We sought to clarify the relationship between family history of schizophrenia, negative symptoms, and the deficit syndrome. We independently categorized a large series of patients with schizophrenia by both family history and the presence of the deficit syndrome to examine if prominent negative symptoms were characteristic of familial schizophrenia. We overcame some methodological limitations of other studies by using rigorous family history and diagnostic assessment methods. We conducted structured symptom ratings during clinically determined medication treatment and, for nearly half the patients, also during both phases of a medication crossover study involving antipsychotic-free and antipsychotic treatment phases. The latter protocol provided an index of treatment response by measuring symptom changes between the antipsychotic-free and antipsychotic treatment conditions.
Results
Comparing Patients Grouped by Family History
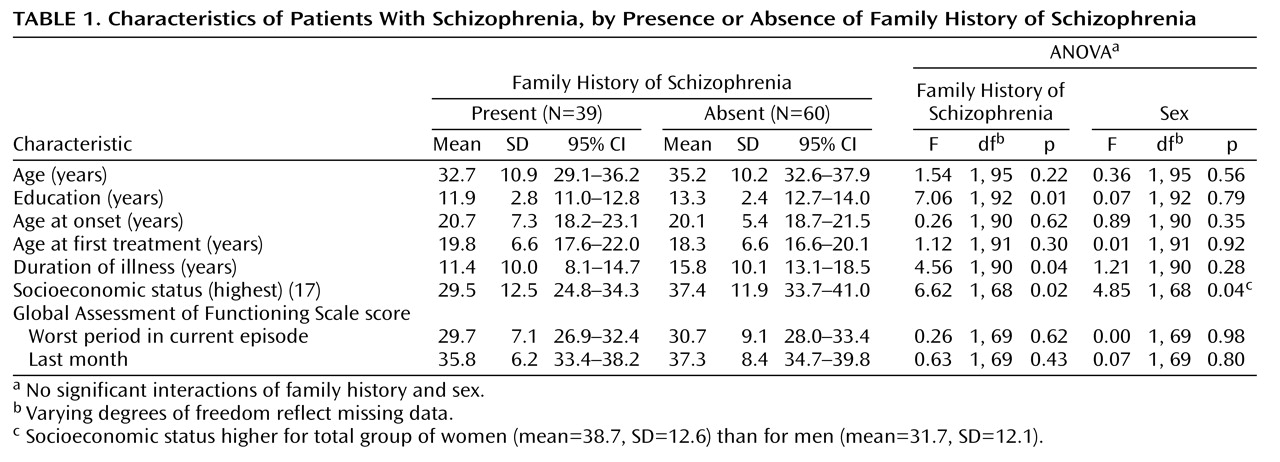
Family history groups did not differ significantly in the average number of relatives considered in making family history assessments (family history 1: mean=35.4, SD=15.5; family history 2: mean=32.8, SD=12.6; family history absent: mean=31.5, SD=10.0) (F=1.13, df=2, 96, p<0.34). The family history 1 and 2 groups were combined for subsequent analyses since they did not differ on any symptom measure or demographic variable or in sex distribution. Demographic characteristics of the patients grouped by family history are in
Table 1. The groups with and without family history did not differ in sex distribution (group with family history present: 27 of 63 men, 42.9%; 12 of 36 women, 33.3%) (χ
2=0.87, df=1, p=0.35) or ethnicity (group with family history present: 19 of 57 non-Hispanic Caucasians, 33.3%; 20 of 42 minorities, 47.6%) (χ
2=2.07, df=1, p=0.15). The groups also did not differ in age, age at onset, age at first treatment, or in global assessments of function during the worst period in the current episode or in the last month. However, the patients with a family history had significantly less education, a lower current socioeconomic status, and a shorter duration of illness. A single significant sex effect was present for socioeconomic status: the women exhibited a higher socioeconomic level. No significant interactions of family history and sex were revealed.
A similar proportion of the groups with and without family history had the deficit syndrome (group with family history present: N=12 of 37, 32.4%; group with family history absent: N=16 of 59, 27.1%) (Pearson χ2=0.31, df=1, p=0.58), but the category assignments for deficit syndrome and family history were unrelated. It was not surprising that all items from the Schedule for the Deficit Syndrome (which were used to make deficit syndrome designations) differed significantly between the groups with and without a deficit syndrome (F values ranged from 16.9 to 61.2, df=1, 93, all p<0.002), and there were no interactions of group and sex. In contrast, the groups with family history and no family history did not differ on any item on the Schedule for the Deficit Syndrome, although a sex effect, with men having a more diminished emotional range and sense of purpose than women, was present.
Comparing Patients Grouped by Deficit Syndrome
Only sex and education differed between the groups with and without the deficit syndrome: those with the deficit syndrome were more likely to be men (23 of 61 men, 37.7%; five of 35 women, 14.3%) (χ2=5.90, df=1, p=0.02) with less education (mean=12.1 years, SD=1.9; mean=13.2, SD=2.5, respectively) (F=3.98, df=1, 89, p=0.05). A significant interaction of deficit syndrome and sex was present for socioeconomic status (F=4.62, df=1, 64, p=0.04), with men with and without the deficit syndrome exhibiting similar socioeconomic status levels (32.1 and 31.5, respectively) and women with and without the deficit syndrome having quite different socioeconomic status (25.0 and 40.9, respectively).
Symptoms Across Groups With and Without Family History
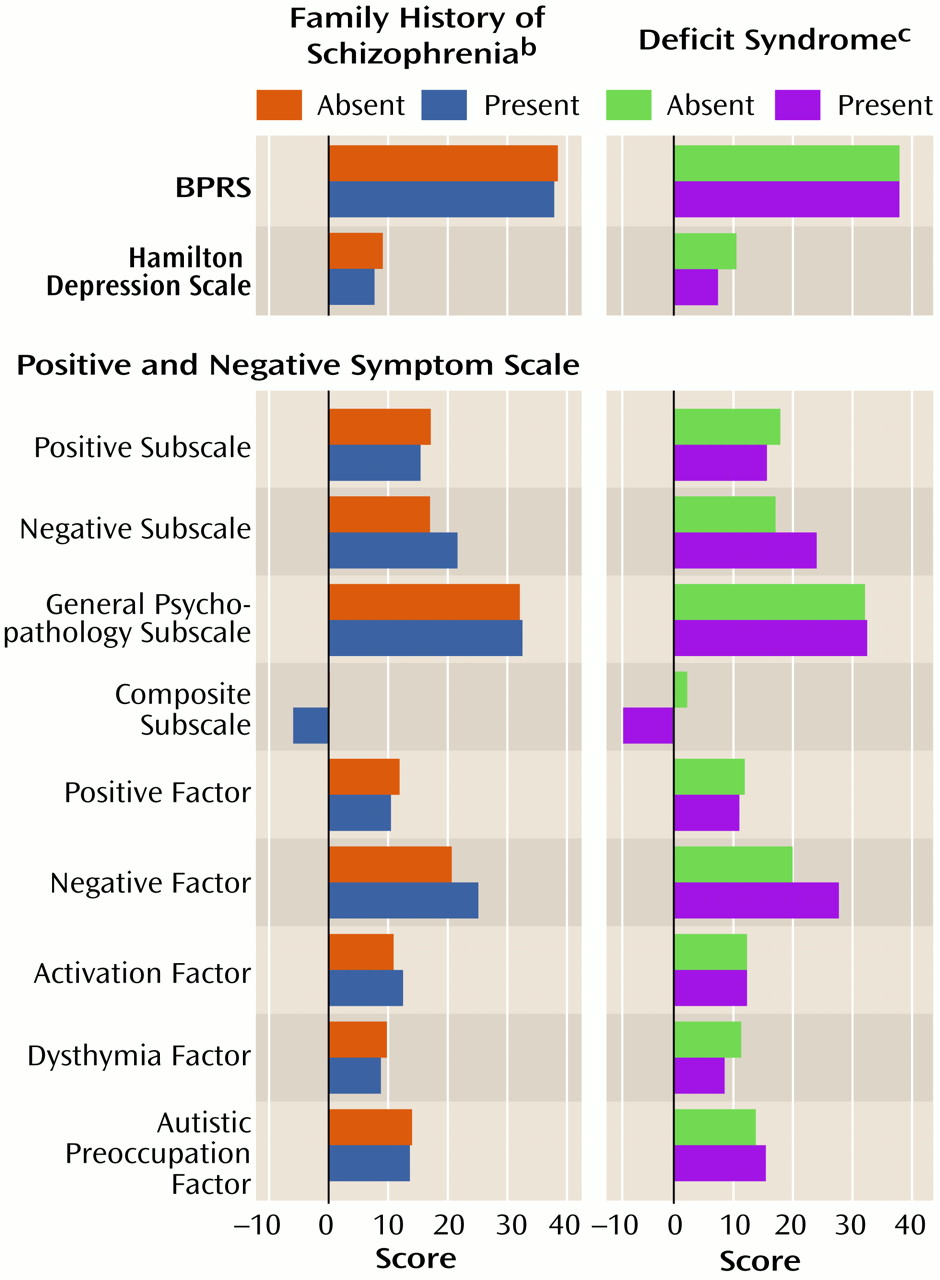
Figure 1 (column 1) presents ANOVA results for patient symptom ratings during individualized clinical treatment for the groups with and without family history. Only negative symptom ratings differed for the groups with and without family history. Those with family history present had higher negative subscale (F=7.89, df=1, 79, p=0.006) and negative factor (F=4.96, df=1, 79, p=0.03) scores and lower composite subscale scores, indicating that those with a family history had greater negative than positive symptoms. A sex effect was present on the positive subscale of the original Positive and Negative Syndrome Scale (with women having greater positive symptoms than men), and there was an interaction of family history group and sex on composite subscale scores (F=4.03, df=1, 79, p=0.05). Women in the groups with and without family history had identical composite subscale scores (2.1), but men had quite different scores (family history present: –9.2; family history absent:–1.1). We examined the individual items of the Positive and Negative Syndrome Scale that composed the subscale or factor scores that differed across the family history groups post hoc and found that the group with family history present had higher scores for emotional withdrawal (F=7.70, df=1, 79, p=0.007), poor rapport (F=14.83, df=1, 79, p<0.001), and lack of spontaneity (F=7.62, df=1, 79, p=0.007) than did those without family history.
Symptoms Across Groups With and Without the Deficit Syndrome
As seen in
Figure 1 (column 2), patients with the deficit syndrome also exhibited greater negative subscale and factor scores on the Positive and Negative Syndrome Scale (F=23.40, df=1, 76, p<0.001; F=18.77, df=1, 76, p<0.001, respectively) and lower composite subscale scores (F=18.94, df=1, 76, p<0.001) than patients without the deficit syndrome. Unlike the family history groups, the groups with and without the deficit syndrome differed in dysthymia ratings, with the group with the deficit syndrome having lower dysthymia scores (F=9.17, df=1, 76, p=0.003). Significant sex effects were present for positive and composite subscale scores (with women having greater symptoms than men) (F=6.14, df=1, 76, p=0.02; F=4.97, df=1, 76, p=0.03). There were no significant or marginal interactions of deficit syndrome and sex. The negative subscale and factor items on the Positive and Negative Syndrome Scale that contributed to the previous differences (using an alpha set at p<0.007 for significance) were all higher in the group with the deficit syndrome and consisted of blunted affect (F=22.21, df=1, 76, p<0.001), emotional withdrawal (F=11.84, df=1, 76, p<0.001), poor rapport (F=11.96, df=1, 79, p=0.001), passive or apathetic social withdrawal (F=8.08, df=1, 76, p<0.006), lack of spontaneity (F=18.83, df=1, 76, p<0.001), and motor retardation (F=18.75, df=1, 76, p<0.001). The differences in dysthymia scale scores were accounted for by lower guilt feelings (F=9.14, df=1, 76, p<0.003) and depression (F=9.77, df=1, 76, p<0.003) in the patients with the deficit syndrome, as would be expected.
Thus, both deficit syndrome and family history categorizations identified groups with greater emotional withdrawal, poor rapport, and lack of spontaneity. However, only the deficit syndrome group included patients with more affective blunting, motor retardation, and passive or apathetic social withdrawal.
Symptoms of Patients Studied Both With and Without Antipsychotic Medication
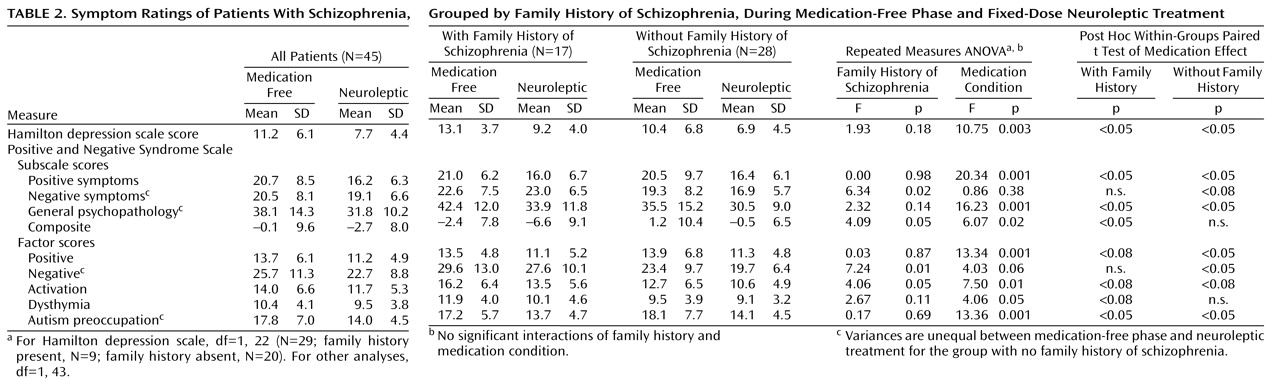
The 45 patients participating in the antipsychotic-free and antipsychotic treatment protocol did not differ from the larger group in demographic characteristics, symptoms, or proportion of group with family history: 43.6% of the patients with family history (17 of 39) and 46.7% of the patients with no family history (28 of 60). The median number of antipsychotic-free (median=21, range=7 to >30) and antipsychotic treatment (median=34, range=19 to >50) days for symptom scores on the Positive and Negative Syndrome Scale did not differ between patients with and without family history. Symptom ratings during the antipsychotic-free and antipsychotic treatment phases (medication conditions) were analyzed by a repeated measures ANOVA for patients grouped by family history and no family history (
Table 2) and then for patients with the deficit syndrome and no deficit syndrome (
Table 3) separately.
Family History Group and Medication Crossover Study
Family history group and medication condition affected subscale scores on the Positive and Negative Syndrome Scale, but there were no interactions of family history group and medication condition. For family history groupings, the group with family history exhibited greater negative symptom (negative subscale: F=6.34, df=1, 43, p<0.02; negative factor: F=7.24, df=1, 43, p<0.01), lower composite subscale (F=4.09, df=1, 43, p<0.05), and higher activation factor (F=4.06, df=1, 43, p<0.05) scores than the group without family history (
Table 2). For medication condition, all scores on the Positive and Negative Syndrome Scale, except for those on the negative subscale, showed significant decreases from medication-free to active treatment phases, consistent with a global improvement in symptoms during antipsychotic treatment. Post hoc tests revealed a similar group response for patients with and without family history across the medication conditions except for the negative symptom ratings. Although there was not a significant interaction in the repeated measures ANOVA, post hoc tests revealed that negative subscale scores for patients with family history did not improve during active treatment, whereas those for patients without family history did. The variances on a few symptom measures were unequal between medication-free and treatment phases for the group without family history but not for the group with family history.
Deficit Syndrome Group and Medication Crossover Study
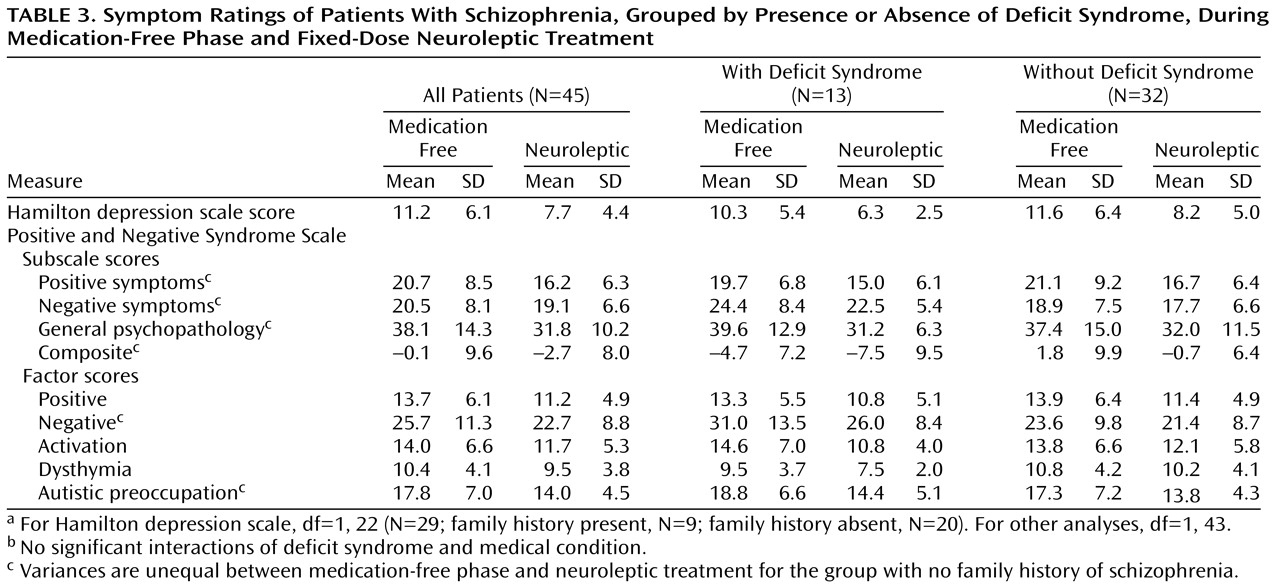
Repeated measures ANOVAs for groups with and without the deficit syndrome across medication conditions (
Table 3) yielded similar results for scores on both negative symptom measures and the composite subscale of the Positive and Negative Syndrome Scale. Furthermore, there were no significant interactions for deficit syndrome group and medication condition. The patients with the deficit syndrome exhibited higher negative symptom scores (negative subscale: F=6.78, df=1, 43, p<0.01; negative factor: F=4.32, df=1, 43, p<0.05) and lower composite subscale scores (F=7.30, df=1, 43, p<0.01) than patients without the deficit syndrome. Again, for medication condition, all scores on the Positive and Negative Syndrome Scale except the negative subscale decreased significantly from medication-free to active treatment phases. Post hoc tests also revealed patterns across the medication condition for the groups with and without the deficit syndrome similar to those for the groups with and without family history. The variances on a few symptom measures were unequal between the medication-free and treatment phases for the groups with and without the deficit syndrome.
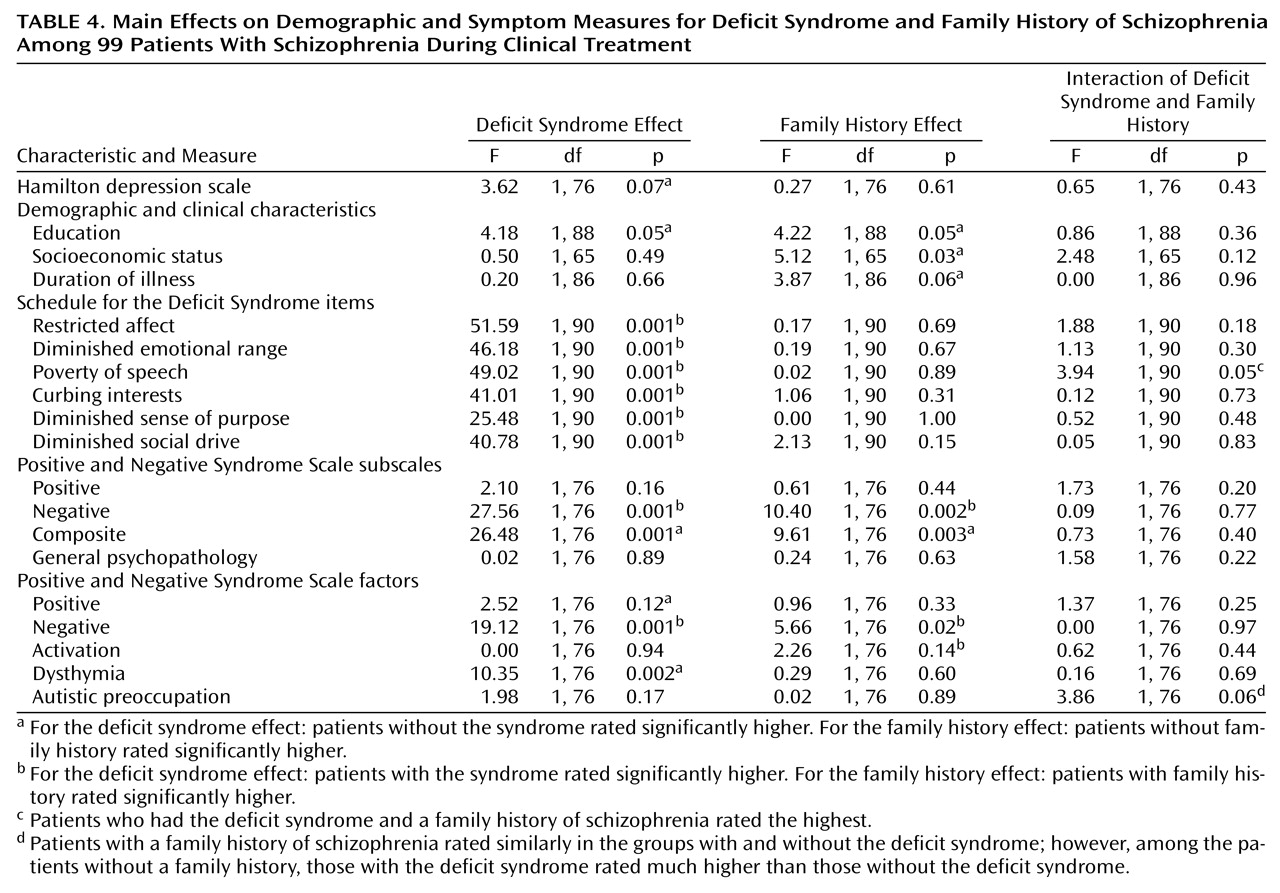
We conducted ANOVAs to look at measures that showed a significant main effect for the groups with and without family history and/or the groups with and without the deficit syndrome and examined if there were interactions between the groups.
Table 4 is a summary of findings for the family history and deficit syndrome categorizations and addresses any interaction of these groups. There were only two significant interactions that would not survive a Bonferroni correction. For the poverty of speech item on the Schedule for the Deficit Syndrome, both the groups with family history and the deficit syndrome exhibited the most variant (highest) scores. For the autistic preoccupation factor on the Positive and Negative Syndrome Scale, the scores for patients with family history were similar across the deficit syndrome parameter, whereas the scores for patients without family history and with the deficit syndrome were much higher than those for the patients without family history and without the deficit syndrome.
Typical Versus Atypical Antipsychotics in the Medication Crossover Study
We examined possible differences in symptom scores on the Positive and Negative Syndrome Scale for subjects receiving typical versus atypical antipsychotics in the medication condition of the crossover study. Scores were compared for groups with and without family history (and then for groups with and without the deficit syndrome) across typical or atypical antipsychotic treatment arms by repeated measures ANOVAs (data not shown). The use of atypical versus typical agents was unrelated to family history grouping. Typical antipsychotic agents were used among 64.1% (25 of 39) of the patients with family history present and 75.0% (45 of 60) of the patients with family history absent; the type of antipsychotic agent used had no effect on the data. The results were also unchanged if only patients receiving atypical agents were analyzed, although the group size was reduced. In addition, there was no interaction of antipsychotic type and family history group for any subscale scores on the Positive and Negative Syndrome Scale. For example, mean negative subscale scores for the group with family history during antipsychotic-free and typical antipsychotic treatment conditions were 21.9 (SD=7.0) and 22.2 (SD=6.7), respectively, whereas, for the group with family history receiving atypical antipsychotics, mean negative subscale scores were 23.8 (SD=8.9) and 24.2 (SD=6.5) (repeated measures ANOVA; effect of antipsychotic type: F=0.35, df=1, 14, p=0.56; effect of medication condition: F=0.00, df=1, 14, p=0.99). Likewise, mean negative subscale scores for the group without family history while antipsychotic free and during the typical antipsychotic treatment condition were 18.9 (SD=9.3) and 16.9 (SD=6.2); those for the group with no family history receiving atypical antipsychotics during the treatment condition were 20.4 (SD=3.9) and 16.6 (SD=3.8) (repeated measures ANOVA; effect of antipsychotic type: F=0.05, df=1, 25, p=0.82; effect of medication condition: F=0.29, df=1, 25, p=0.59.).
Discussion
The patients with schizophrenia and a family history of the illness were not more likely to have the deficit syndrome, although the presence of either family history or the deficit syndrome identified patients with greater negative symptoms. The family history characteristic actually better separated the patients into groups with improving and unchanging negative symptoms between the antipsychotic-free and treatment phases of the study. Indeed, only the group without family history showed improving negative symptoms with antipsychotic treatment. Neither patient group, when classified by the deficit syndrome, showed significant negative symptom differences between the treatment phases.
We next examined differences between the family history and deficit syndrome groupings that might explain why both categorizations were related to global negative symptoms but were unrelated to one another. We looked at the relationship between the family history and deficit syndrome categorizations, both of which are unchanging (trait) characteristics, and individual items on the Positive and Negative Syndrome Scale that assess clinical state symptom measures. Since there were so few interaction terms between the groupings to explain observed phenomena, it is feasible that the family history and deficit syndrome designations capture different dimensions of negative symptoms.
There were three negative symptoms that differed between groups with and without the deficit syndrome that did not significantly differ between the patients when they were grouped by family history: affective blunting, motor retardation, and passive or apathetic social withdrawal. The first symptom, blunted affect, is related to two of the enduring and primary criteria on the Schedule for the Deficit Syndrome that define the deficit syndrome: restricted affect and diminished emotional range. Also, the passive or apathetic social withdrawal symptom may phenomenologically contribute to another three of four remaining criteria on the Schedule for the Deficit Syndrome: curbing of interests, diminished sense of purpose, and diminished social drive. These state symptom differences between the groups with and without the deficit syndrome are consistent with the requisite criteria for the deficit syndrome.
The three other items on the Positive and Negative Syndrome Scale that significantly differed between the groups with and without the deficit syndrome comprised the only symptoms that distinguished the groups with and without family history: emotional withdrawal, poor rapport, and lack of spontaneity. If these state measures differ from the primary and stable criteria on the Schedule for the Deficit Syndrome, it might explain why the familial patients did not have increased rates of the deficit syndrome, despite having high and medication-resistant negative symptoms. Two of the three symptom items differing only between groups with and without the deficit syndrome (affective blunting and motor retardation) reflect psychomotor performance more than social functioning. In contrast, the limited set of symptoms that distinguished the familial groups are related to interpersonal functioning and are remarkably similar to the criteria for DSM-IV axis II schizoid personality disorder, which has demonstrated a genetic relationship to schizophrenia. It should be noted that there is significant overlap among types of negative symptoms and that this study does not in itself contain any empiric evidence to support the distinction between the types of negative symptoms we found differentially characterizing the deficit syndrome and family history groupings.
Although negative symptoms differentiated both the family history and deficit syndrome groupings, only medication condition accounted for the improvement in positive symptoms and global improvement. This independence of positive symptom magnitude and response from that of negative symptoms is in keeping with the idea that positive and negative symptoms are distinct domains of illness
(22), as supported by their different relationships to neural regions, cognitive function, and longitudinal courses
(23–
25).
These data do not address the validity of the deficit concept but rather explore how it differs from the increased stable negative symptoms we observed in familial schizophrenia. This study has limitations, particularly in that its duration was too short to reveal differences in the stability of negative symptoms in the groups with and without family history. There are also potential confounds to assessing and interpreting negative symptoms that we have tried to address. First, negative symptoms can be related to overall illness severity, but our deficit syndrome and family history groups had similar total scores on the Brief Psychiatric Rating Scale and similar global assessments of function. Second, negative symptoms can be reactions to positive symptoms, but none of the patient groups differed in positive symptoms. Third, negative symptoms can be difficult to distinguish from (or can be related to) anxiety and depression, but none of the relevant scores on the Positive and Negative Syndrome Scale or the Hamilton depression scale suggested the presence of these comorbid conditions. Indeed, the patients without the deficit syndrome actually had higher dysthymia factor scores than patients with the deficit syndrome. Also, we excluded patients with schizoaffective disorder from the study. Fourth, typical and atypical antipsychotics may arguably differ in their efficacy in treating negative symptoms and inducing motor side effects. But our patient groups did not differ in the proportions taking atypical and typical antipsychotics, and there was no interaction of antipsychotic type with the family history or deficit syndrome groups. Fifth, antipsychotic side effects such as akinesia can resemble negative symptoms. However, we used benztropine for extrapyramidal symptoms and lorazepam for akinesia on an individualized, clinically determined basis, and the use of these medications did not differ among the groups. Sixth, although demographic characteristics have been related to negative symptoms, the patients with and without the deficit syndrome and family history did not differ in age, age at onset, or ethnicity, and we included sex as a factor in all analyses. Illness chronicity also seems unlikely to account for the greater negative symptoms, since patients with family history actually had a significantly shorter duration of illness than the patients without family history and patients with and without the deficit syndrome did not differ in illness duration. Although demoralization and environmental deprivation have been related to negative symptoms, all of our patients were studied in the same inpatient unit. Our familial patients did have lower socioeconomic attainment, which may be more a consequence than a cause of higher negative symptoms.
We examined and presented Positive and Negative Syndrome Scale symptom data using the original and the new factor-derived solutions of the Positive and Negative Syndrome Scale items
(22) so the comparability of these data to other published results could be examined. The factor-derived solution has enhanced properties in separating mood items from other psychopathology and an enhanced distribution of negative-type phenomena among its negative, activation, and autistic preoccupation factors. Items from the Positive and Negative Syndrome Scale on lack of insight, judgment, and preoccupation measures were removed from the scale’s factor pentagonal model
(21) because they diffusely loaded with other criteria. It was the use of the factor-derived measures from the Positive and Negative Syndrome Scale that showed the difference in dysthymia scores between the groups with and without the deficit syndrome. In contrast, the groups with and without family history did not differ on any indices of depression. This finding further supports the view that the deficit syndrome categorization was not assessing depressive symptoms.
We recognize that family history research methods can lead to misclassification with respect to genetic causality, especially for nonfamilial patients who have heritable forms of illness. The similar number of relatives considered for diagnosis in the different family history groups suggests that family size did not bias our identification of schizophrenia reoccurrences in the relatives. We used only schizophrenia-related chronic psychosis (schizophrenia, schizoaffective, and psychosis not otherwise specified) to define the affectation status of relatives. It is possible that the proportion of patients with family history would have been higher had we also included personality disorders in the relatives as reoccurrences. Particularly given these caveats, we consider that these differences in negative symptoms between the family history groups provide support for the hypothesis that there are real differences in negative symptoms between the groups with and without family history. The unchanging variance in symptoms between medication-free and treatment conditions only for patients with family history is also consistent with the greater homogeneity found in the familial patients with respect to medication response.
Since we made our family diagnoses from psychiatric information from family informants, we obtained some information about all known relatives (even those who had moved away, died, or committed suicide). Although this method is vulnerable to the underreporting of affective illness, substance abuse, and personality disorders, it is sensitive to the presence of broadly defined psychotic illness in relatives
(26), as was used in this study. It is worth noting that the increase in negative symptoms for familial patients was present even though positive symptoms defined illness occurrences in relatives. Our method of combining the patients with a first-degree relative with schizophrenia with those with reoccurrence in second-degree relatives is similar to that in other reports grouping all such patients as familial. It may be of interest that the group with only second-degree relatives with schizophrenia had negative symptom scores that were intermediate to those of the group with first-degree relatives with schizophrenia and the group with no family history.
The present data add to the literature suggesting that negative symptoms are related to the genetic vulnerability for developing schizophrenia, particularly those symptoms concerning emotional and interpersonal functioning. The data are also consistent with the idea that negative symptoms in familial schizophrenia may differ in etiology and treatment response from those in other patients with schizophrenia
(10,
27,
28). Negative symptoms account for the most debilitating aspects of schizophrenia. Their excess may explain the lower education and socioeconomic status of our familial patients, although the burden of psychiatric illness in the family for some patients in the familial group could also have affected these measures.
If family history does contribute some variance in negative symptom response, this might be worth considering in evaluating the efficacy of medication treatment for these symptoms. Further research in this area to refine assessments of the dimensions of negative symptoms may facilitate both genetic and pharmacological research. It may be useful to redefine a version of the deficit syndrome with different terms for its primary features, which could be examined in serious genetic studies using twin and adoption methods.