Latent Class Analysis
After fitting a single-class model, the addition of further classes resulted in significant improvements in fit up through six classes. Neither the seven-class nor the eight-class solution significantly improved the fit. Individual participants were assigned to class membership on the basis of the likelihood of their response profile.
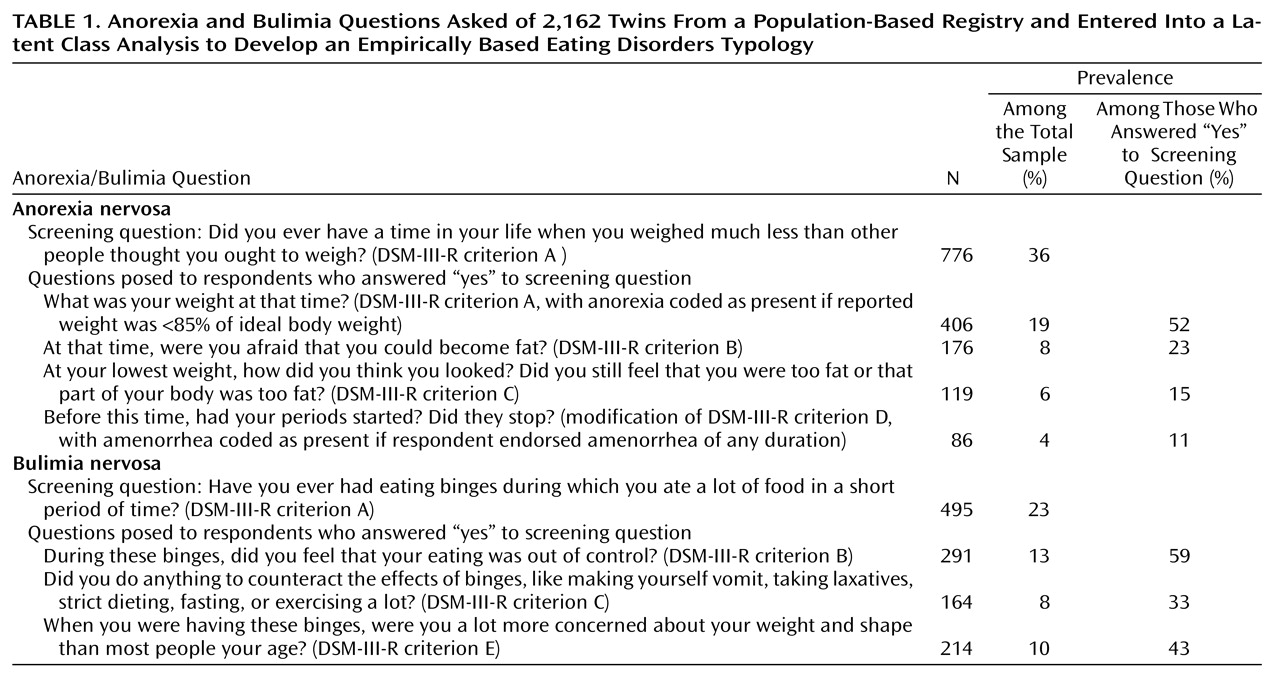
Of the total sample, 1,071 women responded positively to at least one of the eating disorders screening questions.
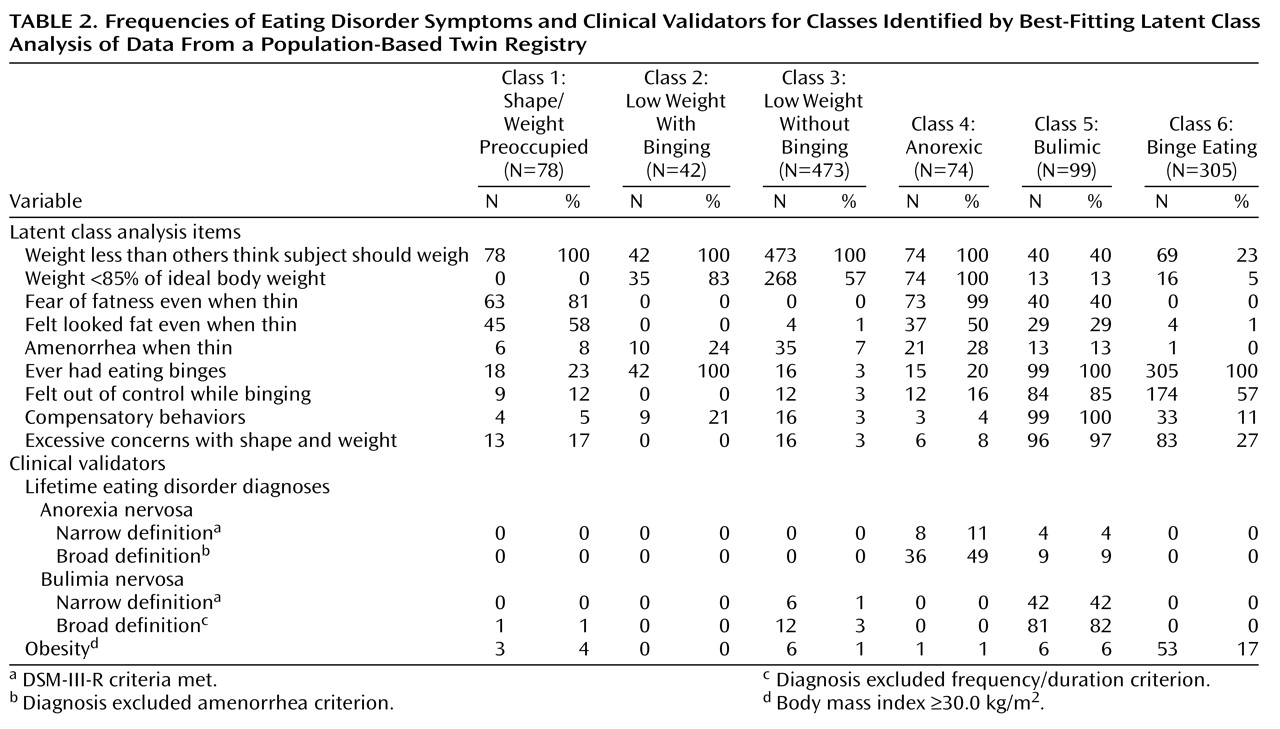
Table 2 depicts the frequency of the nine DSM-III-R eating disorder symptoms for the six classes identified by the best-fitting latent class analysis solution as well as the eating- and weight-related validators. On the basis of these characteristics, we developed the following descriptions of the six classes.
In class 1 (3.6% of the sample; mean age=29.4 years, SD=7.4), all of the women reported weighing less than other people thought they should have weighed. However, none had actually ever been <85% of their ideal body weight. Despite this, fear of fatness and body image distortion were frequently endorsed. Secondary amenorrhea was present in a small percentage. Approximately one-quarter of these women endorsed binge eating; however, feeling out of control and excessive concerns with shape and weight were uncommon, and compensatory behaviors were relatively rare. A lifetime history of anorexia or bulimia, no matter how defined, was extremely rare in members of this class. Obesity (defined as having a body mass index of 30 kg/m2 or more) was also uncommon. On the basis of these characteristics, this class was referred to as “shape/weight preoccupied.”
In class 2 (1.9% of the sample; mean age=29.4 years, SD=6.8), all members reported having weighed less than others thought they should have weighed, and most actually had been <85% of their ideal body weight. None of the women in this class endorsed the psychological features of anorexia nervosa, although approximately one-quarter reported amenorrhea when thin. Although all of the women in class 2 reported having binged, none ever had felt out of control, and all denied having excessive shape and weight concerns. Compensatory behaviors occurred in 21% of this class. None of the women met diagnostic criteria for any definition of anorexia or bulimia, and no one in this class was obese. We called this group the “low weight with binging” class.
In class 3 (21.9% of the sample; mean age=31.6 years, SD=7.8), all members reported weighing less than others thought they should have weighed, and slightly over half had actually weighed <85% of their ideal body weight. The psychological features of anorexia were mostly absent, and amenorrhea was uncommon. Episodes of binge eating and compensatory behaviors were also rare in this class. Anorexia nervosa did not occur in this class, and obesity and a lifetime diagnosis of bulimia nervosa, narrow or broad definition, were rare. This group was the “low weight without binging” class.
In class 4 (3.4% of the sample; mean age=28.1 years, SD=6.1), all of the women said they had weighed less than others thought they should have weighed, and all reported weights that were <85% of their ideal body weight. Fear of fatness was nearly ubiquitous; one-half felt they looked fat even when thin, and secondary amenorrhea was present in over one-quarter of the women. Episodes of binge eating were reported by one-fifth of the women in this class, but purging was infrequent. Approximately half of the women in this class met criteria for the broad definition of anorexia nervosa, while 11% met the narrow anorexia definition. Lifetime bulimia nervosa was absent in this class, and obesity was rare. This group was the “anorexic” class.
In class 5 (4.6% of the sample; mean age=28.4 years, SD=6.8), although many of the women reported having weighed less than others thought they should weigh, few reported weights <85% of their ideal body weight. The psychological features of anorexia nervosa were common, and secondary amenorrhea was reported occasionally. Binge eating, compensatory behaviors, and excessive concern with shape and weight were nearly universal, and the majority reported feeling out of control while binging. Nine percent of women in this class met lifetime criteria for the broad definition of anorexia nervosa, while a substantial majority met criteria for the broad definition of bulimia nervosa. Obesity was reported by 6%. We called this group the “bulimic” class.
In class 6 (14.1% of the sample; mean age=29.7 years, SD=7.6), nearly one-quarter of the women reported having weighed less than others thought they should have weighed, but very few had actually been <85% of their ideal body weight. The psychological features of anorexia nervosa and amenorrhea were rarely endorsed. In contrast, all of these women reported episodes of binge eating, with over one-half reporting having felt out of control. Purging was rarely endorsed, and excessive concerns with shape and weight were also uncommon. None of the women in this class met criteria for either definition of anorexia or bulimia. Obesity was markedly more common in this class than in any other. We called this group the “binge-eating” class.
Classes 4, 5, and 6 were referred to as “eating disorder classes,” since they represented more severe clusters of disordered eating.
Validators
Demographic
There were no significant differences across the six classes and the comparison group on education, parental education, financial status, or size of community in which the individual lived.
Lifetime prevalence of other psychiatric and psychoactive substance use disorders
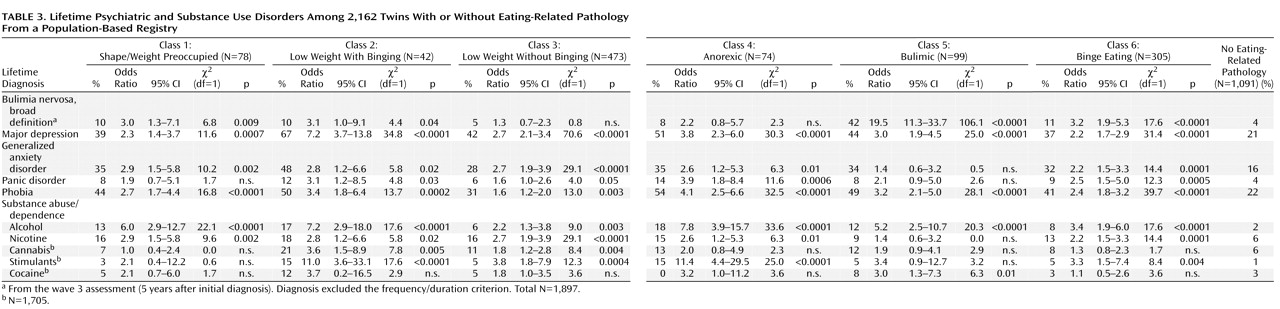
Comorbidity data used to validate the classes are presented in
Table 3. The odds ratios for a bulimia diagnosis at the wave 3 assessment were higher for the shape/weight preoccupied, low weight with binging, binge-eating, and especially for the bulimic class. Members of all six classes were significantly more likely to have comorbid major depression, phobias, and alcohol dependence. The odds ratios for comorbid generalized anxiety disorder and nicotine dependence were significantly higher for all but the bulimic class. Panic disorder and stimulant abuse or dependence were significantly more likely for all subjects except those in the shape/weight preoccupied and bulimic classes. The odds ratios for cannabis abuse or dependence were significantly higher in the low weight with and without binging classes, whereas only the bulimic class had a higher odds ratio for lifetime cocaine abuse or dependence. These results reflect robust differences across the six classes relative to the comparison group, since the probability of obtaining 43 significant results out of 60 comparisons at the p<0.05 level is <0.0007
(46).
Personality and attitudes
The eating disorder classes (classes 4, 5, and 6) exhibited the most deviant scores on the personality and attitudinal measures (
Table 4). In contrast to the comparison group, individuals in these classes exhibited higher dependency and lower mastery, optimism, and self-esteem. In addition, all of the classes derived from the latent class analysis (except class 2) had elevated levels of neuroticism. Excluding the comparison group and examining post hoc comparisons across the six classes, the bulimic and binge-eating classes scored higher on dependency and neuroticism and lower on mastery and self-esteem than the low weight without binging class. In addition, women in the anorexic class scored significantly lower on self-esteem and higher on neuroticism than the low weight without binging class. These results are also robust, since the probability of obtaining 18 significant results out of 48 comparisons at the p<0.05 level is <0.0001
(46). After isolating the three eating disorder groups (classes 4, 5, and 6), we found no significant differences for any personality measures (data not shown).
Lifetime history of eating disorders and obesity in co-twins
Table 5 presents the lifetime risk of bulimia nervosa, anorexia nervosa, and obesity for the co-twin of twins in each class, compared to the co-twins of the twins in the comparison group. Co-twins of twins in the bulimic and binge-eating classes were at significantly greater risk for lifetime history of bulimia nervosa. Co-twins of twins in the shape/weight preoccupied, low weight without binging, and anorexic classes were at significantly greater risk for lifetime anorexia nervosa. Only co-twins of twins in the binge-eating class were at significantly greater risk for obesity; having a co-twin in the low weight without binging class was protective against obesity.
Monozygotic-dizygotic concordance
The monozygotic twins showed greater concordance for class membership across the seven classes (the six classes derived from the latent class analysis and the comparison group) (χ2=112.0, df=36, p<0.0001; contingency coefficient=0.40) than did the dizygotic twins (χ2=59.8, df=36, p<0.008; contingency coefficient=0.34). In addition, there were 103 monozygotic and 74 dizygotic twins for whom both members of the twin pair were in classes 4, 5, or 6 (the eating disorder classes). The monozygotic twins demonstrated substantially greater concordance for class membership (χ2=56.9, df=4, p<0.0001; contingency coefficient=0.60) than did the dizygotic twins (χ2=9.1, df=4, p=0.06; contingency coefficient=0.33).
Severity of and reasons for low weight
In addition to the anorexic class, there were two classes marked by periods of significantly low body weight. When controlling for age, the mean lifetime lowest body mass index reported across the three classes differed significantly. Women in the anorexic and low weight with binging classes reported lower lifetime minimum body mass indexes (mean=16.6 kg/m2 [SD=1.1] and 16.5 kg/m2 [SD=2.0], respectively) than women in the low weight without binging class (mean=17.4 kg/m2, SD=2.0) (F=8.5, df=2, 544, p=0.0002).
We then reviewed the original interview forms in which the “reason for low weight” had been recorded for all women in class 2 and 50% of those in class 3. The reasons endorsed for low weight included constitutional thinness; weight loss secondary to depression, interpersonal loss, or anxiety; weight loss secondary to medical illness or procedures; and an array of infrequently endorsed reasons. There were significantly more women in class 2 than in class 3 who reported weight loss secondary to depression, anxiety, or interpersonal loss (22% versus 14%) (χ2=4.22, df=1, p<0.04). Given that the odds ratios for nicotine dependence were similarly higher in all but the bulimic class, it does not seem that low weight in this group would be fully accounted for by an excess of individuals who were dependent on nicotine.