Single mothers currently head at least 12% of Canadian families with children
(1). Studies examining the health of single mothers have demonstrated higher rates of physical and mental health difficulties among single mothers than among mothers in two-parent families
(2–
5). For example, we found that single mothers were significantly more likely to have mental health problems such as a history of affective disorder, current dissatisfaction with multiple aspects of life, or one or more psychiatric disorders in the past year
(2).
Stressors, both past and present, are associated with higher rates of psychiatric problems. Socioeconomic disadvantage is an example of a current stressor that is much more common among single than married mothers
(3; unpublished 1993 study by Avison and Thorpe). Past stressors include adverse life events, such as parental death and childhood maltreatment. To our knowledge, no study has examined the relationship among childhood maltreatment, marital status, and psychiatric disorders in a general population sample.
The objective of this study was to examine the relationship between childhood abuse and psychiatric disorders among single and married mothers. To do so, we 1) compared the prevalence of childhood abuse and psychiatric disorders among single and married mothers and 2) examined the association among childhood abuse, marital status, and psychiatric disorders while controlling for other risk variables. We used general population data collected as part of the Mental Health Supplement to the Ontario Health Survey.
Method
Study Sample
Respondents to the Mental Health Supplement to the Ontario Health Survey were a subset of participants from the Ontario Health Survey, a province-wide survey of 61,239 people completed in 1990. The design of the Ontario Health Survey included stratification, clustering, and probability sampling. A detailed review of the survey methodology is described elsewhere
(6).
Respondents eligible for the Mental Health Supplement to the Ontario Health Survey were Ontario Health Survey participants in the third and fourth quarters of data collection
(7). One respondent was selected from each household. Eligible respondents aged 15–24 years had a chance of being selected that was three times greater than that of eligible respondents 25 years or older in the same household. This oversampling increased the precision of estimates for 15–24-year-olds. As a result, 19.0% of the respondents to the Mental Health Supplement to the Ontario Health Survey were 15–24 years of age, compared with 17.7% of the 1991 Ontario population. Respondents aged 65 years and over were eligible for inclusion if they scored fewer than 11 errors on the standardized Mini-Mental State
(8).
The Mental Health Supplement to the Ontario Health Survey was conducted between December 1990 and April 1991. Almost 10,000 (9,953) people aged 15–98 years participated (76.5% of eligible respondents from the Ontario Health Survey). Reasons for nonparticipation were refusal (N=751); sickness, death, or language difficulties (N=431); failure to contact the household during the survey period (N=744); and unspecified (N=845).
Mothers 15 years and older with at least one dependent child (under 16 years old) were eligible for participation in the study (N=1,540). Only mothers with complete information on all variables available were used in our analysis (N=1,471).
Measures
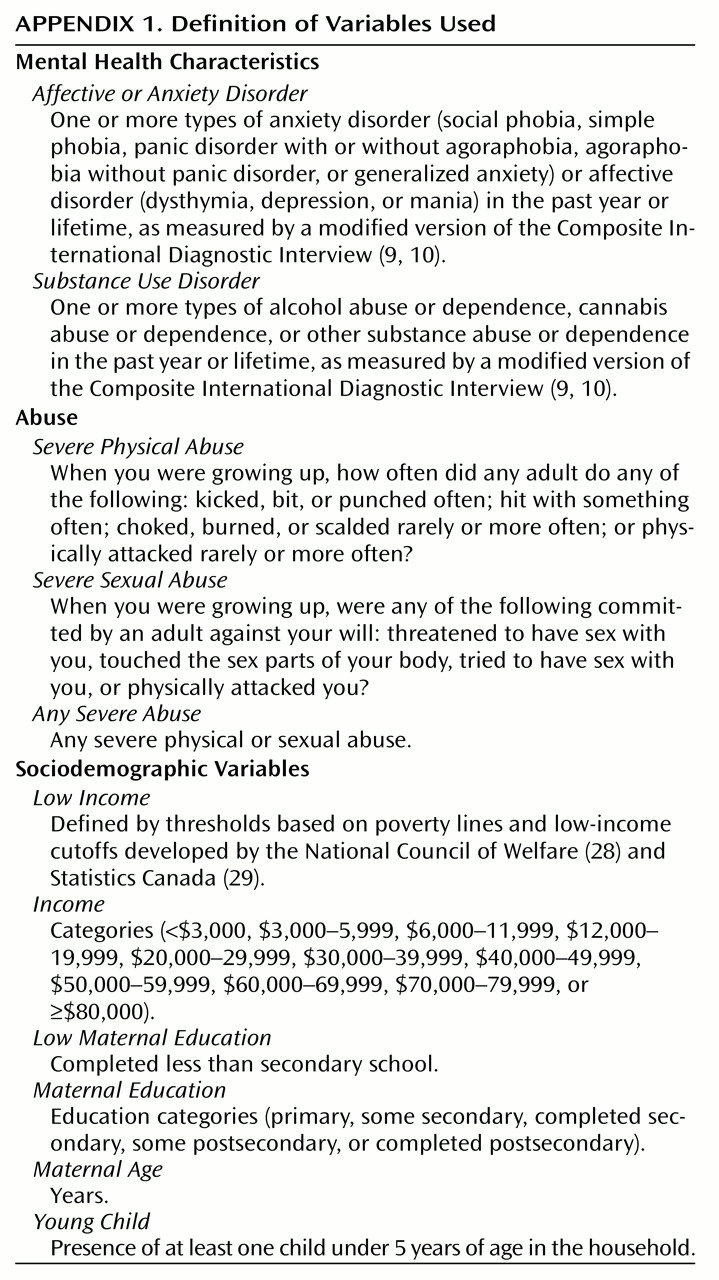
Measures used included the presence of severe childhood abuse (physical, sexual, or any) and psychiatric disorders (affective or anxiety disorder or substance use disorder in the past year or lifetime). Psychiatric disorders were measured by means of a modified Composite International Diagnostic Interview
(9,
10). All data were collected by means of an interviewer-administered questionnaire except the abuse data, which were collected by means of the self-administered Child Maltreatment History Self-Report
(11). All variables are defined in
Appendix 1.
There were 222 mothers with at least one child under 16 years for which the exact age of the child could not be ascertained. These data are included in a variable defined as “missing young child,” coded as 1 (missing) versus 0 (not missing).
Analysis
We calculated the prevalence rates of childhood abuse, psychiatric disorder, and selected sociodemographic characteristics for single and married mothers and the relative odds ratios and 95% confidence intervals (CIs) to estimate the strength of the association among single mother status and the other variables. The chi-squared statistic was used to evaluate the statistical significance of the differences between single and married mothers.
Multiple logistic regression analysis was used to determine the strength of the association among childhood abuse, family status, and selected other variables with psychiatric disorder. This was done by forcing all selected independent variables (childhood abuse [any severe abuse], single mother status, income, maternal education, maternal age, young child, and missing young child) into the model and testing for significant interactions between single mother status and the preceding variables to determine which interactions to retain in the model.
To obtain unbiased point estimates, subject responses were weighted by their probability of selection in the sample. The weighting incorporated adjustments for nonresponse to the Ontario Health Survey and the Mental Health Supplement to the Ontario Health Survey and brought the age and sex distribution of the sample into agreement with the distribution of the Ontario population in 1990. SUDAAN (version 7.5, Research Triangle Institute, N.C., 1999) was used for all analyses.
Results
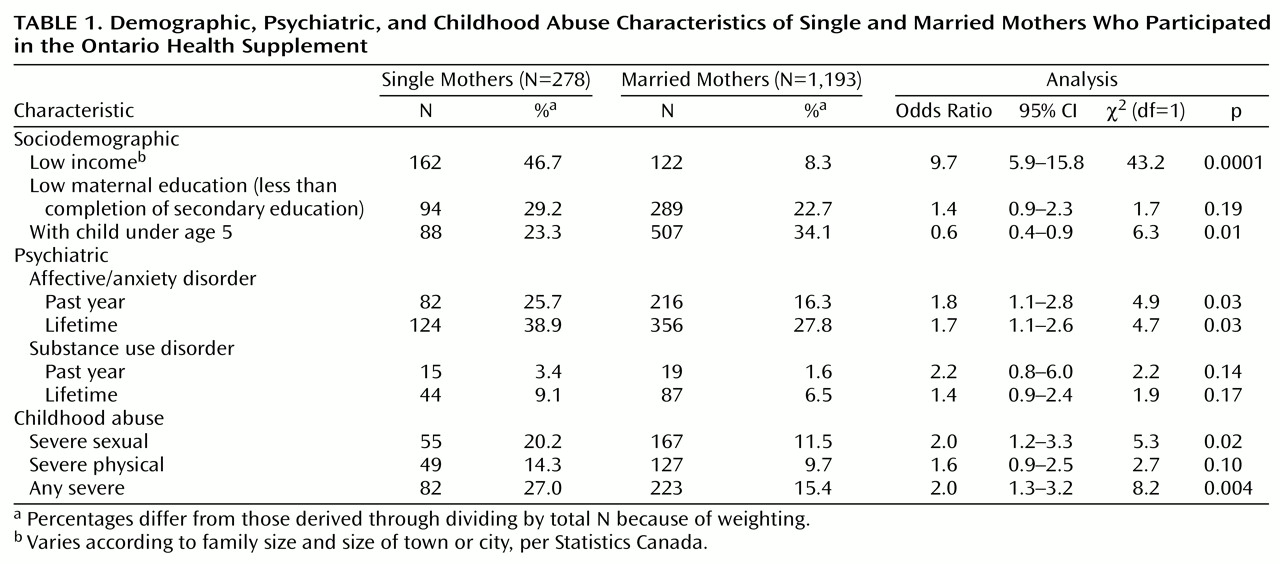
Table 1 provides demographic, psychiatric, and childhood abuse characteristics of the single and married mothers. Single mothers accounted for 18.9% (278 of 1,471) of the sample. The mean ages of the single and married mothers were 36.0 years (SD=10.3) and 36.1 years (SD=12.6), respectively. Almost half of the single mothers were poor compared with less than one-tenth of the married mothers. The prevalence of all psychiatric disorders was higher among single mothers than among married mothers. For example, a lifetime history of affective or anxiety disorder was reported in 38.9% of single mothers and 27.8% of married mothers. The reported rate of any severe childhood abuse among single mothers was almost twice that of married mothers.
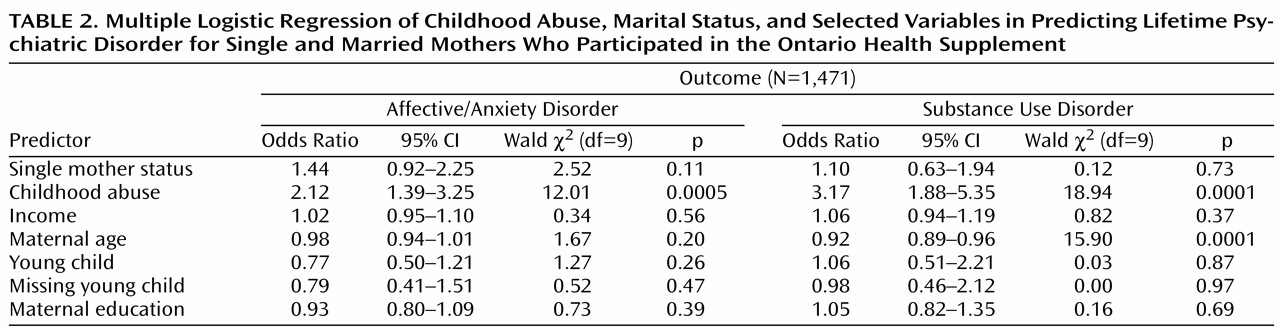
Table 2 presents the strength of the association (odds ratios) obtained by means of logistic regression among childhood abuse, single mother status, and selected other variables in predicting lifetime psychiatric disorder. Childhood abuse significantly predicted both psychiatric outcomes and resulted in the largest effect sizes: the odds of a mother who reported childhood abuse experiencing psychiatric morbidity was at least twice that of a mother not reporting childhood abuse. The effect sizes for single mother status were relatively small and nonsignificant. None of the interactions between single mother status and the other tested variables (e.g., abuse) was retained in the model. Additional regressions were performed for psychiatric outcome in the past year. Childhood abuse significantly predicted both psychiatric outcomes (affective or anxiety disorder: odds ratio=2.49, χ
2=15.81, df=1, p=0.0001; substance use disorder: odds ratio=6.18, χ
2=7.77, df=1, p=0.01). Single mother status did not significantly predict either psychiatric outcome in the past year: affective or anxiety disorder, odds ratio=1.53, χ
2=2.99, df=1, p=0.08; substance use disorder, odds ratio=1.32, χ
2=0.23, df=1, p=0.63. No other main effects or interactions significantly predicted outcome.
Discussion
Comparisons between single and married mothers in a large general population sample from Ontario consistently revealed that single mothers reported a higher prevalence of severe childhood abuse than married mothers. The odds of a single mother reporting severe childhood sexual abuse, or any severe childhood abuse, was twice that of married mothers. Single mothers also had higher rates of all psychiatric disorders examined and lower incomes.
Logistic regression analysis revealed that reported childhood abuse was a strong and significant predictor of maternal psychiatric morbidity, even after controlling for other risk variables (family composition, maternal age, and sociodemographic variables). The effect sizes of single mother status on outcome were nonsignificant, and no significant interactions were found between single mother status and other variables, such as childhood abuse, for psychiatric outcomes.
Two cross-sectional studies performed with disadvantaged populations both found a higher prevalence of childhood maltreatment among single mothers than among married mothers
(12,
13). In the study of 404 inner-city British women, the authors stated that both single mother status and childhood maltreatment predicted comorbid depression and anxiety disorders, but no specific estimates were provided
(12). The Mental Health Supplement to the Ontario Health Survey was the first survey to examine the rate of childhood abuse among single mothers in the general population.
Higher levels of reported childhood abuse and psychiatric disorders among single mothers led us to test for an interaction between single mother status and childhood abuse in the prediction of psychiatric outcomes. The theoretical basis for this test is the hypothesis that exposure to childhood abuse creates an early vulnerability to psychiatric difficulties that is activated by periods of interpersonal stress (e.g., at marital dissolution). Conversely, the absence of such stress (e.g., maintenance of an intact family) attenuates some of the negative effects associated with exposure to childhood abuse. This study does not support a differential effect of childhood abuse on single mothers compared with married mothers in predicting psychiatric disorders.
Comparisons of difficulties among single and married mothers must be interpreted cautiously. The tradition of comparing single mothers with mothers from potentially less stressed groups may be seen as perpetuating negative stereotypes about single mothers
(14,
15). There is considerable heterogeneity among single mothers
(2), and there are likely marked individual differences in how they cope
(16). In the current study, single and married mothers both showed difficulties associated with childhood abuse. The similarities between these two groups of mothers are as important as the differences.
Strengths of the Mental Health Supplement to the Ontario Health Survey include rigorous methodology and sophisticated sampling techniques to ensure a group representative of the general population, a large sample size, and poststratification weighting to minimize bias associated with the loss of participants.
Limitations include the inability to establish the chronology of experiences such as childhood abuse and psychiatric problems in a cross-sectional study. Also, the sampling strategy used in the Mental Health Supplement to the Ontario Health Survey focused on household dwellings, excluding specific groups (homeless people or native people living on reserves) who might have been at a higher risk for both childhood abuse and single parenthood
(17–
19). Since these groups represent a small proportion of the total population of Ontario
(20), their exclusion is unlikely to have a large impact.
Possible biases associated with retrospective self-reports of childhood abuse
(21–
25) must be acknowledged. However, there is no reason to suggest that a selective difference in recall exists between single and married mothers
(26). It is unlikely that recall bias could account for the finding that single mothers reported a greater prevalence of childhood abuse than did married mothers.
Results of this study have implications for the research, clinical, and policy fields. Researchers must endeavor to further understand the mechanisms through which childhood abuse influences adult mental health. Clinicians should be cognizant of the high prevalence of childhood abuse among single mothers. Routine assessments of mothers with psychiatric difficulties, particularly single mothers, should include questions about childhood abuse. Treatment of psychiatric conditions such as depression may be influenced by a history of childhood abuse
(27). Finally, these findings should encourage policy makers to make interventions for childhood maltreatment a priority. These data suggest that decreasing childhood abuse can potentially have a long-term influence on reducing the prevalence of adult psychiatric disorders, such as mood disorders, and the associated burden of suffering.
In conclusion, single mothers reported higher rates of childhood abuse than did married mothers. A strong and significant association exists between childhood abuse and psychiatric difficulties for both single and married mothers, even when maternal age, family composition, and sociodemographic disadvantages are controlled. No interaction between single mother status and childhood abuse was found for psychiatric outcomes. The mechanisms through which childhood abuse influences adult mental health are yet to be determined. This problem deserves further study in both single and married mothers.