Glycogen synthase kinase-3 (GSK-3) is a highly conserved serine/threonine protein kinase that is involved in the signal transduction cascade of multiple cellular processes. GSK-3 is a juncture of at least three signal transduction cascades—the mitogen-activated protein kinase cascade
(1), the phosphatidylinositol 3-kinase cascade
(2), and the Wnt cascade, which plays a role in modulation of cell fate during development
(3). Recently, GSK-3β has been identified as a potent kinase highly abundant in brain tissue
(4) that apparently regulates diverse brain proteins, including microtubules
(5), myelin basic protein
(6), nerve growth factor
(7), and neurofilaments
(8). GSK-3β is also a potent tau kinase capable of phosphorylating tau on sites that are abnormally phosphorylated in Alzheimer’s disease brain and responsible for reducing microtubule binding involved in neuronal degradation
(9). Lithium has been found to be an inhibitor of GSK-3β, with an inhibition constant within the therapeutic concentration range
(10,
11). We were therefore interested in the possibility that GSK-3β might be elevated in patients with bipolar disorder. Because of theories that posit schizophrenia as a disorder of neurodevelopment
(12), we were also intrigued by the possibility that GSK-3β levels might be abnormal in this disease.
Method
Frozen postmortem brain samples of frontal cortex (Brodmann’s area 10) were obtained from the Stanley Foundation Brain Bank. The 58 samples were taken from 14 schizophrenic patients, 15 patients with bipolar disorder, 15 with unipolar depression, and 14 normal comparison subjects. None of the comparison subjects had had a history of psychiatric disorder or had received antipsychotic medication, nor did any die as a result of suicide or a neurological disorder. The four groups were matched for age, sex, race, postmortem interval, and side of brain. The 14 schizophrenic patients (eight men and six women) were a mean age of 44.2 years (range=25–62), with a mean postmortem interval of 33.7 hours (range=12–61); 12 of these subjects were white, two were Asian. The 15 patients with bipolar disorder (nine men and six women) were a mean age of 42.3 years (range=25–61), with a mean postmortem interval of 32.5 hours (range=13–62); 14 of these subjects were white, one was black. The 15 patients with unipolar depression (nine men and six women) were a mean age of 46.5 years (range=30–65), with a mean postmortem interval of 27.5 hours (range=7–47); all were white. Finally, the 14 normal comparison subjects (eight men and six women) were a mean age of 48.1 years (range=29–68), with a mean postmortem interval of 23.7 hours (range=8–42); 13 of these subjects were white, one was black. The investigator who carried out the assays (N.K.) was blind to diagnosis and received specimens in a balanced way so that each run included matched samples, one from each of the four diagnostic groups. The study was approved by our hospital’s institutional review board.
We assessed postmortem stability of GSK-3β immunoreactivity by assessing GSK-3β in rat brain. Rats were sacrificed and left at room temperature for 0, 0.5, 2, 4, 8, 16, 24 and 48 hours (two rats per each time point, each assayed at least three times). Frontal cortex tissue was then frozen at –70˚C until assayed for GSK-3β immunoreactivity.
Sodium dodecyl sulfate/polyacrylamide gel electrophoretic separation and immunoblotting of GSK-3β were performed by means of a previously described procedure
(13) with modifications. Briefly, samples (25–50 mg) of postmortem frontal cortex were sonicated for 10 seconds in 50% power capacity (Heat Systems Ultrasonic Inc.), and 0.1% (vol/vol) nonident P-40 was added. The cell lysate was diluted to 1 mg total protein/ml, and aliquots were stored at –20˚C until assayed. Aliquots of 9 and 18 ml (0.3 and 0.6 mg total protein) were separated, blotted, and probed for 16–18 hours at 4˚C with diluted (1:6000) anti-GSK-3β antibodies (Transduction Laboratories, Lexington, Ky.). Bands were detected with Chemiluminescence Western blot detection kit (Amersham, Oakville, Ont.). Densities of the immunoreactive bands were quantified using AIDA-2D image analysis system (Dinco and Rhenium Marketing, Jerusalem).
To minimize the effect of interblot variability, a calibration standard curve of known amounts of recombinant GSK-3β units (Upstate Biotechnology, Lake Placid, N.Y.) was run in each gel. The correlation coefficient of the standard curves was always higher than 0.9. Furthermore, each sample was analyzed at least three times and at two different protein concentrations, both within the linear range of detection. Thus, the absolute GSK-3β values (in units) of each band were derived from the standard curve run on the same gel. The mean value for each sample was calculated from all of the replicates. Statistical analyses of the data were preformed by the software STATISTICA for Windows.
Results
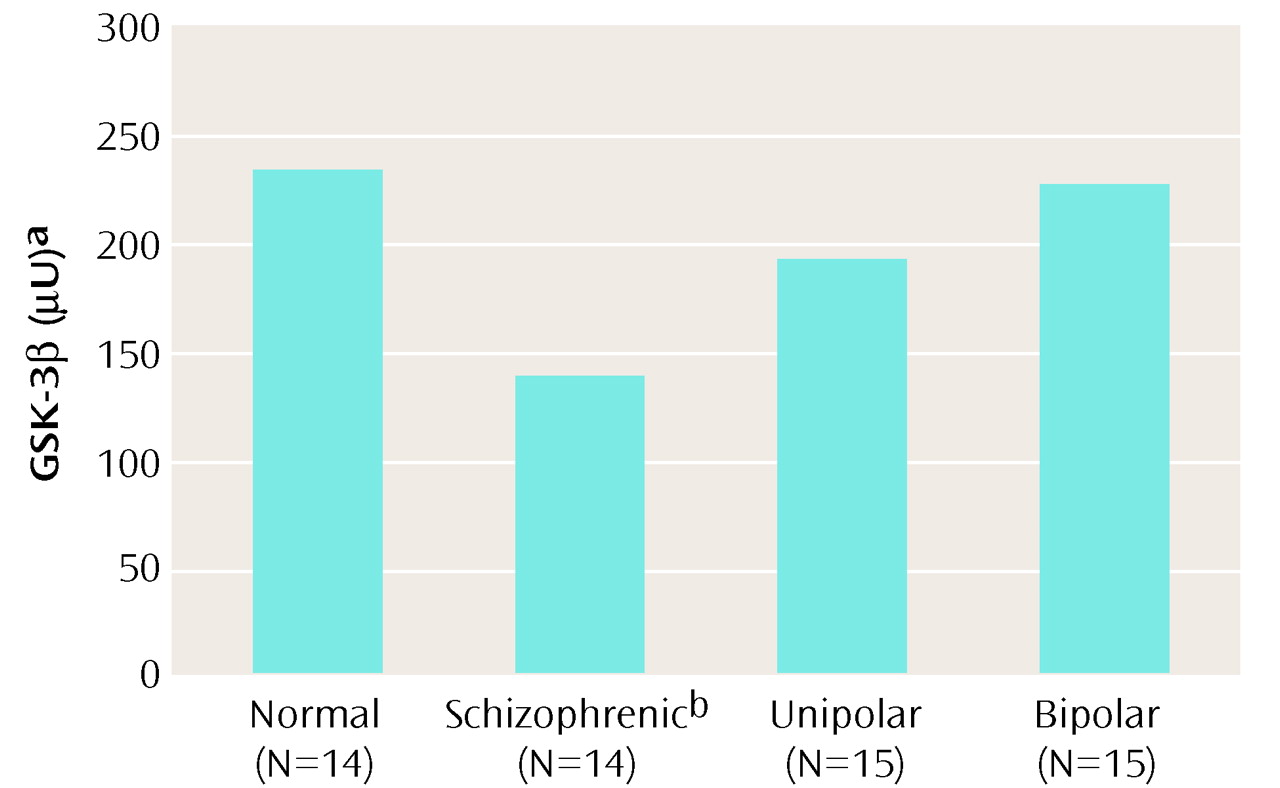
A single immunoreactive band of GSK-3β in the human brain frontal cortex (46 kDa) was confirmed. As seen in
Figure 1, the schizophrenic patients had GSK-3β levels that were 41% lower than those of normal subjects (analysis of variance [ANOVA] F=3.09, df=3, 54, p=0.03; post hoc least significant difference, p=0.008).
There was no correlation between GSK-3β and age (r=0.11, df=56, n.s.) or postmortem interval (r=0.0002, df=56, n.s.). One-way ANOVA for the eight time points from 0 to 48 hours showed that postmortem interval did not have a significant effect on rat prefrontal cortex GSK-3β levels (F=1.2, df=7, 42, p=0.32). Values at 48 hours were 19% lower than those at time zero (post hoc least significant difference, p=0.44). There was no correlation between GSK-3β levels in the schizophrenic patients and their estimated lifetime antipsychotic consumption in chlorpromazine equivalents. Two-way ANOVAs revealed GSK-3β levels in the frontal cortex were lower in female than in male subjects (for diagnosis: F=3.37, df=3, 50, p=0.03; for sex: F=4.24, df=1, 50, p=0.04; for diagnosis-by-sex interaction: F=0.80, df=3, 50, p=0.50).
Discussion
The lower levels of GSK-3β found in our study seem specific for the patients with schizophrenia, since no changes were found in the levels of GSK-3β in patients with bipolar disorder or unipolar depression. In view of the fact that lithium inhibits GSK-3β
(10,
11), it may seem surprising that GSK-3β is not altered in patients with bipolar disorder; however, the site of psychopharmacologic action of lithium is not necessarily the site of etiology for bipolar illness. The present study, supported by the previous lymphocyte findings of Yang et al.
(14) and the recent report of Miyaoka et al.
(15) of increased expression of Wnt-1 in the hippocampus of schizophrenic patients, suggest that alterations of neurodevelopment-linked proteins are markers of schizophrenia.
One of the multiple substrates of GSK-3, b-catenin, mediates signal transduction effects of this enzyme, particularly within the Wnt signaling cascade
(3). By binding with cadherins b-catenin regulates cell adhesion and affects intracellular junctions such as synapses
(16). Cotter et al.
(17) recently found reduced immunohistochemically stained intraneuronal b- and g-catenin in the hippocampal subregions CA3 and CA4 of schizophrenic subjects. Indeed, schizophrenia has been shown to involve developmental brain changes reflected by abnormal neuronal lamination and synaptic organization
(17,
18). Marker proteins that correlate with neurodevelopmental pathology have been reported in schizophrenia, e.g., lower mRNA levels of synaptophysin
(19) and higher levels of growth-associated protein GAP-43
(20). Aberrant signal transduction as an underlying mechanism of schizophrenia has also been previously postulated
(21).
The constitutively active form of GSK-3β is phosphorylated at the 216-tyrosine residue, while the inactivated form is phosphorylated at serine-9 residue
(22). The anti-GSK-3β antibodies used in the present study do not discriminate between the active and the inactive forms; therefore, only total enzyme protein levels are quantitated.
The factors regulating total GSK-3 levels in the brain and other tissues are not known. Reduced total GSK-3β protein levels cannot be directly interpreted in terms of downstream effects, since the active fraction of the enzyme is the relevant one for such consideration. Therefore, it remains to be investigated whether the active fraction of GSK-3β, or its activity, is also low in frontal cortex of schizophrenic patients, and if this is also reflected in other brain regions.