From May 1993 to April 1994, 211 patients were referred for study. After complete description of the study to the subjects, written informed consent was obtained. We excluded 111 patients because 1) their fatigue had lasted less than half of the time during the previous 6 months (N=51), 2) organic causes were found (N=14), 3) there was concurrent antidepressant treatment by psychiatrists (N=5), 4) pregnancy (N=1), or 5) they did not give consent (N=40).
Demographic Data and DSM-III-R Diagnoses
The 100 patients included in the study (25 men and 75 women) were all Chinese residents of Hong Kong. Their mean age was 40.8 years (SD=8.8, range=18–63). Seventy-nine percent were married, 10% single, 6% widowed, and 5% divorced. The five general categories of occupation were housewife (31%), laborer (27%), clerical (20%), professional (19%), and student (3%). Their mean number of years of education was 7.9 (SD=3.7, range=1–17). Most patients were from the lower social class. Monthly family income in Hong Kong dollars ($1.00 in U.S. currency=$7.80 in Hong Kong currency) was as follows: $5,000–$10,000 (38%), $10,000–$20,000 (41%), $20,000–$30,000 (11%), greater than $30,000 (10%).
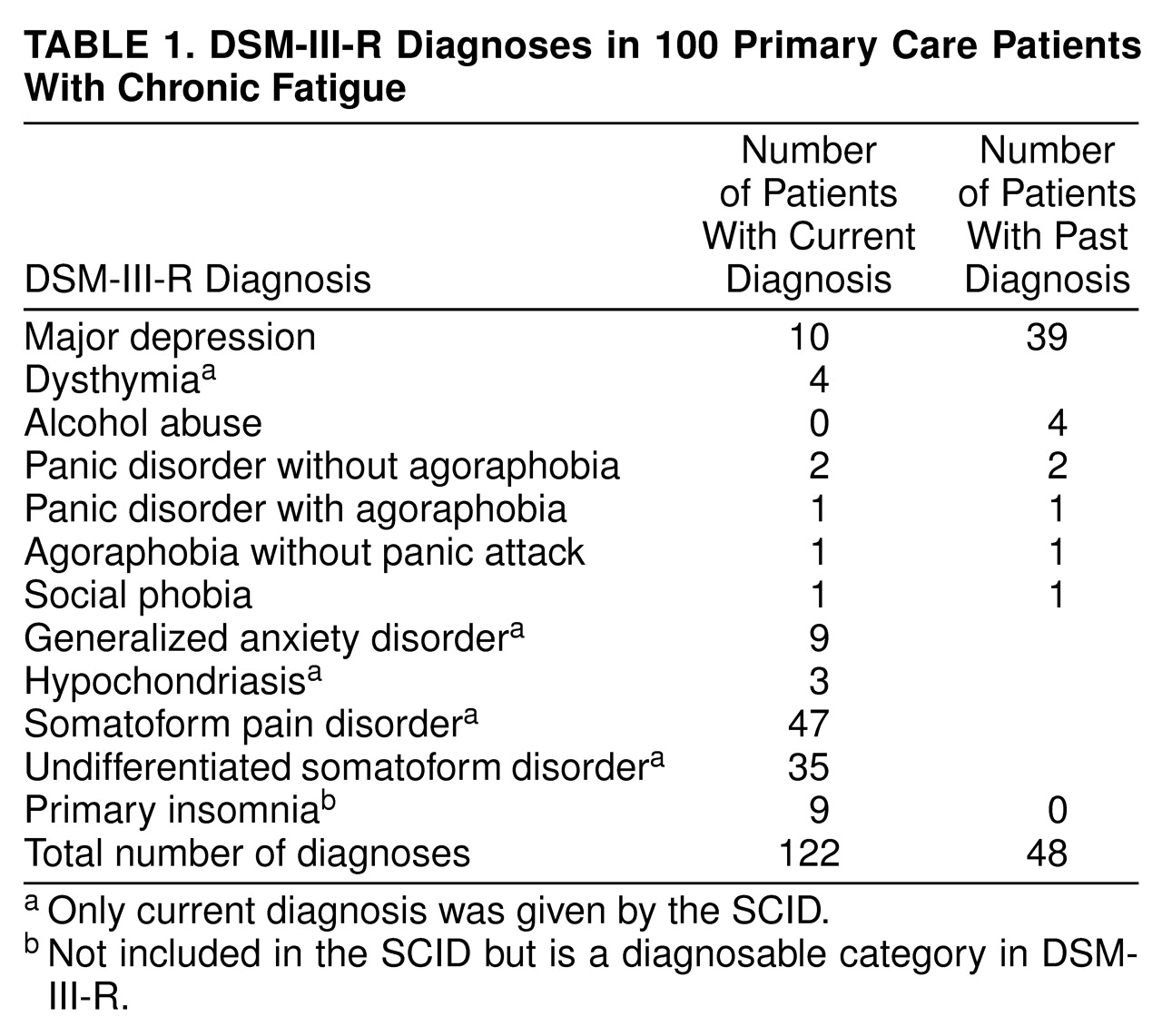
Patients had a mean of 1.22 current diagnoses (
table 1). The most common diagnoses were somatoform pain disorder and undifferentiated somatoform disorder. Ten patients had major depression. The other current diagnoses included generalized anxiety disorder, dysthymia, panic disorder, hypochondriasis, social phobia, and agoraphobia. Nine patients could not be diagnosed as having undifferentiated somatoform disorder because their somatic symptoms were secondary to insomnia. They could be diagnosed only as having primary insomnia according to DSM-III-R. If comorbidity was not counted, the current diagnoses were major depression (N=10), dysthymia (N=4), panic disorder (N=2), agoraphobia (N=1), generalized anxiety disorder (N=9), hypochondriasis (N=2), somatoform pain disorder (N=33), undifferentiated somatoform disorder (N=30), and primary insomnia (N=9).
After somatoform pain disorder, undifferentiated somatoform disorder, and primary insomnia were excluded, the lifetime prevalence of depressive and anxiety disorders was 54%, with major depression being the most frequent (40%).
Weakness of Nerves, Neurasthenia, and Chronic Fatigue Syndrome
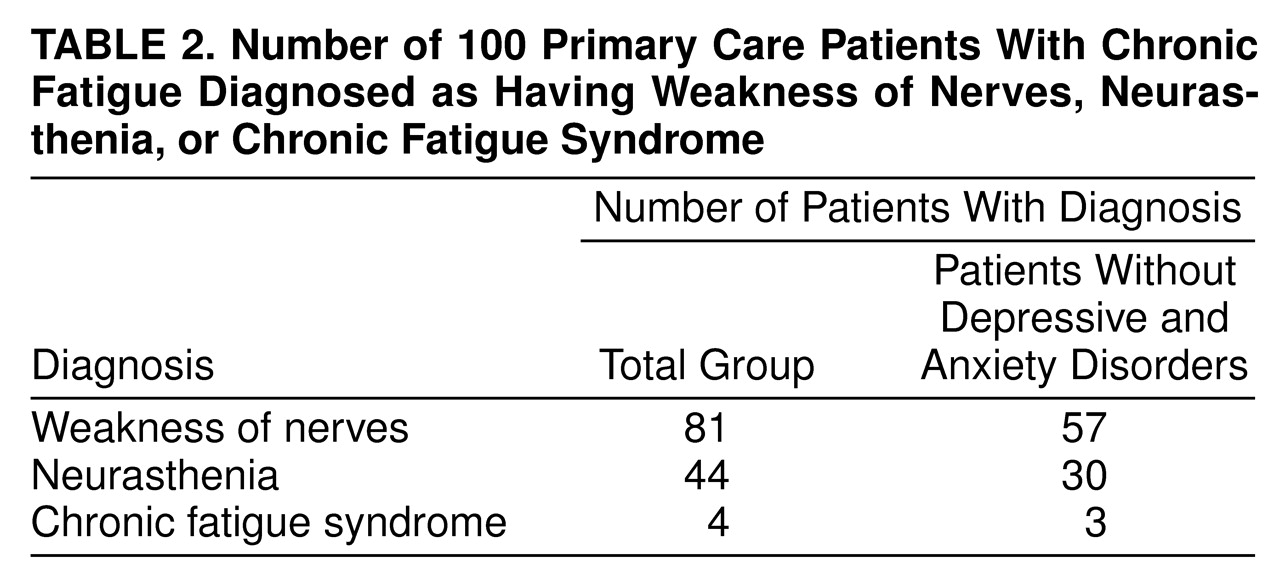
Fifty-seven patients met the criteria for weakness of nerves, and 30 patients met the criteria for neurasthenia (
table 2). These numbers rose to 81 and 44 if exclusion criteria for depressive and anxiety disorders were not applied. As for chronic fatigue syndrome, 55 patients did not fulfill the core symptom criteria, which require that fatigue reduced daily activity by over 50% and did not resolve with bedrest. Forty-one patients did not have physical signs. Only four patients, because of the presence of mild fever, sore throat, or painful lymph nodes, fulfilled the CDC symptom criteria. After one patient with current major depression was excluded, three satisfied the complete CDC criteria. Their mean Hamilton anxiety scale (12.3) and Hamilton depression scale (7.3) scores were low.
The mean Hamilton depression scale score for all of the patients was 9.8 (SD=5.9, range=2–37) (possible range=0–96). The mean score for the 10 patients with current major depression was 22.7 (SD=6.9, range=15–37). The mean Hamilton anxiety scale score for all of the patients was 12.7 (SD=4.6, range=3–28) (possible range=0–56). The most frequently reported Hamilton depression scale items were general somatic symptoms, anxiety, and insomnia, and the most commonly reported Hamilton anxiety scale items were tension, insomnia, and autonomic symptoms. The mean SCL-90-R score (82.8, SD=53.9, range=13–233) (full range=0–360) of the 100 patients was significantly higher than that of a local community sample of 1,471 subjects without mental disorders (59.9, SD=52.9) (t=4.17, df=1569, p<0.0001) (unpublished paper by Lee and Leung). All subscale scores of the 100 patients were also significantly higher than those of community subjects (p<0.0001 after Bonferroni correction). Somatization was positively correlated with depression (r=0.69), anxiety (r=0.75), hostility (r=0.63), and phobia (r=0.55) (N=100, p<0.001).
Headache (21%), insomnia (20%), worries (20%), and other pains (12%) were the most common unprompted complaints. Only five patients spontaneously complained of fatigue. The other unprompted complaints included irritability (3%), indigestion (3%), unhappiness (2%), dizziness (2%), fright (1%), flu (1%), and hypertension (1%).
In descending order, the most troubling complaints were pains (20%), insomnia (20%), headache (16%), worries (13%), fatigue (11%), unhappiness (5%), somatic discomfort (4%), dizziness (3%), irritability (3%), loss of drive (2%), weakness (1%), poor memory (1%), and suspicion of ill health (1%).
Thirty-one patients were unable to name their illness. Twenty spontaneously called it weakness of nerves. Other names reflected the diversity of patients’ illness experience, including nervousness (10%), headache/pain/migraine (8%), rheumatism (5%), fatigue/fatigue illness (5%), insomnia (5%), urban illness (3%), occupational illness (3%), unchangeable illness (2%), unhappiness (1%), stress (1%), hotness (1%), kidney illness (1%), aging (1%), fright (1%), longing for son (1%), and weakness (1%). When patients were specifically asked whether they had weakness of nerves, 72% answered in the affirmative. Nobody had heard of chronic fatigue syndrome before.
According to the etiological categories in the Explanatory Model Interview Catalogue, over half of the patients identified psychosocial factors as the main cause of their problems. The more common causes were mind problem/worry (18%), marital problem (9%), problems at work (9%), physical problem (8%), stress/loss (8%), weakness (7%), overwork (4%), personality (4%), and injury/surgery (4%). The rest included other physical or constitutional causes. Only one patient referred to immune dysfunction, and only two patients referred to infection.
Differences Between Subgroups
Twenty-eight patients with current depressive and anxiety disorders were merged as one group. The other 72 patients were classified as another group. These two groups exhibited no significant difference in sociodemographic characteristics. The group with current depressive and anxiety disorders scored significantly higher on the Hamilton depression scale (mean=15.86, SD=7.33, versus mean=7.42, SD=2.76) (t=5.94, df=30, p<0.0001), Hamilton anxiety scale (mean=17.21, SD=4.79, versus mean=10.89, SD=3.09) (t=7.80, df=98, p<0.0001), SCL-90-R (mean=120.5, SD=57.6, versus mean=68.2, SD=44.8) (t=4.83, df=98, p<0.001), and all SCL-90-R subscales than the other group. Fatigue had a similar duration in the two groups (mean=8.0 years, SD=6.3, versus mean=7.9 years, SD=6.3) but was significantly more likely to reduce daily activities by 50% or more in the group with current depressive and anxiety disorders (64.3% versus 37.5%) (χ2=5.84, df=1, p<0.05). There was no significant difference in the two groups’ illness experience in regard to unprompted complaints, most troublesome complaint, or attributional style.
Patients’ fatigue had a mean duration of 7.9 years (SD=6.2, median=6, range=0.5–30). Forty-five patients reported that their fatigue was severe enough to reduce their average daily activity by 50% or more. More of these patients with severe fatigue than patients with milder fatigue received current diagnoses of depressive and anxiety disorders (N=18 [40.0%] versus N=10 [18.2%]), and fewer received current diagnoses of somatoform pain disorder/undifferentiated somatoform disorder (N=27 [60.0%] versus N=45 [81.8%]) (χ2=5.84, df=1, p<0.05). The scores of the more severely fatigued patients on the Hamilton depression scale (mean=11.2, SD=6.5, versus mean=8.7, SD=5.2) (t=–2.15, df=98, p<0.05) and Hamilton anxiety scale (mean=13.9, SD=4.5, versus mean=11.6, SD=4.5) (t=–2.52, df=98, p<0.05) were higher than those of the less fatigued patients, but the difference was not of clinical significance.