Since ADHD and learning disabilities are both familial conditions, family studies can help to clarify the nature of their association by examining patterns of aggregation in first-degree relatives
(6). When we examined ADHD and learning disabilities in a large study of boys with and without ADHD and their first-degree relatives, results suggested that ADHD and learning disabilities were etiologically independent rather than either different manifestations of the same underlying condition or consequences of one another
(3). Results further suggested that the comorbidity of ADHD and learning disabilities was the result of assortative, or nonrandom, mating between parents (i.e., individuals with ADHD showed a tendency to marry and have children with learning-disabled individuals at a rate greater than chance). These findings are consistent with a growing number of studies supporting the validity of ADHD and learning disabilities as separate conditions with unique risk factors and cognitive manifestations
(1,
7–
9).
Yet, similar to the general literature on ADHD, studies that have examined the relationship between ADHD and learning disabilities have primarily been based on studies of boys. Thus, the generalizability of these results to girls with ADHD remains unknown
(10). Understanding the nature of the relationship between ADHD and learning disabilities in girls has important clinical and scientific relevance in light of emerging concerns about the underidentification and undertreatment of girls with ADHD
(11). ADHD and learning disabilities require different therapeutic approaches, with ADHD generally benefiting from pharmacological treatment and learning disabilities benefiting from a specialized educational curriculum. Thus, establishing the validity of the co-occurrence of these conditions has implications for the management of affected individuals.
The present study used the same familial risk analysis methods as our previous study of boys to examine the relationship between ADHD and learning disabilities in a group of girls and their parents and siblings. By comparing the actual aggregation of ADHD and learning disabilities in relatives to patterns predicted by different models of transmission, we aimed to determine the relationship of these conditions in female subjects. On the basis of our previous study of boys, we hypothesized that ADHD and learning disabilities in girls would be separate conditions transmitted independently and that their comorbidity would be due to nonrandom mating between parents.
Method
The current analyses are derived from a longitudinal family study of girls with and without ADHD and their nuclear families
(12). Greater details of the methods used in this study are reported elsewhere
(12,
13). Briefly, we studied two female index groups: 140 ADHD probands and 122 comparison probands without ADHD. These groups had 417 and 369 first-degree biological relatives, respectively. All probands were girls between the ages of 6 and 18. No ethnic or racial groups were excluded from the study. Potential probands were excluded if they were adopted or if their nuclear family was not available for study. We also excluded probands who had major sensorimotor handicaps (paralysis, deafness, blindness), psychosis, autism, or a full-scale IQ less than 80. Additionally, subjects from the lowest socioeconomic status
(14) were excluded in order to minimize the potential confounds of extreme social adversity. All of the ADHD probands met diagnostic criteria for current ADHD at the time of clinical referral, and each had active symptoms of the disorder at the time of recruitment.
Two independent sources—one psychiatric and one pediatric—provided the index children. Girls with ADHD who were considered psychiatric probands were selected from consecutive referrals to a pediatric psychopharmacology program at a major university hospital. This site is not a tertiary care clinic, since approximately 50% of new patients have never been diagnosed or treated before. Pediatrically referred ADHD probands were referred from pediatricians at a large health maintenance organization (HMO) in the Boston area. The comparison probands without ADHD were selected from the general pediatric practices within the hospital and HMO settings; these individuals were selected because they had a pediatrician at one of these sites. Before participation in the study, all parents provided written consent for themselves and their children, and children gave written assent.
Since the determination of learning disabilities was based on information collected from psychological testing, relatives who were not available for in-person evaluations were excluded from the current analyses. Direct assessments for ADHD and learning disabilities were conducted on 87% of the first-degree relatives of ADHD probands (N=361) and 86% of the first-degree relatives of the comparison probands (N=318).
Similarly, a small number of probands from the larger family study were not eligible for inclusion in the current analyses because they had not completed at least one of the tests required for calculation of the learning disabilities variable. Lack of completion occurred because of factors such as time constraints of subjects on the date of the interview, lack of cooperation of the subject, or rater error. Of the 140 ADHD probands, 98% completed the full cognitive battery. Of the 122 comparison probands, 93% completed the full battery. Thus, the final number of ADHD and comparison probands eligible for the current study were 137 and 113, respectively.
Measures
Diagnostic data on probands and siblings 12 years of age and older were obtained from independent interviews with them and their mothers by using the Schedule for Affective Disorders and Schizophrenia for School-Age Children—Epidemiologic Version (K-SADS-E)
(15). Children younger than 12 years of age were not interviewed directly; diagnostic information on these subjects came from parent interviews only. Diagnostic assessments of parents were based on direct interviews with the Structured Clinical Interview for DSM-III-R (SCID)
(16). Interviewers were unaware of the proband’s diagnosis. Interviewers had undergraduate degrees in psychology and were trained to high levels of interrater reliability. We computed kappa coefficients of agreement by having three experienced, board-certified child and adult psychiatrists diagnose subjects from audiotaped interviews made by the interviewing staff. On the basis of 173 interviews, good agreement was seen for all K-SADS-E diagnoses (median kappa=0.86) and for ADHD (kappa=0.99).
We scored the ADHD diagnosis as positive if, on the basis of the interview results, DSM-III-R criteria were unequivocally met. All diagnostic uncertainties were resolved by a four-person committee of board-certified child and adult psychiatrists from which the chairperson (J.B.) sought consensus. The committee members were unaware of the subject’s ascertainment group, cognitive data, and all data collected from family members. For children older than 12, the ADHD diagnosis was based on combined data from direct and indirect interviews; a symptom was considered positive if it was endorsed in either interview.
Interviewers were trained to administer tests of cognitive functioning and academic achievement by a licensed child psychologist (Dennis K. Norman, Ed.D.) who continued to supervise them throughout the study. For subjects younger than 17, estimates of cognitive functioning were obtained with the Wechsler Intelligence Scale for Children—Revised (WISC-R)
(17). Subjects completed the vocabulary, block design, arithmetic, digit span, and coding subtests. For 17- and 18-year-old subjects, estimates of cognitive functioning were obtained with the Wechsler Adult Intelligence Scale—Revised (WAIS-R)
(18). These subjects completed the vocabulary, block design, arithmetic, digit span, and digit symbol subtests. As per the methods of Sattler
(19), we estimated full-scale IQ by using the vocabulary and block design subtests from the WISC-R and WAIS-R as proxies for verbal and performance IQ. Academic achievement was assessed with the arithmetic and reading subtests of the Wide Range Achievement Test—Revised
(20).
The definition of a learning disability under Public Law 94-142 requires a significant discrepancy between a child’s aptitude and achievement
(21). Reynolds
(22) provided a thorough review of measurement issues involved in the definition of learning disabilities. We used the procedure recommended by him and others
(23) as follows. We first converted the estimated full-scale IQ and achievement scores to z scores (z
IQ and z
A, respectively). We then estimated the expected achievement scores (z
EA) by the regression equation
where r
IQA is the correlation between IQ and achievement. The discrepancy score is z
EA minus z
A, the standard deviation is
and the standardized discrepancy score was thus calculated as
with subjects whose scores were >1.65 defined as having a learning disability in reading or arithmetic.
Analyses
We stratified participants into three groups for analyses: female ADHD probands with a comorbid learning disability (N=21) and their parents and siblings (N=58), female ADHD probands without a learning disability (N=116) and their parents and siblings (N=303), and female comparison subjects without ADHD (N=113) and their parents and siblings (N=318).
We compared rates of ADHD and learning disabilities in the relatives of each group by using the generalized estimating equation method
(24), as implemented in Stata
(25), to fit logistic regression models that account for the nonindependence of relatives. A working correlation structure (independence) was used with empirical estimates of variance in order to produce consistent standard errors and p values. Models were specified with the binomial family and a logit link to conduct logistic regression, with the three groups of proband diagnoses as the independent variables and the rates of ADHD and learning disabilities in relatives as the dependent variables. For comparison of individual variables, we used the Wald chi-square test to determine significance. All tests were two-tailed with alpha set at 0.05.
By comparing the familial aggregation of the conditions across groups to the patterns expected on the basis of different modes of transmission, we inferred the etiologic association between ADHD and learning disabilities
(6,
26–
28). Specifically, we compared our data to three basic hypotheses regarding the relationship in girls between ADHD and learning disabilities.
First, we examined whether the presence of a learning disability is secondary to the cognitive impairments associated with ADHD. This hypothesis predicts no familial transmission of learning disabilities in the families of the ADHD probands either with or without a learning disability, although some increase in learning disabilities might be found among the ADHD relatives of ADHD probands.
Second, we examined whether ADHD and learning disabilities share common etiological factors but either differ in severity (ADHD with a learning disability being more severe than ADHD without a learning disability) or differ in expression because of environmental factors. If ADHD with a learning disability is a more severe form of the disorder than ADHD without a learning disability, there would be higher rates of both ADHD and learning disabilities among relatives of ADHD probands with a learning disability than in relatives of ADHD probands without a learning disability. In addition, relatives of ADHD probands either with or without a learning disability should have higher risks for each disorder than relatives of the comparison probands. If ADHD children either with or without a learning disability share common familial etiologic factors but differ because of environmental effects, we would find similar rates of ADHD and learning disabilities in the relatives of both subgroups.
Third, we examined whether ADHD and learning disabilities are distinct conditions. If so, we would find equally high rates of ADHD in the first-degree relatives of ADHD probands either with or without a learning disability, and the prevalence of learning disabilities should be higher only among relatives of girls with both ADHD and a learning disability. If our data were consistent with this pattern of transmission, we would then ascertain whether ADHD with a learning disability was a distinct familial subtype by testing for cosegregation (i.e., the co-occurrence of the two disorders in individual relatives). That is, among the relatives of ADHD probands with a comorbid learning disability, we would compare the rate of learning disabilities between those with and those without ADHD. If the disorders did not cosegregate (i.e., if the rates of learning disabilities did not differ between those two groups), we would then examine whether the comorbidity of ADHD and learning disabilities appears as a result of either chance or assortative mating in parents. Assortative, or nonrandom mating, refers to individuals with one disorder showing a tendency to marry and have children with individuals who have another disorder. To test for assortative mating, we test for an association between ADHD in fathers and a learning disability in mothers and between a learning disability in fathers and ADHD in mothers.
Results
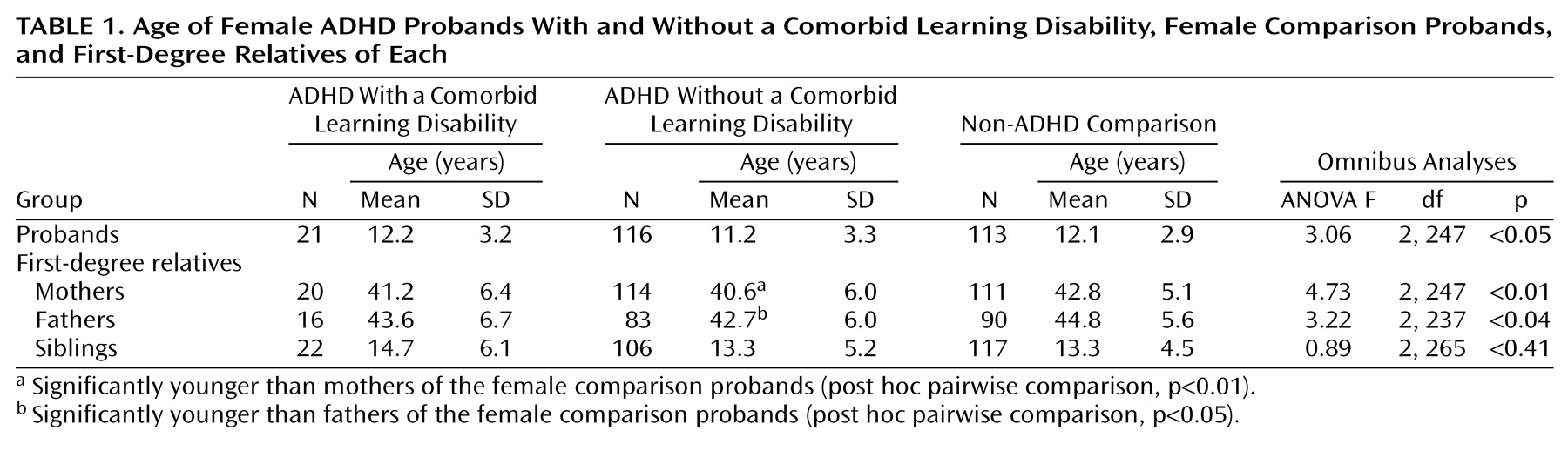
Table 1 shows the number of relatives of each proband group and compares them in terms of age by using a one-way ANOVA. Although the omnibus test suggested a significant difference between the ages of probands, pairwise comparisons showed no statistically significant differences between groups. No group differences emerged when the ages of siblings were compared. Both mothers and fathers of ADHD probands without a learning disability were significantly younger than those of the comparison probands. However, further analyses were not corrected for parental age, since the difference between these groups was quite small (approximately 2 years), and all parents had passed through the age of risk for both ADHD and learning disabilities. The three proband groups did not differ in terms of parental socioeconomic status (ADHD with comorbid learning disability: mean=1.9, SD=0.8; ADHD, no learning disabilities: mean=1.9, SD=1.0; comparison [no ADHD]: mean=1.7, SD=0.8) (χ
2=2.14, df=2, p<0.34).
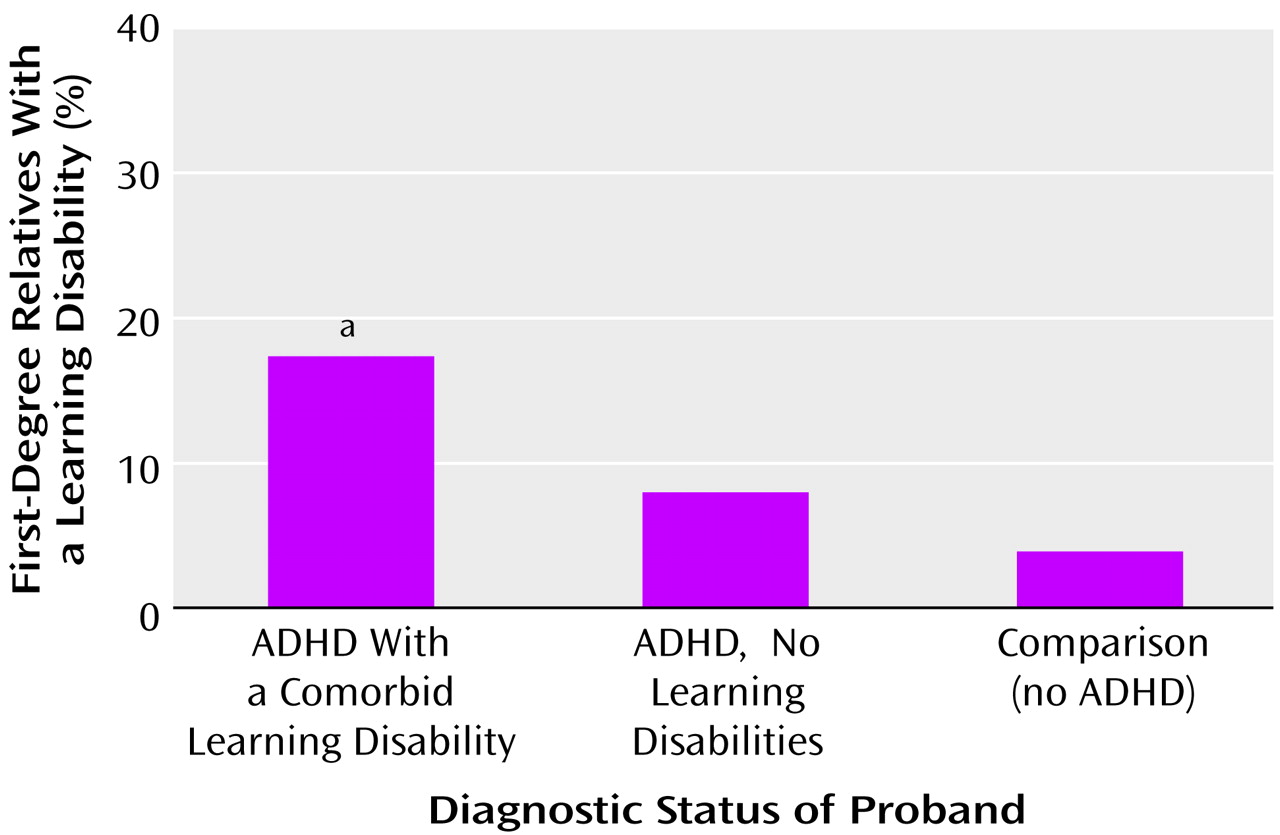
As shown in
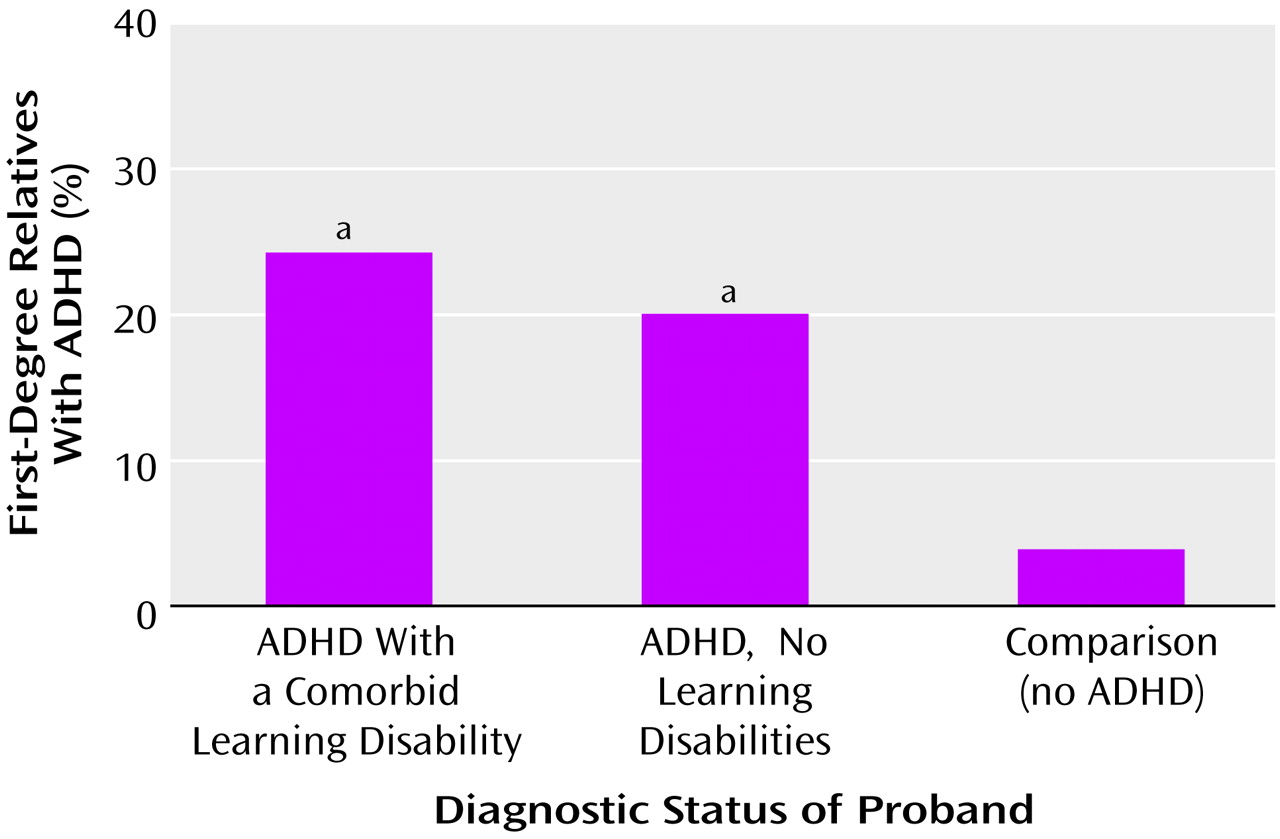
Figure 1, analyses revealed that learning disabilities were significantly overrepresented among the first-degree relatives of girls with ADHD and a comorbid learning disability (17%) compared to relatives of ADHD probands without a learning disability (8%) and relatives of comparison probands (4%). In contrast, as seen in
Figure 2, ADHD was equally familial in the ADHD probands either with or without a learning disability (24% and 20%, respectively, versus 4% in comparison subjects).
To examine whether the relationship between ADHD and learning disabilities was due to cosegregation, we examined the 58 relatives of the female ADHD probands with a comorbid learning disability. We compared the 13 relatives with ADHD with the 45 without ADHD to determine if ADHD and learning disabilities were independently transmitted in these families. Relatives with ADHD had a higher rate of learning disabilities than relatives without ADHD (30.8% versus 13.3%). While this difference did not reach statistical significance (Wald χ2=3.71, df=1, p=0.054), the fact that relatives with ADHD were over two times more likely than relatives without ADHD to have a learning disability suggests at least some degree of cosegregation between ADHD and learning disabilities.
Also plausible in accounting for the association between ADHD and learning disabilities is assortative or nonrandom mating between parents. To test for nonrandom mating, we examined associations between ADHD and learning disabilities in the parents of the ADHD probands. Among the 16 mothers with ADHD, 6.3% had husbands with a learning disability compared with 6.0% of the 81 mothers with no history of ADHD (χ2=0.001, df=1, p=0.99). Among the 14 fathers with ADHD, 7.1% had wives with a learning disability compared with 6.0% of the 83 fathers without ADHD (χ2=0.08, df=1, p=0.77). (Of note is that group numbers reflect the fact that these analyses were limited to families from whom we had data available for both parents.) Thus, we found no evidence of nonrandom mating among the current participants.
Discussion
In a familial risk analysis of the association between ADHD and learning disabilities in girls, we found that 1) relatives of ADHD probands either with or without a learning disability had significantly higher rates of ADHD than did relatives of comparison subjects; 2) the risk of learning disabilities was higher only among relatives of the ADHD probands with a learning disability; 3) a strong (although statistically nonsignificant) pattern of cosegregation between ADHD and learning disabilities emerged; and 4) there was no evidence of nonrandom mating between parents with ADHD and learning disabilities. When these findings are compared to patterns predicted by various models of transmission, they are most consistent with the hypothesis that, in girls, ADHD and learning disabilities are distinct disorders.
Although some researchers have suggested that ADHD and learning disabilities may be different manifestations of the same underlying condition
(29,
30), our data were not consistent with this hypothesis. If learning disabilities were secondary to the cognitive impairments associated with ADHD, we should not have found familial transmission of learning disabilities in the families of girls with ADHD and a learning disability. Yet, these relatives had a significantly higher rate of learning disabilities (17%) than did relatives of the ADHD probands without a learning disability and the comparison probands (8% and 4%, respectively). If ADHD with a learning disability represented a more severe familial form of ADHD, we should have found a higher risk for both ADHD and learning disabilities among relatives of ADHD probands with a learning disability than in relatives of ADHD probands without a learning disability. However, the risk for ADHD in these groups was comparable. Furthermore, if ADHD probands either with or without a learning disability shared common familial etiologic factors but differed because of environmental triggers, we should have found similar rates of ADHD and learning disabilities in the relatives of both subgroups. Instead, we found more learning disabilities among the relatives of girls with ADHD and a learning disability.
We also investigated two explanations for why learning disabilities were concentrated among relatives of ADHD probands with a learning disability
(6). First, we examined whether ADHD with a learning disability was a distinct familial subtype. If so, then ADHD and learning disabilities should have cosegregated in relatives of girls with ADHD and a learning disability (i.e., we should have found significant comorbidity between ADHD and learning disabilities among relatives of this group). Relatives of the girls with ADHD and a learning disability who themselves had ADHD had over twice the rate of learning disabilities than did relatives without ADHD. This finding suggests cosegregation; however, the difference in the rate of learning disabilities between the ADHD and non-ADHD relatives did not reach statistical significance, most likely because of low statistical power. Thus, while these results raise the possibility that ADHD with a learning disability is a distinct familial subtype, this hypothesis cannot be confirmed by the current data.
Second, we examined the possibility that nonrandom, or assortative, mating accounted for the comorbidity between ADHD and learning disabilities. However, fathers with ADHD were no more likely to have wives with a learning disability than were fathers without ADHD, and mothers with ADHD were no more likely to have husbands with a learning disability than were mothers without ADHD. Thus, results did not support our hypothesis that we would find evidence for nonrandom mating between parents with ADHD and learning disabilities.
Results of the current study of girls showed similarities as well as differences to our previous study of boys, which used an identical design
(3). Both studies found an excess of learning disabilities only among relatives of ADHD probands with a learning disability, suggesting that ADHD and learning disabilities are distinct disorders. However, the two studies differed in terms of the mechanisms that seem to explain the comorbidity of ADHD and learning disabilities: data from the study of boys pointed to nonrandom mating, whereas data from the current study raise the possibility that ADHD with a learning disability is a distinct familial subtype. Although further work is needed to explore this issue, it may be that the comorbid condition in girls has a more biological substrate than in boys.
It is unclear why we did not find evidence of assortative mating in the current study of girls. Since assortative mating is a social/cultural phenomenon, it is possible that the discrepancy across studies is due to a cohort effect. It is also possible that our initial finding of assortative mating in the parents of boys was spurious. It is noteworthy, however, that other evidence points to gender differences in the comorbidity rate of ADHD and learning disabilities. For example, overall rates of comorbidity with learning disabilities were different across male and female probands. In a study of girls
(12), 16% of ADHD probands and 7% of comparison subjects met criteria for a learning disability in either reading or math, whereas in the study of boys
(31), the rates were 30.1% versus 10.4%, respectively. These conclusions must, however, be tempered by the fact that these studies involved two different cohorts of children. Further work comparing male and female subjects directly is needed to confirm the extent of gender differences in the comorbidity of ADHD and learning disabilities.
Support for our finding that ADHD and learning disabilities are distinct conditions can be found in the literature. Several studies have shown separable neuropsychological deficits in individuals with ADHD and learning disabilities
(1,
5,
32). To our knowledge, no other family studies to date have addressed the relationship between ADHD and learning disabilities in female subjects. However, three twin studies
(8,
33,
34) have examined the comorbidity of ADHD and learning disabilities in combined male and female groups. Results of two of these studies also support the hypothesis that ADHD and learning disabilities are distinct conditions
(8,
33), but they did not specifically examine the influence of gender. In the third study
(34), the relationship between learning disabilities and the inattentive symptoms of ADHD showed evidence of genetic mediation, while the relationship of learning disabilities and hyperactive/impulsive symptoms did not. Yet, no statistically significant effect of gender was found. The current study adds to these findings because it examined a large group of girls with ADHD and used direct assessment of parents which, unlike classical twin studies, allows for an estimation of the effects of nonrandom mating.
Our results must be interpreted in the context of certain design limitations. Since we did not have a comparison group of learning-disabled probands without ADHD, further work is needed to extend our results to youth without ADHD. Because subjects were predominantly Caucasian (91%), our results may not generalize to other ethnic groups. Since the study groups consisted of referred youth, we also do not know whether our results will generalize to community samples. Although raters were blind to the diagnosis of the probands, parents were not. It is therefore possible that this knowledge may have increased the likelihood of their reporting ADHD symptoms.
In addition, our definition of a learning disability was based on a limited amount of psychoeducational data. The degree to which our measures would generalize to the results of a comprehensive psychoeducational assessment is a matter for further research. Nevertheless, our definition of a learning disability was not idiosyncratic. It has been suggested and used by others for at least a decade
(21,
22). Furthermore, when we followed subjects from our family study of boys longitudinally, probands with a comorbid learning disability had more school failure than did boys without a learning disability 4 years later
(35), suggesting that our definition of learning disabilities has predictive validity.
Finally, because of limited statistical power, we were not able to examine the transmission of arithmetic and reading disabilities separately. Yet, Knopik and DeFries
(36) have found evidence for shared genetic etiology between math and reading difficulties. Furthermore, our finding of independent transmission of ADHD and learning disabilities was consistent with findings from twin studies that have examined ADHD and reading disability
(8) and spelling disability
(33).
Despite these limitations, the current study extends previous findings regarding the comorbidity of ADHD and learning disabilities to female subjects by using data from the largest study of girls with ADHD to date. In sum, our results support the hypothesis that ADHD and learning disabilities are independent conditions and raise the possibility that ADHD with a comorbid learning disability is a distinct familial subtype. Despite the large literature on ADHD, much of what we know about this disorder derives from studies of boys
(10). Thus, results of the current study emphasize the importance of direct assessments of ADHD and related conditions in girls.