Bipolar disorder (types I and II) affects 1%–2% of the population and occurs commonly in women during childbearing years
(1). Despite this relatively high prevalence, remarkably little is known about the risk of recurrence of bipolar illness during pregnancy, although major affective disorders, including psychotic forms, are quite common in pregnancy
(2). The postpartum period is widely considered a high-risk period for recurrence of potentially severe and life-threatening recurrences of often-psychotic major affective illness, and thus it has received more systematic study
(3–
12). A traditional view is that pregnancy may protect against recurrence of major affective disorders or suicide. However, this impression is based on very limited data
(13,
14), and several reports have suggested that pregnancy is not associated with altered recurrence risk in bipolar illness
(15–
17). Recurrences of mania and bipolar depression are not uncommon during pregnancy
(18–
21), and lithium has been used safely during pregnancy by many patients
(22–
25).
Management of pregnant women with bipolar disorder poses several clinical dilemmas. First, commonly employed antimanic agents (e.g., lithium, valproate, and carbamazepine) all carry some fetal teratogenic risk in early pregnancy and potential adverse effects during late pregnancy, labor, and delivery
(26–
33). Second, the impact of untreated psychiatric illness during pregnancy often appears to be discounted in decisions regarding maintaining or discontinuing a mood stabilizer. Finally, interruption, especially abruptly, of ongoing treatment with lithium—and perhaps other mood stabilizers—is associated with high risk of early relapse that can exceed rates predicted by the natural history of untreated manic-depressive illness
(34–
38) and may contribute to higher suicidal risk
(39,
40). However, optimal clinical management of pregnant women with bipolar disorder only recently has begun to be examined critically. Treatment guidelines can be further refined as predictions of risk for bipolar disorder recurrence during pregnancy improve
(25,
31,
33,
41–
43). Specifically, it remains to be established whether pregnancy is associated with either a greater or lower risk of recurrence of mania or bipolar depression and whether pregnant and nonpregnant women respond differently to treatment discontinuation.
We now report on a retrospective assessment of recurrence risk in gravid and nongravid women with DSM-IV bipolar I or II disorder who elected to discontinue lithium maintenance treatment. This is the first study to compare 1) bipolar disorder recurrence risk after lithium discontinuation at different rates in a substantial number of pregnant and nonpregnant women, and 2) recurrence rates after discontinuing lithium in pregnancy with the recurrence rates of the same patients in the period preceding treatment discontinuation.
METHOD
We examined the clinical course of DSM-IV bipolar I or II disorder in 42 pregnant and 59 nonpregnant women aged 16–50 years who discontinued lithium either rapidly (over 1–14 days) or gradually (15–30 days), as defined previously
(35–
37). The pregnant women discontinued treatment within 6 weeks of the date of conception. The subjects had an overall mean of 3.94 years (SD=3.40) of maintenance treatment. Subjects were obtained from the Perinatal and Reproductive Psychiatry Research Program at Massachusetts General Hospital in Boston and the Lucio Bini–Stanley Foundation Center for Mood Disorders Research in Cagliari, Sardinia. In addition, comparison data were obtained for the same women from the year before they discontinued lithium, as well as from another nine women who elected to continue lithium treatment throughout their pregnancy. Patients were advised of the relative risks of fetal exposure to psychotropic drugs and of recurrences of illness during maintenance treatment and after discontinuation of mood stabilizers, to the extent that these could be estimated
(20,
26–
33). In the nongravid comparison group, decisions regarding lithium discontinuation arose clinically, usually at the patient’s insistence after periods of relative euthymia (75% of cases) or in response to treatment-emergent adverse effects (25% of cases). All subjects provided informed consent for review and anonymous reporting of information pertaining to their clinical course. The study protocol was approved by the institutional review board at Massachusetts General and McLean Hospitals and by corresponding officials at the University of Cagliari Medical Center.
Demographic and clinical information was recorded systematically from semistructured interviews and review of clinical records. Recurrence was defined as a new episode of mania (or hypomania) or major depression that met DSM-IV criteria at any time during pregnancy or postpartum or within corresponding periods for nongravid women (weeks 1–40 and weeks 41–64, respectively), as well as during the year of maintenance treatment preceding lithium discontinuation.
Analyses included contingency tables (chi-square or Fisher’s exact p), analysis of variance (F), and Kaplan-Meier survival analysis (Mantel-Cox or Wilcoxon chi-square), determined with Statview-V programs for the Macintosh microcomputer (SAS Corp., Cary, N.C.). Data are means and standard deviations, survival-computed times (with standard errors), or proportions (with 95% confidence intervals [CI]), at stated degrees of freedom (df); statistical results yielding p>0.05 (two-tailed) were considered nonsignificant (n.s.). All clinical and analytical methods used have been detailed previously
(37–
39).
RESULTS
First, among women with bipolar illness who discontinued lithium maintenance treatment, comparisons were made between the 42 pregnant women followed throughout their pregnancy and for 24 weeks postpartum and the 59 nongravid women followed through equivalent periods (weeks 1–40 and 41–64). The pregnant and nonpregnant subjects were of similar age at illness onset (mean=22.72 years [SD=4.46] and mean=23.31 [SD=8.43], respectively) and at lithium discontinuation (mean=32.53 [SD=4.95] and mean=32.81 [SD=9.54]) (both F values ≤0.170, df=1, 99, n.s.). They also did not differ significantly in the proportion with bipolar I disorder (73.81% [N=31] and 62.71% [N=37]) or with respect to previous illness (proportion with four or more prior episodes: 64.29% [N=27] and 59.32% [N=35]; χ2=0.03–2.55, df=1, n.s.). However, a somewhat higher proportion of the pregnant women discontinued lithium rapidly (73.81% [N=31] versus 54.24% [N=32]; χ2=4.00, df=1, p=0.05).
Recurrence Risks After Lithium Discontinuation
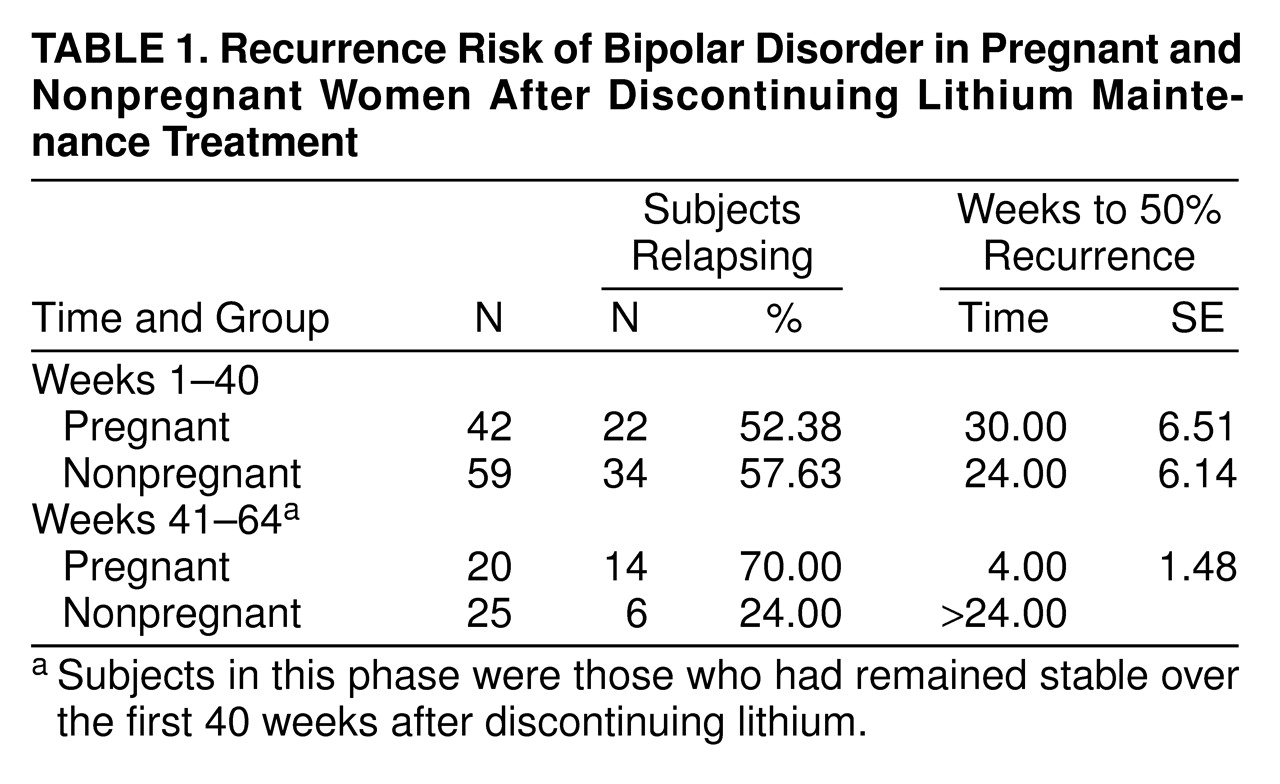
During the first 40 weeks after lithium discontinuation, there was little difference in recurrence rates between pregnant and nonpregnant women (52.38% [N=22 of 42] and 57.63% [N=34 of 59], respectively; χ2=0.273, df=1, n.s.) The overall recurrence rate was 55.45% (N=56 of 101). In contrast, among women who remained euthymic for 40 weeks after discontinuing lithium, significantly more pregnant subjects experienced a recurrence postpartum (70.00% [N=14 of 20]) than did the nonpregnant subjects during the corresponding time (24.00% [N=6 of 25]) (χ2=13.94, df=1, p=0.0002). None of the nine women with bipolar disorder who continued lithium treatment during pregnancy relapsed during weeks 1–40, but three (33.33%) experienced a recurrence soon after delivery (all within 2 weeks) despite continued maintenance treatment.
Over the entire 64-week period of risk after lithium discontinuation, recurrences were very common for both the pregnant/postpartum and the nonpregnant women (85.71% [N=36 of 42] and 67.80% [N=40 of 59], respectively). Among all subjects, the polarity of recurrent episodes was as follows: manic or hypomanic, 50.00%; depressive, 39.74%; and mixed-dysphoric, 10.26%. Among the pregnant subjects, the proportion of depressive or mixed episodes was similar during pregnancy and the postpartum period (63.64% and 62.50%, respectively; χ2=1.19, df=1, n.s.). However, depressive/mixed-dysphoric episodes were significantly more common among the pregnant/postpartum women than in nongravid subjects (63.16% versus 37.50% of episodes; χ2=5.13, df=1, p=0.02).
Survival Analyses
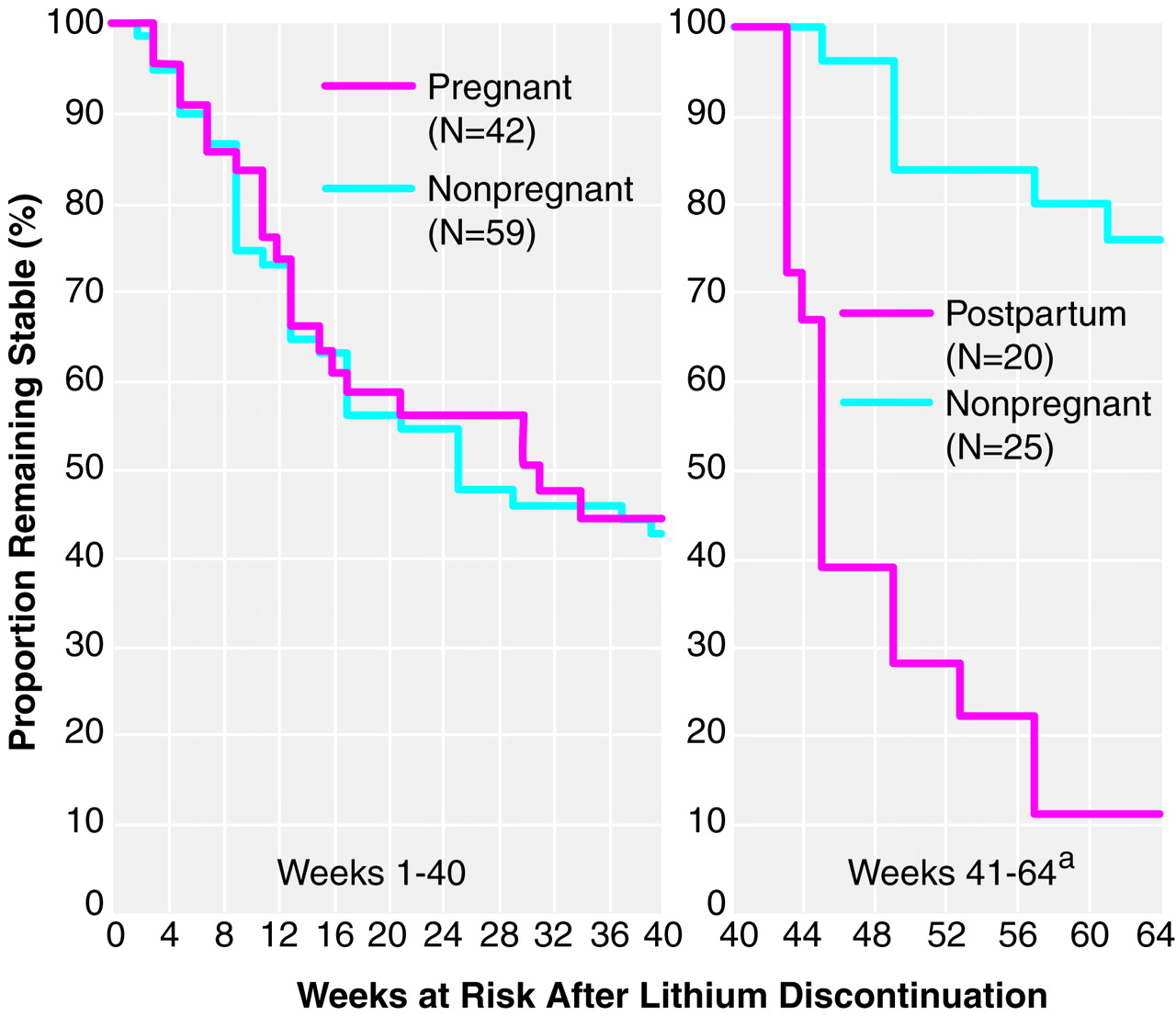
Kaplan-Meier survival functions over the initial 40 weeks after discontinuation of lithium maintenance treatment were compared for the pregnant and nonpregnant women (
figure 1,
table 1). The resulting computed time to 50% risk was 30.00 weeks (SE=6.51) in the pregnant women (43.92% remained stable throughout pregnancy without lithium) versus 24.00 weeks (SE=6.14) in nonpregnant women (of whom 42.37% remained stable for 40 weeks without lithium). These differences were not significant (χ
2=0.057, df=1, n.s.;
table 1). Secondary analyses based on matching for rapid discontinuation also did not reveal significant differences in recurrence risks between pregnant and nonpregnant women in the first 40 weeks after discontinuing treatment. Their respective computed times to 25% risk after rapid discontinuation were 10.00 weeks (SE=1.78) versus 8.00 weeks (SE=1.74) (χ
2=2.54, df=1, n.s.). These findings suggest that pregnancy did not appreciably protect against risk associated with lithium discontinuation.
In contrast to the high rate of recurrences within 40 weeks after discontinuing lithium (55.45%), the recurrence rate among the same 101 women during the year before discontinuing was much lower (20.79% [N=21 of 101]). None of the nine pregnant women who elected to continue lithium treatment experienced a recurrence during their pregnancy. The survival function obtained from the pooled results of all 101 women during lithium maintenance, starting at 1 year before discontinuation, differed highly significantly from the survival function after discontinuation of lithium (time to 25% recurrence: >40 weeks during maintenance treatment versus 10.00 weeks [SE=2.62] after discontinuing lithium; χ2=36.20, df=1, p<0.0001). Serum lithium concentration during maintenance treatment averaged 0.620 meq/liter (SD=0.125).
Additional survival analyses were carried out among pregnant (N=20) and nonpregnant women (N=25) who remained stable throughout the first 40 weeks after stopping lithium (excluding two cases with episodes in both pregnancy and the puerperium). In contrast to the very similar early recurrence risk seen during weeks 1–40, recurrences of mania or depression in weeks 41–64 after discontinuing lithium were much greater in postpartum women. Computed time to 50% recurrence risk was only 4.00 weeks (SE=1.48) after pregnancy and indeterminate (>24 weeks) in women who had not been pregnant. Only 30.00% of 20 women without recurrence during pregnancy remained stable postpartum, but 76.00% of 25 nonpregnant comparison subjects remained stable through the additional 6 months of follow-up (by survival analysis, χ
2=22.00, df=1, p<0.0001) (
figure 1,
table 1).
Rapidity of Lithium Discontinuation Effects
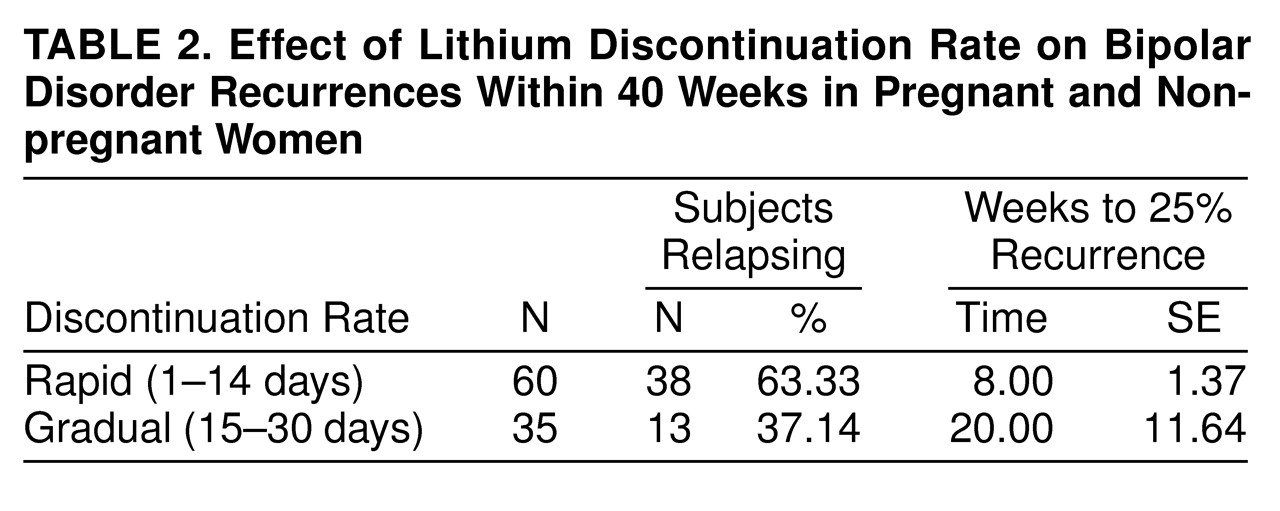
Because of the small number of pregnant patients who discontinued gradually, all subjects (gravid and nongravid) were pooled to evaluate the effect of lithium discontinuation rate. Only weeks 1–40 were considered because of the profound difference in risks in postpartum women versus nongravid women after 40 weeks. As shown in
table 2, the resulting computed time to 25% recurrence risk was 2.50 times shorter after rapid than after gradual lithium discontinuation (χ
2= 7.59, df=1, p=0.006). Moreover, six cases with uncertain discontinuation times yielded an intermediate computed time to 25% recurrence (12.00 weeks [SE=2.89]) between those with rapid and gradual discontinuation rates.
Clinical Factors Associated With Recurrences
The 56 women (pregnant and nongravid) who relapsed during the first 40 weeks after lithium discontinuation were compared to the 45 women who did not. No significant differences were found between these groups in several measures. These included age at onset (F=1.39, df=1, 99, n.s.), years of illness (F=3.76, df=1, 99, n.s.), and proportion of diagnostic subtypes (χ2=0.31, df=1, n.s.). There were also no relationships of these factors to relapse risk at weeks 41–64 (not shown). However, at weeks 1–40, patients with a relatively high number of prior episodes (four or more) had a significantly higher risk than those with 1–3 episodes (66.13% [N=41 of 62] versus 38.46% [N=15 of 39]; χ2=7.42, df=1, p=0.006), with a nonsignificant difference in the same direction at weeks 41–64 (83.87% [N=52 of 62] versus 69.23% [N=27 of 39]; χ2=3.01, df=1, p=0.08).
DISCUSSION
Information remains limited about the risk of recurrence of mood disorders during pregnancy or about the effects on maternal or child health of continuing or interrupting treatment. A recent study reported that pregnant women with preceding recurrent major depression were at significant risk for recurrence after antidepressant discontinuation
(44). However, information regarding risk for recurrence in bipolar women after discontinuation of lithium or other mood stabilizers is very limited, and the effects of treatment discontinuation and acute psychiatric illness on fetal development are virtually unknown
(45). The present study is the first systematic effort to quantify recurrence risk after lithium discontinuation during pregnancy, as well as postpartum, with comparisons to risk during previous lithium maintenance treatment. The study design is far from ideal in that it lacks randomization and prospective or blind assessment and may be affected by subtle mismatching of pregnant and nonpregnant women or by cultural differences between study sites. On the other hand, prospective randomization of women to continue or discontinue maintenance treatment during and after pregnancy for experimental purposes would present severe ethical and clinical challenges.
An important finding of this study was that survival functions after lithium discontinuation were very similar in pregnant and nonpregnant women with bipolar disorder. Recurrence rates also were similar for bipolar I and II subtypes but were higher in patients with a history of four or more prior episodes of illness and for those who underwent rapid discontinuation of lithium. These findings are consistent with our previously replicated findings
(34–
38) with broader study groups of men and mainly nonpregnant women in which we reported that recurrence risk was sharply elevated within the first several months after lithium discontinuation and was much greater after abrupt or rapid discontinuation.
The similar recurrence risks in pregnant and nonpregnant women within the first 40 weeks after stopping lithium may suggest that pregnancy is relatively “risk neutral” or unlikely to exert important protective or risk-enhancing effects. Alternatively, it may well be that lithium discontinuation represents a dominant stressor during the first months after stopping treatment that overshadows any more subtle effects of pregnancy. It is also possible that women were somewhat protected from recurrences of mania or bipolar depression by pregnancy but that such an effect was countered by other factors that contributed to a higher risk than in nonpregnant women, which is perhaps suggested by their experiencing a higher proportion of depressive or mixed episodes after discontinuing lithium than nonpregnant comparison subjects. Although pregnant women did not differ from nonpregnant subjects in onset age, duration of illness, or number of prior episodes, a higher proportion of pregnant women had discontinued lithium rapidly, consistent with fear of potential teratogenic effects of lithium
(30). However, matching on discontinuation rate did not reveal significantly lower risks over time (1–40 weeks) in pregnant versus nonpregnant women. Nevertheless, a potential for effects of uncontrolled variables on the present findings indicates that further studies of the effects of pregnancy on recurrence risk in treated and untreated women with bipolar disorder are required, if ethical and clinically sound study designs can be developed.
Recurrence rates were much higher postpartum than during the equivalent period for nonpregnant women (weeks 41–64). This finding is consistent with many previous reports that the postpartum period brings particularly great risk for women with major affective and psychotic disorders
(3–
11). Postpartum recurrence risk can be reduced in pregnant women with bipolar disorder by lithium prophylaxis in late pregnancy or after delivery
(46–
51). In the present small study group, however, the protection afforded by continuing lithium was not complete, since three of nine pregnant women who elected to continue taking lithium suffered a postpartum recurrence. None of these nine women relapsed while continuing lithium throughout pregnancy, whereas 21 of the 101 women who later discontinued lithium experienced a recurrence in the year before their pregnancy while still being treated with lithium, perhaps suggesting a protective effect of pregnancy. All nine women who continued lithium throughout pregnancy delivered infants without major malformations. Nevertheless, the safety and prophylactic effectiveness of lithium and other alternative treatments, including newer anticonvulsants and antipsychotics, require further investigation in women with bipolar disorder, particularly after the developmentally critical first trimester of pregnancy and into the postpartum period
(52,
53).
Gradually discontinuing lithium limited recurrence risk during the first 40 weeks after discontinuation. This finding supports our previous findings in a broader study group of bipolar disorder patients, which indicated that slower discontinuation of lithium can reduce, and not merely delay, recurrence risk
(35–
38), and perhaps suicide risk as well
(39,
40). Abrupt discontinuation of other maintenance medications, including antipsychotics and antidepressants, has also been associated with a high, early relapse risk
(54,
55). Pending further study of the effects of treatment discontinuation in pregnancy, clinicians managing pregnant women receiving maintenance psychotropic medicines should consider the rate of drug discontinuation as an important risk variable. Although gradual discontinuation of lithium into the first trimester of pregnancy results in greater fetal exposure during organogenesis, this vulnerability may be offset by reducing risk for potentially serious or life-threatening psychiatric illness that may follow rapid discontinuation of lithium, particularly in women with a history of multiple episodes of affective illness
(55).
Appropriate concerns regarding the teratogenic effects of lithium have led to treatment practices that require reconsideration. For example, mood-stabilizing treatment is often discontinued abruptly after diagnosis or anticipation of pregnancy to minimize potential teratogenic risks. This practice needs to be balanced against the high risk of recurrence found soon after discontinuing treatment and unknown effects of drug discontinuation on early fetal development. The impact of untreated psychiatric illness on pregnant women and their offspring is often discounted, perhaps owing to greater concern about fetal malformations. Nevertheless, acute affective or psychotic illness in pregnancy places a woman and her fetus at risk due to impulsive or self-injurious behavior, substance abuse, or inattention to prenatal care, as well as increased exposure to multiple psychotropic drugs at relatively high doses. Moreover, the impact of mania or depression, as well as of drug withdrawal, on fetal development is poorly defined
(56). Stress in pregnant animals can lead to sustained dysfunction of the hypothalamic-pituitary-adrenal system in their offspring
(56–
58), but a clinical counterpart of such effects has not yet been proved. However, untreated affective illness during pregnancy has been associated with adverse neonatal outcomes, including premature delivery, low birth weight, and lower Apgar ratings of neonatal status
(33).
The present findings do not, by themselves, provide an adequate basis for proposing guidelines for the clinical management of pregnant women with bipolar disorder. However, they add compelling evidence that the risks of stopping maintenance lithium treatment, especially abruptly, are similar in pregnant women and in broader clinical samples. Clinicians who manage women with bipolar disorders who are planning to conceive should consider the high risk of relapse associated with lithium discontinuation in the overall risk/benefit assessment.