The association between depression and smoking is well established
(1–
4). Smoking cessation studies have reported a high proportion of smokers (median=32.7%, range=18.5%–60.6%) coming in for treatment with a lifetime history of major depression
(4–
13). Evidence, mostly from case studies, suggests some individuals are at a higher risk for developing major depressive episodes after smoking cessation, particularly those who have a history of depression
(5,
14–
16).
Reports of severe major depressive episodes after smoking cessation indicate that the onset of severe depressive symptoms ranges from 2 days to 6 weeks after the initial abstinence from smoking
(3,
14,
16–
21). In some cases, depression after smoking cessation was resolved with the use of nicotine replacement therapy
(14,
19) or the use of antidepressants
(14); in others, depressive symptoms dissipated after a relapse to smoking
(16,
17). In a study examining the effectiveness of clonidine for smoking cessation
(8), nine participants (3%) developed severe major depressive episodes during the 10-week treatment; seven patients (77.8%) had a history of depression. In another trial of smoking cessation using fluoxetine
(5), five subjects (7%) were diagnosed with major depressive episodes during the 10-week treatment, and all had a history of depression.
Covey and colleagues
(15) examined the predictors of major depressive episodes among 126 smokers who were abstinent at the end of the 10-week, placebo-controlled trial of smoking cessation with clonidine
(8). During the 3-month follow-up, 7.1% (N=9) of the participants experienced major depressive episodes with remarkably higher rates of incidence among smokers with a history of depression (four [17%] of the 24 subjects with a history of single episodes and three [30%] of the 10 subjects with a history of recurrent episodes). The significant predictors of major depressive episodes were having a history of major depression and experiencing elevated withdrawal symptoms at the end of treatment. This study included only smokers who were abstinent; therefore, it was unclear whether cigarette abstinence induced major depression
(15).
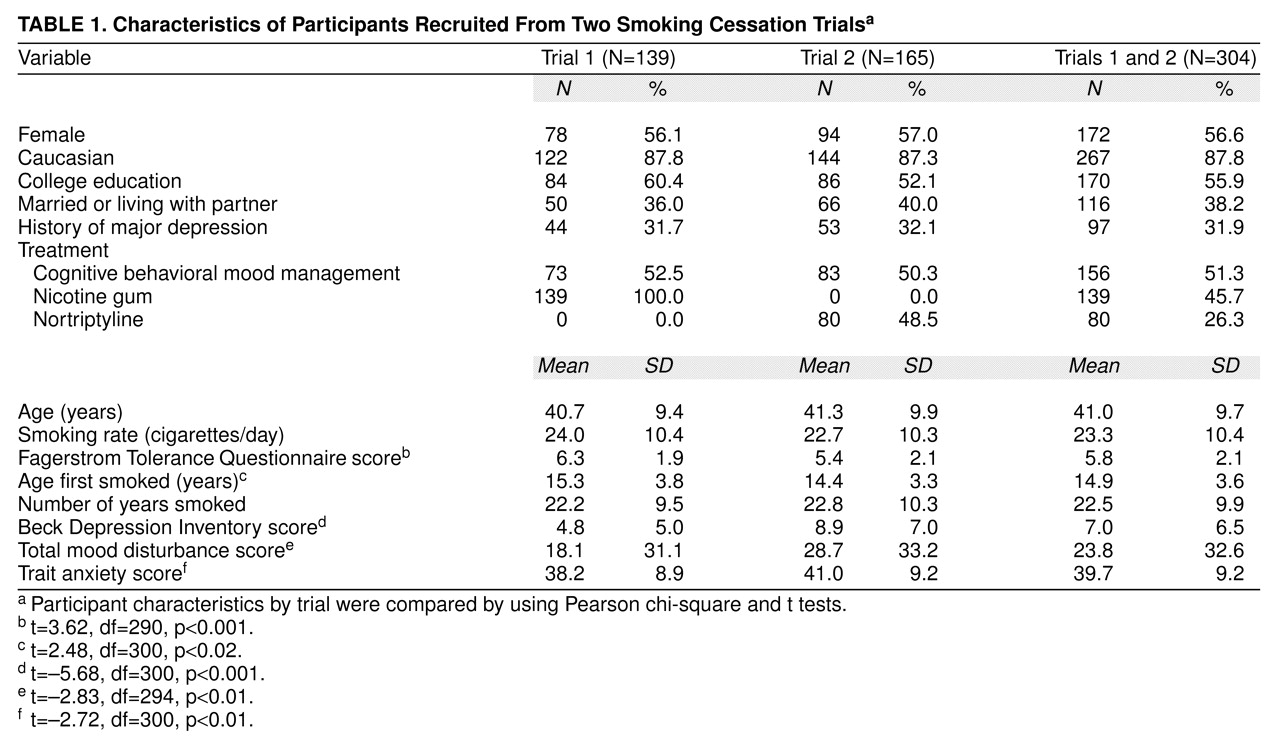
In summary, smoking cessation may be followed by new major depressive episodes, particularly among smokers with a history of depression. To better understand the role of abstinence status, history of depression, and other factors involved in major depression after treatment for smoking cessation, we included smokers who achieved abstinence at the end of treatment and those who relapsed or continued to smoke. The purpose of this study was to investigate the 12-month incidence of major depressive episodes after treatment for smoking cessation and the frequency of depressive symptoms and related impairments and to explore the predictors associated with major depressive episodes after treatment. In addition, two hypotheses were tested: 1) abstinence status at the end of treatment increased the likelihood of major depressive episodes after treatment; and 2) smokers with a history of depression were more likely to develop major depressive episodes after treatment.
RESULTS
Incidence of Major Depression After Treatment
Among the 304 participants, 14.1% (N=43; 95% confidence interval [CI]=10.2%–18.0%) reported a major depressive episode within 12 months after treatment for smoking cessation. The incidence rates across trials were similar (trial 1: N=16, 11.5%, versus trial 2: N=27, 16.4%) (χ2=1.46, df=1, p=0.23, N=304). About half (N=170, 55.9%) of the participants were abstinent from smoking at the end of treatment. Contrary to our hypothesis, there was no significant difference in the 12-month incidence rates of major depressive episodes among those who were abstinent at the end of treatment and those who were not (N=25 of 170, 14.7%, versus N=18 of 134, 13.4%) (χ2=0.10, df=1, p=0.75, N=304). The 12-month incidence rate of major depressive episodes was higher for participants who had a history of depression (23.7%, N=23 of 97; 95% CI=19.4%–28.0%) than for those who had no history of depression (9.7%, N=20 of 207; 95% CI=7.6%–11.8%) (χ2=10.74, df=1, p=0.001, N=304). No difference was found in the incidence rates of major depressive episodes among participants who had a history of a single depressive episode and those who had a history of recurrent episodes (N=4 of 18, 22.2%, versus N=19 of 79, 24.0%, respectively) (χ2=0.03, df=1, p=0.87, N=97). However, the results were limited because 81.4% (N=79) of those who were positive for a history of depression had recurrent depressive episodes.
Frequency of Depressive Symptoms and Related Impairment
Among the 43 individuals who met the criteria for major depressive episode on the basis of the Inventory to Diagnose Depression, five participants reported major depressive episodes at more than one assessment. For these participants, we used the first reported episode for the description of symptom frequency. Twenty-seven participants (62.8%) reported that their depressive episodes lasted for at least 1 month. All 43 participants reported depressed mood, and 27 (62.8%) reported loss of interest or pleasure. Twenty-one participants (48.8%) reported suicidal ideation for at least 2 weeks. Other depressive symptoms were frequently reported: poor concentration (N=40, 93.0%), insomnia or hypersomnia (N=37, 86.0%), fatigue (N=36, 83.7%), significant weight change (N=34, 79.1%), feelings of worthlessness (N=27, 62.8%), and psychomotor rigidity or agitation (N=24, 55.8%). The mean number of depressive symptoms reported was 6.72 (SD=1.32, range=5–9). Most participants (N=37, 86.0%) who experienced major depressive episodes reported a significant impact on their normal activities due to major depressive episodes. Eighteen participants (41.9%) reported seeking professional help for their posttreatment depression; 10 participants (23.3%) reported taking medication (both over-the-counter and prescribed), and one participant (2.3%) reported being hospitalized because of depression.
Predictors of Major Depressive Episodes After Treatment
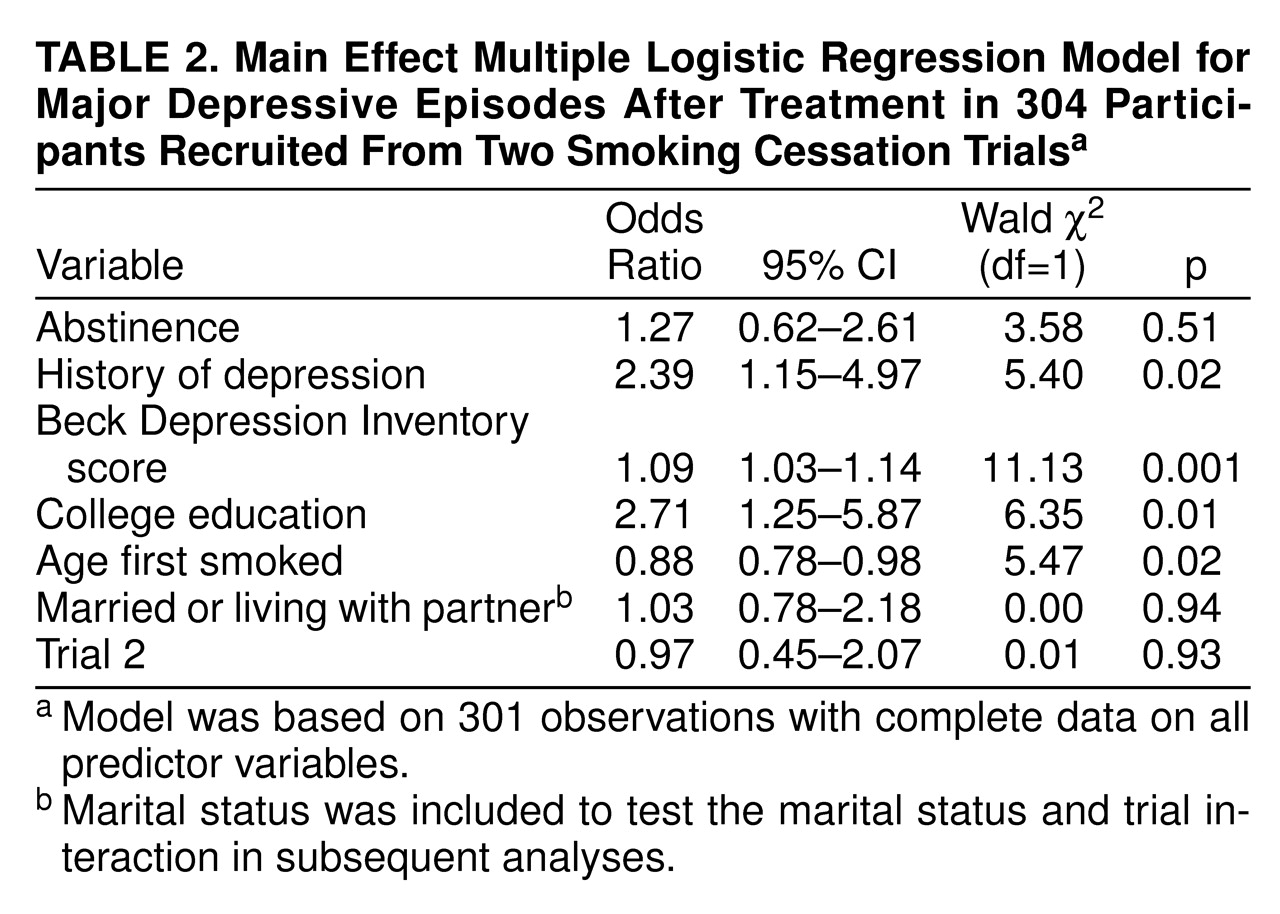
Significant predictors of the main effects model were the Beck Depression Inventory score, history of depression, college education, and age at smoking initiation (
table 2). The logits of the continuous scaled predictors (baseline Beck Depression Inventory score and age at smoking initiation) were found to have a linear association with the risk of major depressive episodes after treatment. The log likelihood of the main effects model was 107.52 (χ
2=31.78, df=7, p<0.001). The Hosmer and Lemeshow goodness-of-fit statistic
(31) was 6.77 (df=8, p=0.56), indicating an acceptable fit for the data.
The interaction between abstinence status and history of depression was not significant (χ
2=0.11, df=1, p=0.74). Three interaction terms were found to have potential significant contribution (p<0.15): depression history by marital status (χ
2=3.79, df=1, p=0.05), abstinence status by trial (χ
2=3.40, df=1, p=0.06), and marital status by trial (χ
2=3.98, df=1, p=0.05). The marital status and trial interaction was later removed from the final logistic regression because of a lack of significant contribution (p<0.05) to the model in the presence of other predictors and interaction terms (χ
2=3.15, df=1, p=0.08).
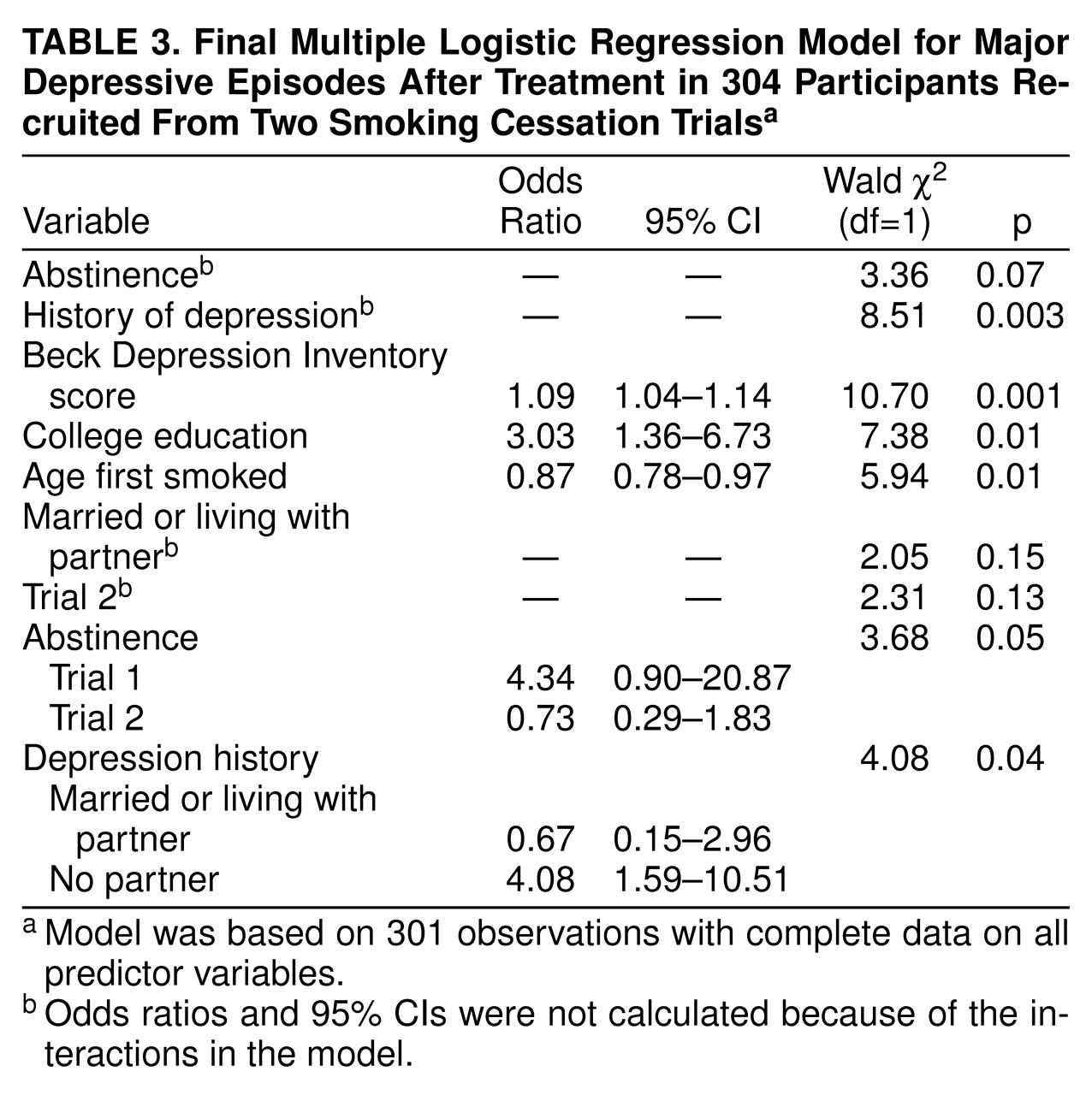
Table 3 shows the final logistic regression model, containing both main and interaction effects. The log likelihood of the final model was 103.29 (χ
2=40.31, df=9, p<0.001). The Hosmer and Lemeshow goodness-of-fit statistic
(31) was 3.25 (df=8, p=0.92), indicating that the logistic model for major depressive episodes after treatment fit the data adequately.
DISCUSSION
Contrary to our first hypothesis, abstinence status at the end of treatment did not increase the risk of major depressive episodes. Unexpectedly, a similar rate of incidence of major depressive episodes was observed among those who were not abstinent. The cause of these depressive episodes was not clear. On the basis of previous reports
(5,
21), it might be argued that reduction in smoking, as opposed to abstinence, precipitated major depressive episodes. However, reduction in cigarettes smoked at the end of treatment was not found to be associated with the incidence of major depressive episodes when tested instead of abstinence in logistic regression analyses. Psychological factors might precipitate major depressive episodes, such as the fear of relapse among participants who were abstinent
(14) or the experience of failure among those who were motivated to quit but were unsuccessful. However, these hypotheses could not be empirically tested by using the current data because these data were not collected.
The risk of major depressive episodes after treatment associated with abstinence was significantly higher in the trial with nicotine gum (trial 1) than in the trial with nortriptyline and placebo (trial 2), independent of whether the participants were taking active medication or placebo. The reason for the interaction of abstinence status and trial was not clear. The participants differed significantly on several variables, including nicotine dependence (Fagerstrom Tolerance Questionnaire score), age first smoked, depressed symptoms (Beck Depression Inventory score), and mood measures (total mood disturbance and trait anxiety scores). However, the direction of the differences was not consistent and was not logically related to the interaction.
Consistent with our second hypothesis, the risk of experiencing major depressive episodes was two times higher among smokers with a history of depression. Preliminary results showed that marital status might serve to moderate the effects of a history of depression. The risk of major depressive episodes after treatment in those who had a history of depression was four times higher among participants who had no partners, but the risk was similar among those who had partners. This finding should be interpreted with caution since the estimate was based on exploratory analyses and a small group of participants (N=23) who had a partner and a history of depression.
The incidence of major depressive episodes reported in the first 4 months after treatment (N=25, 8.5%; 95% CI=6.8%–10.0%) was similar to the 3-month incidence of major depressive episodes (N=9, 7.1%; 95% CI=2.8%–11.6%) reported in a previous study that used interview data from abstinent smokers
(15). (Calculations for the rate of incidence and confidence intervals were based on the total of 295 subjects who provided follow-up data during the first 4 months.) We observed a markedly high 12-month incidence of major depressive episodes after treatment compared to population estimates (1.6%–3.2%) of the 12-month incidence of major depressive disorders
(32–
34) and to an estimate of the first onset of major depressive episodes among young smokers (1.7%)
(35). Without a comparison group of smokers who did not attempt to abstain from smoking, it is unclear whether the elevated incidence of major depressive episodes in our group was related to the process of quitting, participants’ self-selection bias in seeking intensive treatment, assessment issues, or other factors.
The severity of baseline depression increased the risk of major depressive episodes after treatment by 9% with each 1-point increase in Beck Depression Inventory score. With other factors controlled, participants who were college educated were three times more likely than those who were less educated to develop major depressive episodes. The earlier one started smoking, the higher the risk that one might experience major depressive episodes. In particular, those who started smoking before age 15 (N=148, 48.7% of the group) were twice as likely to report major depressive episodes than those who started smoking later (odds ratio=2.21, 95% CI=1.05–4.62; Wald χ
2=4.41, df=1, p=0.04). (The odds ratio was estimated from the multiple logistic regression model by using the same predictors shown in
table 2). The presence of depression symptoms in adolescence predicted the duration of smoking in adulthood
(36) and the presence of nicotine dependence
(37). If some smokers rely mostly on smoking to cope with depression at an early age, they might be at a higher risk for severe depression when they attempt to quit smoking later in life. This was purely speculative, however, since there was no comparison group of participants who were not trying to quit smoking.
The use of cognitive behavioral mood management and nortriptyline for the treatment of smoking cessation was not related to the risk of major depressive episodes. The lack of association between the risks of major depressive episodes and the psychological treatment conditions might be explained by the intervention’s focus on teaching mood management skills related to smoking cessation rather than on preventing major depression itself. The observed lack of association between nortriptyline administration and the recurrence of major depressive episodes should be viewed as preliminary evidence. Treatment guidelines have recommended at least 4–9 months of antidepressant treatment for the prevention of the recurrence of major depressive episodes
(38). However, because the primary focus of the original design was on the acute effects of antidepressant medication on smoking cessation, participants in the current study received only 11 weeks of nortriptyline treatment. The follow-up assessments of major depressive episodes took place when the subjects were no longer receiving medication. These factors might account for the lack of difference in the risk of major depressive episodes between the medication and placebo groups.
Limitations
These findings should be interpreted taking the following limitations into account. First, the incidence estimate in this study was based on self-report questionnaire data. Second, this study lacked a comparison group of smokers who did not attempt to quit smoking. Third, no detailed data were available on the onset of major depressive episodes in relation to quit dates or to precipitating events such as psychological and situational stress. Furthermore, the results were confined to smokers who sought intensive treatment for smoking cessation and who tended to be more nicotine dependent.