Although binge eating disorder has no established treatment
(1), selective serotonin reuptake inhibitors (SSRIs) hold promise because they are effective in the treatment of bulimia nervosa
(2,
3), a related condition. In a previous study
(4), we found fluvoxamine to be superior to placebo in the treatment of binge eating disorder. Because of these observations, we conducted a placebo-controlled study of the SSRI sertraline in the treatment of binge eating disorder.
Method
The subjects were outpatients meeting DSM-IV criteria for binge eating disorder who also had experienced at least three binge eating episodes weekly for at least 6 months. We defined a binge according to DSM-IV criteria plus requiring the estimated number of calories to be at least 1500 kcal. The patients were between 18 and 60 years of age and had to weigh more than 85% of their ideal body weight
(4). We excluded individuals who, on the basis of structured interview
(5), had current anorexia nervosa, substance use disorder within the past 6 months, or history of psychosis or mania; risk of suicide; use of psychotropics within 2 weeks of random assignment to treatment or placebo groups; previous use of sertraline; or fewer than three binges in the week before random assignment to groups.
After a week of single-blind placebo administration, we assigned patients randomly to 6 weeks of double-blind treatment with sertraline or placebo. Study materials were capsules containing either 50 mg of sertraline or placebo. Subjects took one capsule daily for at least 3 days; thereafter the dose could be adjusted to between one and four capsules daily.
At each weekly visit, we assessed the number of binges since the last visit (using diaries); Clinical Global Impression (CGI) severity and improvement ratings; medication dose; and weight. We administered the 24-item Hamilton Depression Rating Scale at baseline and weeks 2, 4, and 6. We categorized responses at week 6 on the basis of percentage of decrease in frequency of binges from baseline: remission=cessation of binges; marked=75%–99% decrease; moderate=50%–74% decrease; and none=less than 50% decrease.
For each outcome (except response category), we performed repeated measures random regression analyses
(6,
7) comparing rate of change of outcome in the sertraline group and the placebo group (see reference
4). This was an intent-to-treat analysis because it included observations from all subjects (including dropouts) at all time points. To analyze frequency of binges, we used logarithmic transformation (log [(binges/week) + 1]) to stabilize variance. We compared differences in response categories using the exact trend test for two-by-k-ordered tables
(6–
8).
The institutional review board at the University of Cincinnati approved the protocol. All subjects signed informed consent forms after study procedures had been fully explained. Forty-five subjects entered the study; 34 were randomly assigned to active drug or placebo groups.
Results
Eighteen patients received sertraline, and 16 received placebo. There were no significant differences between groups at baseline in age, sex, body mass index, number of binges/week, Hamilton depression scale score, lifetime major depressive disorder, or current major depressive disorder. The mean age of the patients given sertraline was 43.1 years (SD=9.9), and the mean age of those given placebo was 41.0 (SD=12.2) (t=0.55, df=32, p=0.58). Sixteen (89%) of the patients given sertraline and all of the placebo patients were women (p=0.49, Fisher’s exact test). The mean body mass index of the sertraline group was 36.4 (SD=7.4), compared with 35.8 (SD=7.5) for the placebo group (t=0.23, df=32, p=0.82). The mean number of binges/week and its logarithmic transformation for the sertraline group were 7.6 (SD=4.8) and 2.04 (SD=0.48), respectively, compared with 7.2 (SD=5.8) and 1.97 (SD=0.52) for the placebo group (t=0.22, df=32, p=0.83, and t=0.40, df=32, p=0.69, respectively). The mean Hamilton depression scale score of the sertraline group was 6.4 (SD=3.9), compared with 7.5 (SD=8.4) for the placebo group (t=–0.50, df=32, p=0.62). Eleven (61%) of the patients given sertraline and seven (44%) of those given placebo had a lifetime diagnosis of major depressive disorder (p=0.30, Fisher’s exact test). Three (17%) of the sertraline patients and three (19%) of the placebo patients had a current diagnosis of major depressive disorder (p=1.00, Fisher’s exact test).
Eight patients withdrew during the study, all before the end of 4 weeks, for the following reasons: three for failure to make follow-up appointments; two for refusal to discontinue disallowed medications; one for refusal to obtain evaluation of a medical condition, one for a death in the family, and one for finding the study requirements burdensome. No patient withdrew because of an adverse medical event or worsening psychiatric status. The remaining 26 patients (13 in each group) completed the study. There were no significant differences between groups in incidence of adverse events, except that more sertraline-treated patients (N=7 [39%]) than patients given placebo (N=1 [6%] experienced insomnia (p=0.04, Fisher’s exact test).
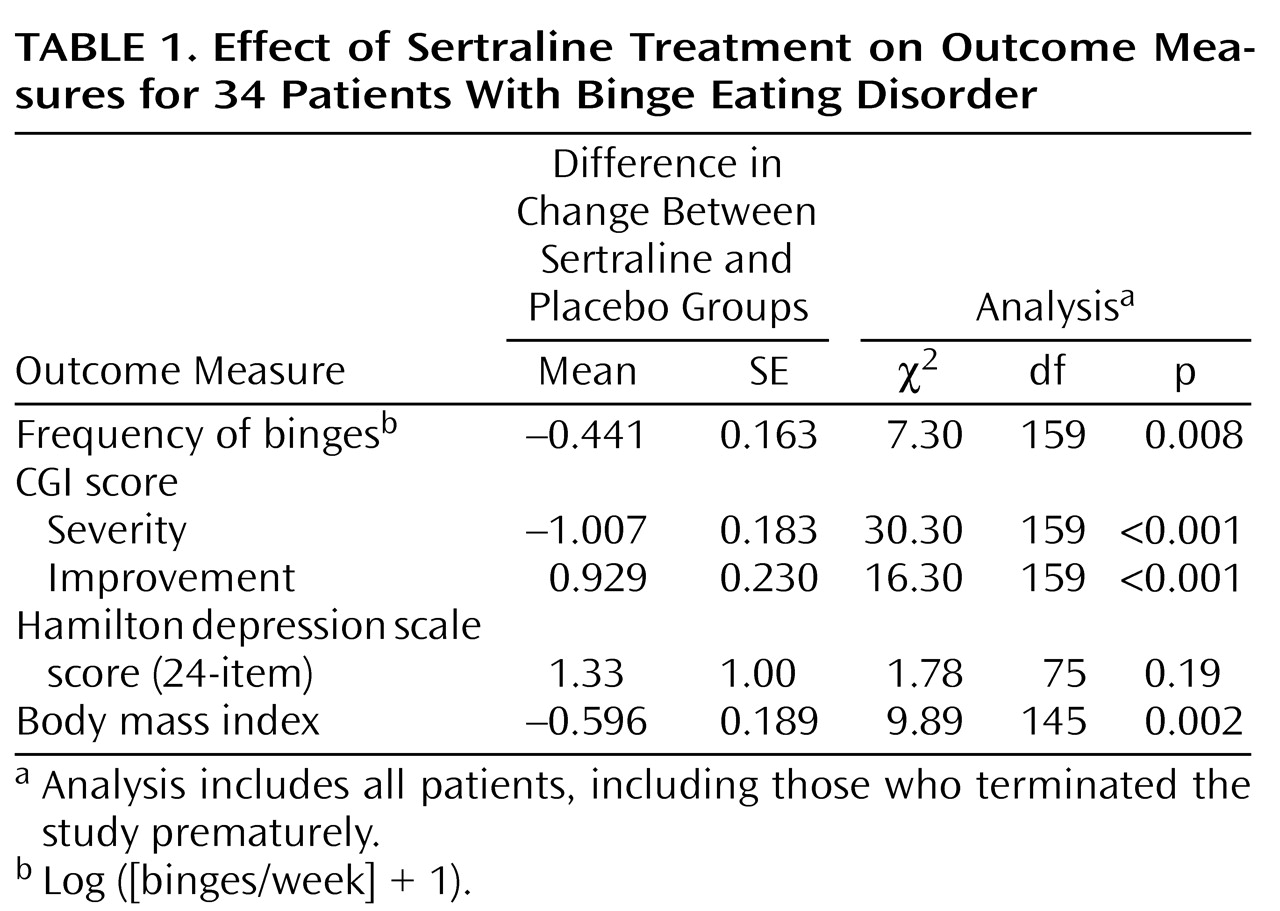
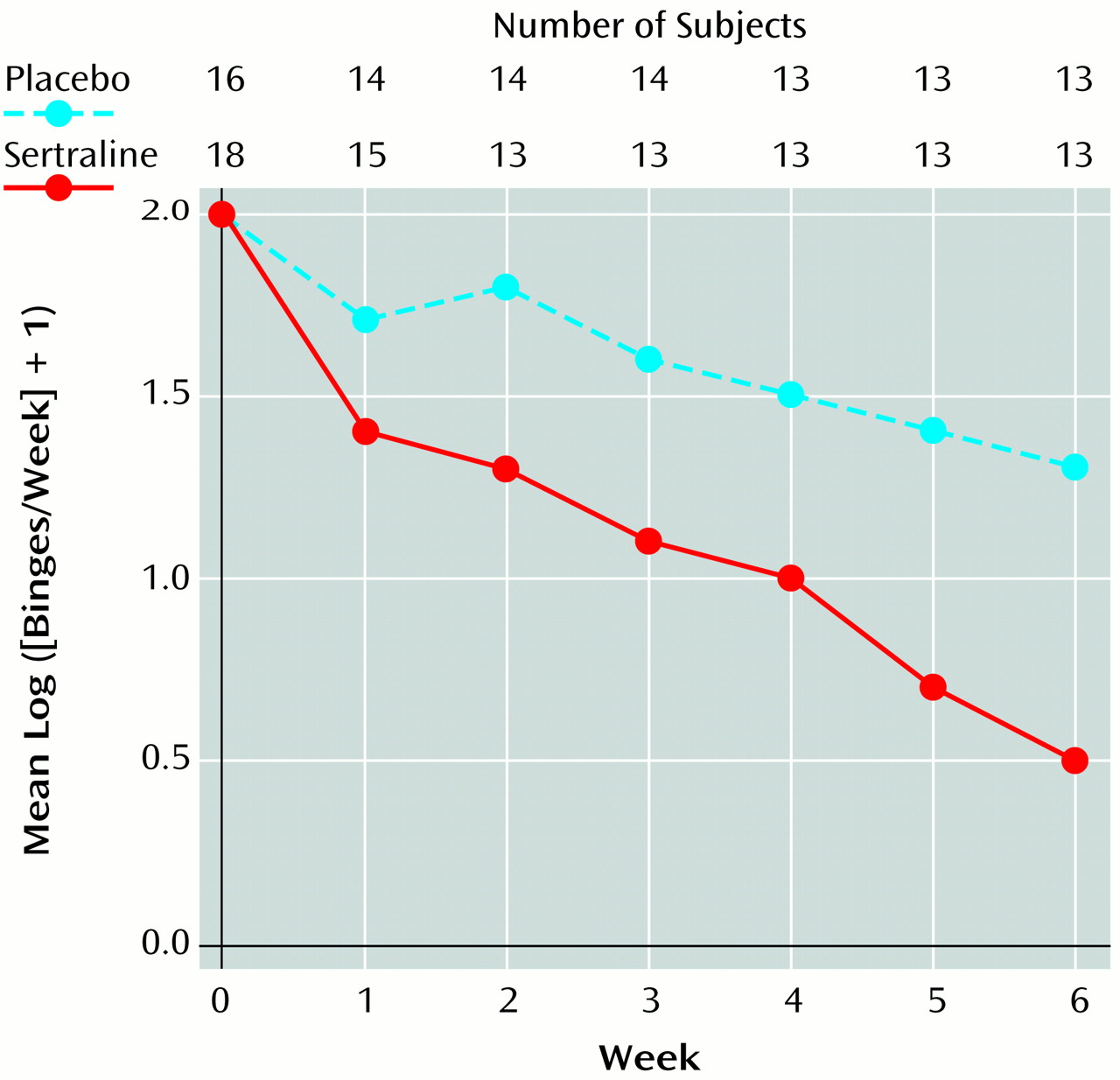
Over the course of treatment, the frequency of binges decreased in both groups, but more so in the sertraline group (
Figure 1). Rates of decrease in the frequency of binges, improvement in CGI scores, and decrease in body mass index were significantly greater in the sertraline group than in the placebo group (
Table 1). Estimated mean weight loss after 6 weeks of treatment for a patient 65.2 inches tall (the mean height for all patients) was 12.3 lb on sertraline, compared with 5.3 lb on placebo. Differences between groups remained significant even when the six patients with current major depressive disorder were excluded from the analysis. Among the patients who completed the study, sertraline was associated with a higher response level than placebo (seven versus two reached remission; two versus three had a marked response; three versus four had a moderate response; and none versus four had no response), but the difference did not reach statistical significance (p=0.06, exact trend test). At week 6, the mean number of binges/week was 1.13 (SD=1.56) in the sertraline group and 3.85 (SD=3.81) in the placebo group, and the mean log ([binges/week] + 1) was 0.54 (SD=0.66) in the sertraline group and 1.30 (SD=0.80) in the placebo group. The mean medication dose in the sertraline group was 187 mg (SD=30).