abuse, secondary features of dissociative identity disorder, extrasensory/paranormal experiences, and childhood physical and sexual abuse. The Dissociative Disorders Interview Schedule has established reliability and concurrent validity when compared to a clinical interview, the Structured Clinical Interview for DSM-IV Dissociative Disorders
(40 –
44), and the Dissociative Experiences Scale-T
(34,
35) . When respondents in a survey of general adult psychiatric inpatients were categorized as having no dissociative disorder, dissociative identity disorder, or dissociative disorder not otherwise specified, the Dissociative Disorders Interview Schedule has rates of agreement (using Cohen’s kappa) of 0.71 with clinician ratings, 0.74 with the Structured Clinical Interview for DSM-IV Dissociative Disorders, and 0.81 with the Dissociative Experiences Scale-T taxon membership. Interviewers in this study were blind to the results of all other measures.
Results
Demographics
There were significant differences among the inpatients, outpatients, and factory workers in terms of age (36.1 years [SD=8.9], 40.7 years [SD=7.0], and 41.7 years [SD=5.9], respectively; F=80.797, p<0.00001), percentage of women (44%, 41%, and 52%; F=6.329, p<0.002), number of children (mean= 0.3 [SD=0.5], 0.4 [SD=0.5], and 1.0 [SD=0.4]; F=351.199, p<0.00001), and percentage who were married (28%, 37%, and 92%; F=417.076, p<0.00001).
Childhood Trauma History
There were significant differences among the inpatients, outpatients, and factory workers in terms of the rate of childhood physical abuse (5.4% [N=23], 13.1% [N=40], and 0.1% [N=1], respectively; F=40.504, p<0.00001). While the groups did not differ in rate of childhood sexual abuse (2.8% [N=12], 3.0% [N=9], and 0.0% [N=0]), when the two forms of trauma were combined, a significant difference among the groups was found (7.8% [N=33], 14.5% [N=44], and 0.1% [N=1]; F=42.959, p<0.00001).
Diagnoses
There were no cases of somatization disorder. There were significant differences among the inpatients, outpatients, and factory workers in prevalence of the following disorders queried in the Dissociative Disorders Interview Schedule: substance abuse (2.8% [N=12], 2.0% [N=6], and 8.3% [N=51], respectively; F=11.76, p<0.00001), dissociative amnesia (0.2% [N=1], 1.3% [N=4], and 0.2% [N=1]; F=3.37, p<0.04), dissociative fugue (0.0%, 1.3% [N=4], and 0.0%; F=6.92, p<0.001), and a dissociative disorder of some type (1.7% [N=7], 5.0% [N=15], and 0.3% [N=2]; F=12.59, p<0.00001). Other disorders diagnosed among the inpatients, outpatients, and factory workers were major depressive episode (6.4% [N=27], 7.6% [N=23], and 2.6% [N=16]), borderline personality disorder (1.7% [N=7], 1.3% [N=4], and 0.3% [N=2]), depersonalization disorder (0.2% [N=1], 0.0%, and (0.2% [N=1]), dissociative identity disorder (0.5% [N=2], 0.3% [N=1], and 0.0%), and dissociative disorder not otherwise specified (0.7% [N=3], 2.0% [N=6], and 0.0%). Membership in the dissociative taxon on the Dissociative Experiences Scale-T was as follows: six inpatients (1.4%), six outpatients (2.0%), and three factory workers (0.5%), a nonsignificant difference.
Symptoms
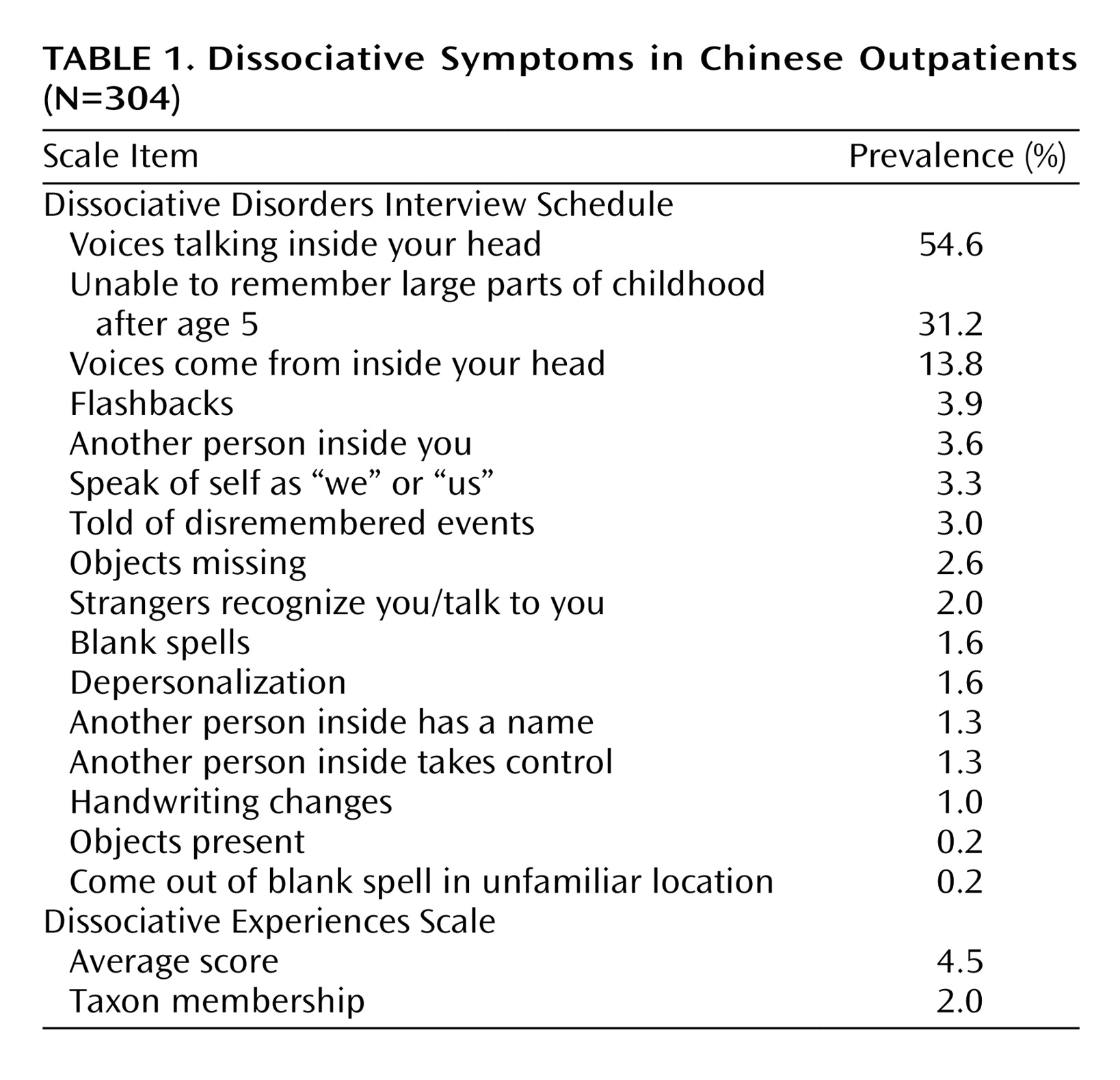
There were significant differences among the inpatients, outpatients, and factory workers on the following sections of the Dissociative Disorders Interview Schedule: somatization symptoms (1.2 [SD=2.0], 2.1 [SD=2.9], and 1.9 [SD=2.5], respectively; F=14.76, p<0.00001), positive substance abuse items (0.03 [SD=0.2], 0.02 [SD=0.2], and 0.08 [SD=0.3]; F=10.64, p<0.00001), Schneiderian symptoms (1.9 [SD=1.9], 2.8 [SD=2.3], and 0.01 [SD=0.2]; F=414.11, p<0.00001), secondary features of dissociative identity disorder (0.9 [SD=1.1], 1.3 [SD=1.2], and 0.5 [SD=0.7]; F=65.64, p<0.00001), borderline personality disorder criteria (0.4 [SD=1.0], 0.5 [SD=1.0], and 0.2 [SD=0.6]; F=19.71, p<0.00001), and extrasensory/paranormal experiences (0.5 [SD=1.3], 0.3 [SD=0.8], and 0.2 [SD=0.6]; F=12.54, p<0.00001). Symptoms of the outpatients are shown in
Table 1 .
The average score on the Dissociative Experiences Scale was 4.1 (SD=7.5) for inpatients, 4.5 (SD=7.9) for outpatients, and 2.6 (SD=4.3) for factory workers, a significant difference (F=11.64, p<0.00001).
Discussion
The results of our study support the epidemiological prediction of the trauma model of dissociation and are not consistent with the sociocognitive model. Pathological dissociation was reported by Chinese respondents, despite the lack of contamination, role demands, and iatrogenic suggestion in China. Pooling the 1,345 Chinese respondents, a dissociative disorder of some type was diagnosed in 24 individuals by the Dissociative Disorders Interview Schedule, while 15 respondents were in the dissociative taxon on the Dissociative Experiences Scale. There were three individuals with dissociative identity disorder.
As shown in
Table 1, there are hints in the secondary features of dissociative identity disorder that full or partial forms of dissociative identity disorder could affect more than 2.3% of the Chinese outpatient sample (the sum of the frequencies of these two diagnoses on the Dissociative Disorders Interview Schedule). For instance, 3.6% of the Chinese outpatients said that they have another person inside of them.
The outpatients reported more childhood trauma than the other two groups. The outpatients had more dissociative disorders on the Dissociative Disorders Interview Schedule, more members of the dissociative taxon on the Dissociative Experiences Scale, higher average scores on the Dissociative Experiences Scale, and more secondary features of dissociative identity disorder on the Dissociative Disorders Interview Schedule. Thus, the outpatients were more dissociative than the other two groups on four different ways of assessing dissociation. The fact that they also reported more childhood abuse is consistent with the trauma model of pathological dissociation.
Our study has several strengths and limitations. All interviews were conducted by practicing psychiatrists; three separate samples of Chinese respondents were included; and the measures used have established reliability and validity
(32,
34,
35,
44) . China provides an example of a culture largely uncontaminated by popular or professional knowledge of dissociative identity disorder and therefore is suitable for testing the epidemiological predictions of the trauma and sociocognitive models.
The limitations of this study include the fact that all respondents were from one Chinese city, and therefore the results may not be generalizable to China as a whole. This limitation does not affect the test of the study’s primary hypothesis, however. There may have been unrecognized problems with the translations of the Dissociative Experiences Scale and Dissociative Disorders Interview Schedule that affected the validity of the findings. In addition, the meaning of some responses may have been misunderstood because of unrecognized cultural factors. These two possible limitations are tempered by the fact that the interviews were conducted by Chinese psychiatrists practicing in Shanghai.